

COPD Exacerbation is one of the most common reasons for admission to the hospital.
Here's a streamlined approach (with some key pearls and literature) to make admitting these patients second nature.
- Thread -
#MedTwitter #MedEd #FOAMEd #tipsfornewdocs #POCM
1/19
Here's a streamlined approach (with some key pearls and literature) to make admitting these patients second nature.
- Thread -
#MedTwitter #MedEd #FOAMEd #tipsfornewdocs #POCM
1/19
Check out these @pointofcaremed digital resources for AECOPD:
Online Template:
pointofcaremedicine.com
Podcast:
anchor.fm
YouTube Video:
youtu.be
@GlassHealthHQ:
glass.health
2/19
Online Template:
pointofcaremedicine.com
Podcast:
anchor.fm
YouTube Video:
youtu.be
@GlassHealthHQ:
glass.health
2/19
AECOPD is a clinical diagnosis and is broadly defined as a worsening of respiratory symptoms in a COPD patient necessitating further treatment.
Cardinal Symptoms:
- dyspnea
- increased freq and severity of cough
- increased volume/purulence of sputum
3/19
Cardinal Symptoms:
- dyspnea
- increased freq and severity of cough
- increased volume/purulence of sputum
3/19
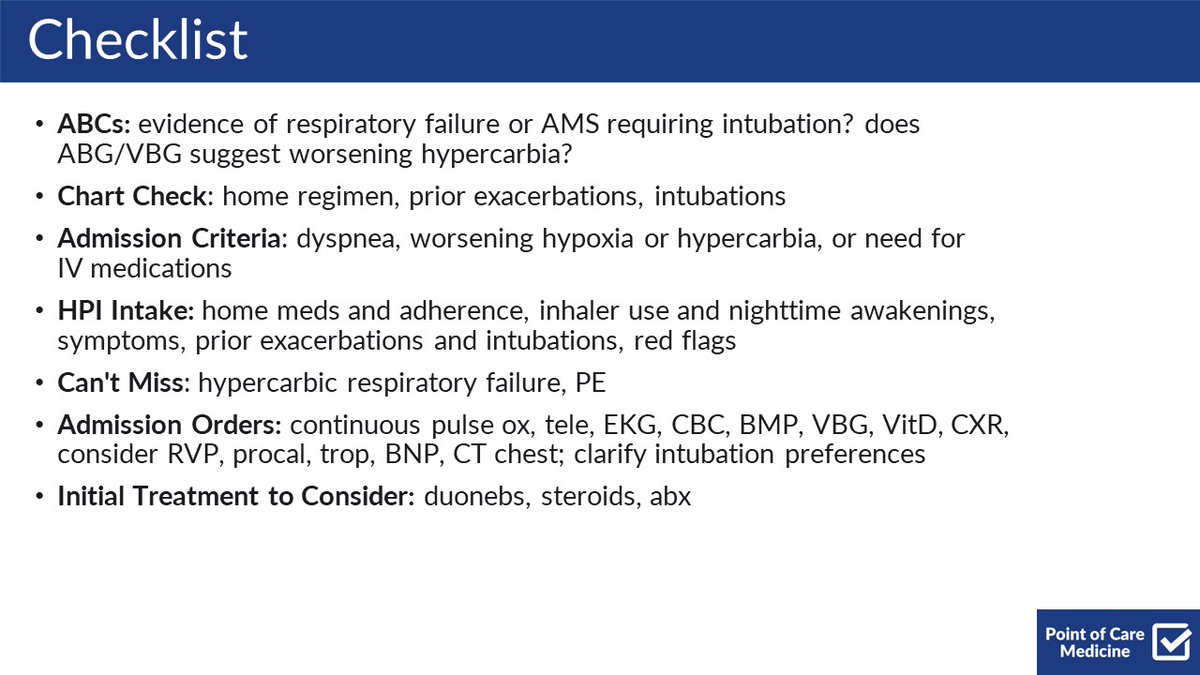
Here's a checklist to use when admitting a patient with AECOPD.
Some key things to remember:
- Chart Check - home med fills, prior exacerbations, and intubations
- Can't Miss - respiratory failure and PE
- Admission orders - include VitD, RVP, steroids, abx if needed
4/19
Some key things to remember:
- Chart Check - home med fills, prior exacerbations, and intubations
- Can't Miss - respiratory failure and PE
- Admission orders - include VitD, RVP, steroids, abx if needed
4/19
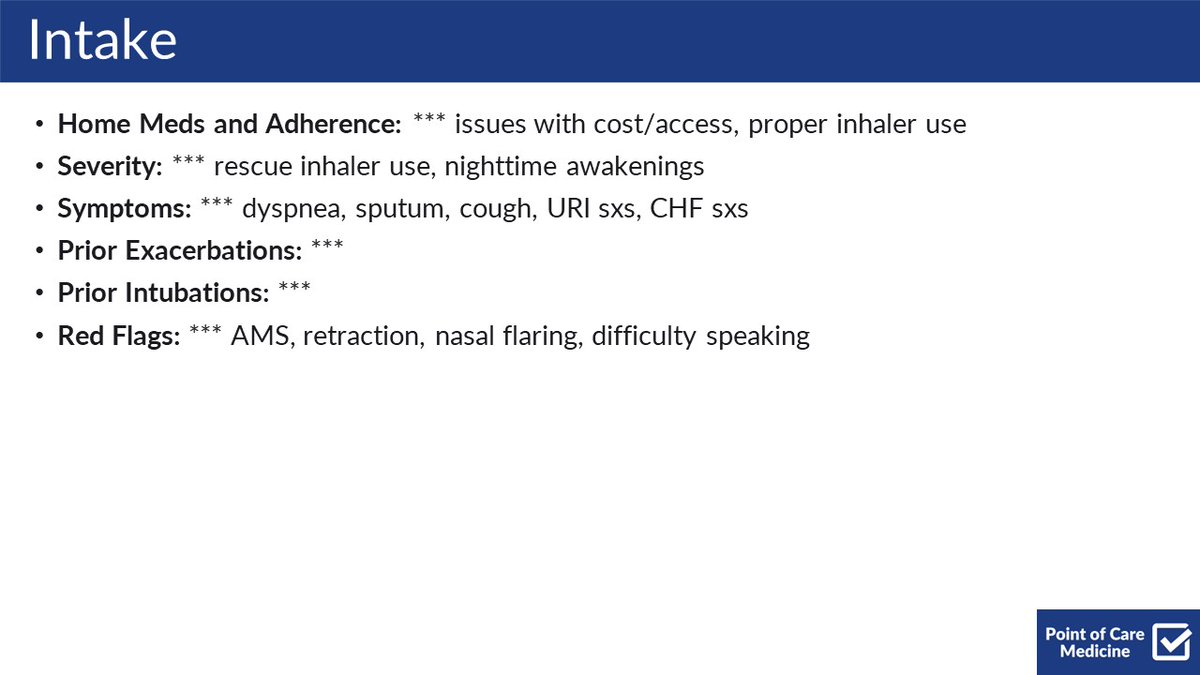
Here is the most pertinent info to collect for your HPI.
- Home meds - understand issues with adherence/access, and ensure the patient demonstrates proper inhaler use
- Symptoms - dyspnea, sputum, cough, URI sxs, CHF sxs
- Trigger - sick contacts, missed meds, etc.
5/19
- Home meds - understand issues with adherence/access, and ensure the patient demonstrates proper inhaler use
- Symptoms - dyspnea, sputum, cough, URI sxs, CHF sxs
- Trigger - sick contacts, missed meds, etc.
5/19
For the physical exam, focus on:
- Increased WOB: tachypnea, nasal flaring, retraction, tripoding, pursed lips, difficulty speaking, etc
- AMS
- Lung sounds: wheezing, rhonchi, rales
- Volume exam (JVP, LE edema, POCUS)
- e/o DVT (leg swellingg, erythema, pain)
6/19
- Increased WOB: tachypnea, nasal flaring, retraction, tripoding, pursed lips, difficulty speaking, etc
- AMS
- Lung sounds: wheezing, rhonchi, rales
- Volume exam (JVP, LE edema, POCUS)
- e/o DVT (leg swellingg, erythema, pain)
6/19
Your DDx should include:
- CHF - volume exam, BNP
- PNA - WBC, RVP, CXR
- PTX - CXR
- PE - D-dimer, CTPE (if either indicated)
7/19
- CHF - volume exam, BNP
- PNA - WBC, RVP, CXR
- PTX - CXR
- PE - D-dimer, CTPE (if either indicated)
7/19
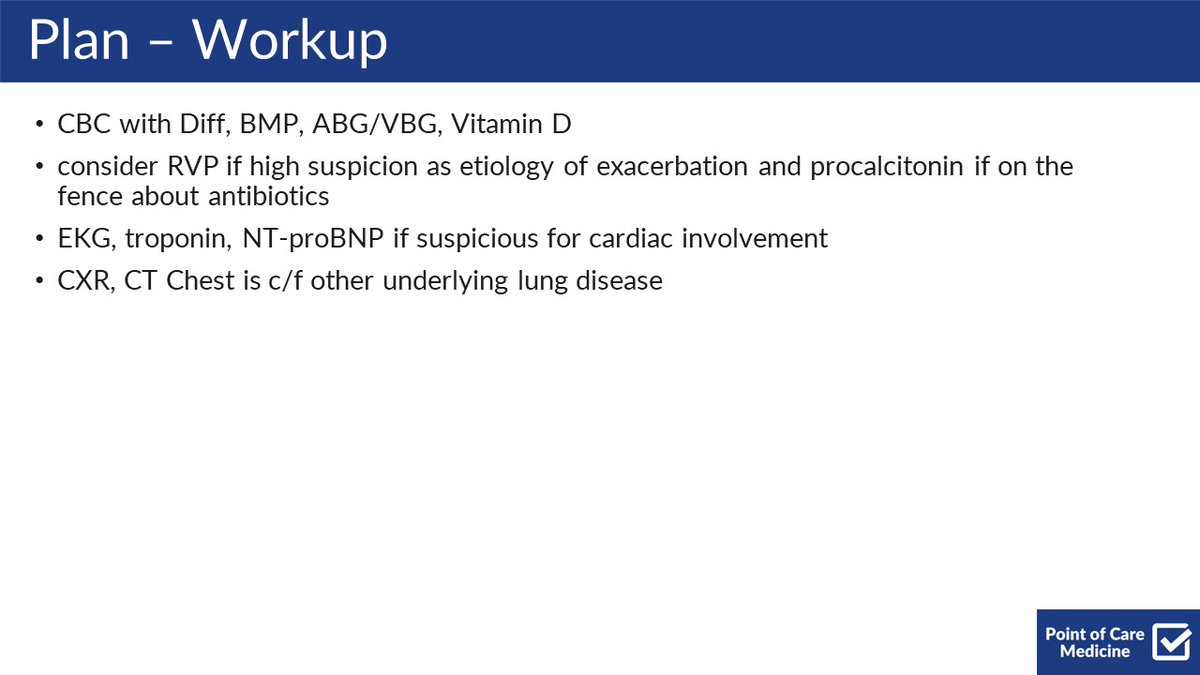
Here is a sample workup to include in your plan:
Some notes:
- RVP and procalcitonin can be useful if you are not sure about antibiotics, though they are not necessarily validated for that purpose
- VBG will likely show chronic hypercarbia and may not be useful
8/19
Some notes:
- RVP and procalcitonin can be useful if you are not sure about antibiotics, though they are not necessarily validated for that purpose
- VBG will likely show chronic hypercarbia and may not be useful
8/19
Treatment is based around:
- Bronchodilators - albuterol and ipratropium Q4-6 standing with albuterol q2 PRN
- Steroids - PO pred 40mg for 5 days; IV methylpred if severe
- Abx: azithro most commonly used, but consider CTX or levoflox if c/f PNA or pip-tazo if c/f PsA
9/19
- Bronchodilators - albuterol and ipratropium Q4-6 standing with albuterol q2 PRN
- Steroids - PO pred 40mg for 5 days; IV methylpred if severe
- Abx: azithro most commonly used, but consider CTX or levoflox if c/f PNA or pip-tazo if c/f PsA
9/19
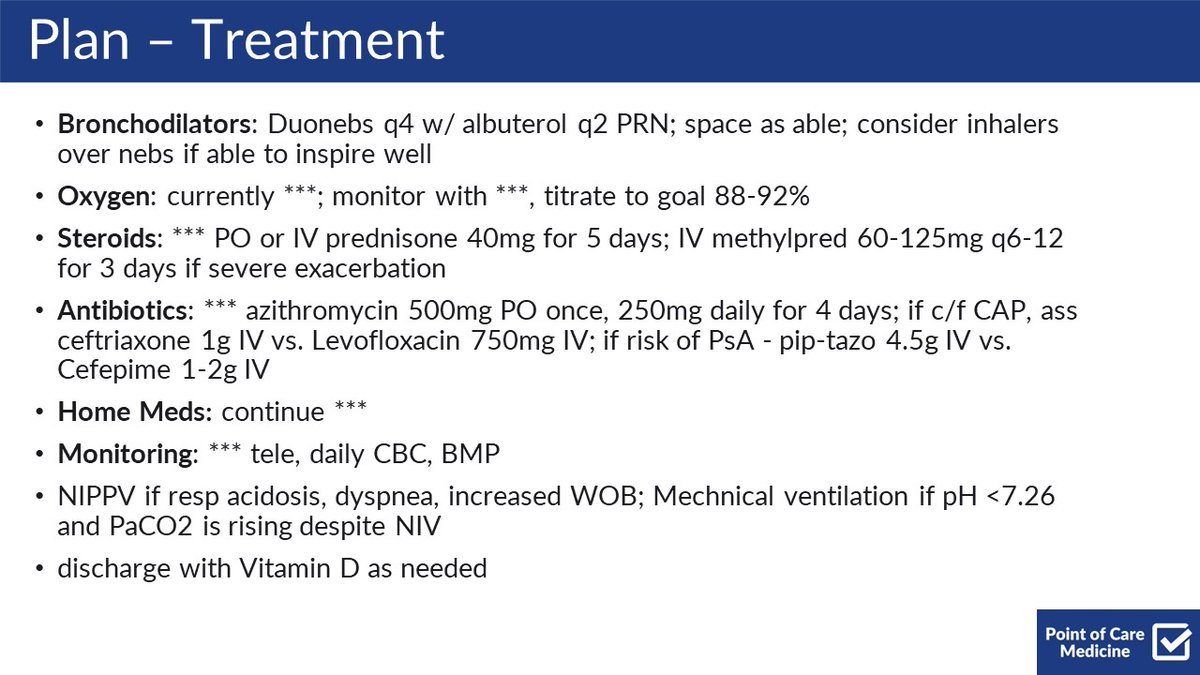
NIPPV is almost always worth trialing before intubation.
That being said, if the patient is crashing or has worsening hypercarbia or pH despite these measures, you should not delay intubation.
10/19
That being said, if the patient is crashing or has worsening hypercarbia or pH despite these measures, you should not delay intubation.
10/19
Pearl #1
Home O2 (if SpO2 <88%) and quitting smoking are the only things that decrease mortality in the outpatient setting
11/19
Home O2 (if SpO2 <88%) and quitting smoking are the only things that decrease mortality in the outpatient setting
11/19
BUT
Hyperoxia leads to worse outcomes!
Likely due to worsening hypercarbia via:
- The Haldane effect
- Improper pulmonary vasoconstriction --> V/Q mismatch
NOT due to reduced respiratory drive (which seems to be what we were all taught)
ncbi.nlm.nih.gov
12/19
Hyperoxia leads to worse outcomes!
Likely due to worsening hypercarbia via:
- The Haldane effect
- Improper pulmonary vasoconstriction --> V/Q mismatch
NOT due to reduced respiratory drive (which seems to be what we were all taught)
ncbi.nlm.nih.gov
12/19
Pearl #2
Cochrane Analysis: somewhat favors nebs over inhalers in AECOPD, but inhalers deliver a more potent dose, are cheaper, less aerosolizing, and more portable.
Start with nebs, then switch to inhalers - an opportunity for inhaler teaching!
cochrane.org
13/19
Cochrane Analysis: somewhat favors nebs over inhalers in AECOPD, but inhalers deliver a more potent dose, are cheaper, less aerosolizing, and more portable.
Start with nebs, then switch to inhalers - an opportunity for inhaler teaching!
cochrane.org
13/19
Pearl #3
You should use PO steroids if the patient can tolerate it
60mg PO was non-inferior to 60mg IV prednisolone (LOS, treatment failure)
(Chest, 2007) pubmed.ncbi.nlm.nih.gov
14/19
You should use PO steroids if the patient can tolerate it
60mg PO was non-inferior to 60mg IV prednisolone (LOS, treatment failure)
(Chest, 2007) pubmed.ncbi.nlm.nih.gov
14/19
Pearl #4
REDUCE Trial
5 days of steroids is enough
5 days of PO steroids was non-inferior to 14 days (six-month re-admissions)
pubmed.ncbi.nlm.nih.gov
15/19
REDUCE Trial
5 days of steroids is enough
5 days of PO steroids was non-inferior to 14 days (six-month re-admissions)
pubmed.ncbi.nlm.nih.gov
15/19
Pearl #5
Vitamin D supplementation can help reduce mod/severe exacerbations if baseline 25(OH) levels <25.
pubmed.ncbi.nlm.nih.gov
16/19
Vitamin D supplementation can help reduce mod/severe exacerbations if baseline 25(OH) levels <25.
pubmed.ncbi.nlm.nih.gov
16/19
Pearl #6
There has been increasing attention on disparities inherent in pulse oximeters and the effect of occult hypoxemia, which is 3x more prevalent in black patients when compared to white patients.
More here:
nejm.org
jamanetwork.com
17/19
There has been increasing attention on disparities inherent in pulse oximeters and the effect of occult hypoxemia, which is 3x more prevalent in black patients when compared to white patients.
More here:
nejm.org
jamanetwork.com
17/19
Here are some great resources:
Shoutout to @thecurbsiders, @COREIMpodcast, @runthelistpod for amazing COPD-related content.
use-inhalers.com is also amazing for reviewing how to properly use different inhalers so you can make sure your patients are doing it right!
18/19
Shoutout to @thecurbsiders, @COREIMpodcast, @runthelistpod for amazing COPD-related content.
use-inhalers.com is also amazing for reviewing how to properly use different inhalers so you can make sure your patients are doing it right!
18/19
If you remember nothing else:
- Clinical Dx - dyspnea, cough, sputum
- DDx for hypoxia and resp distress includes CHF, PNA, PTX, PE
- Most common etiology is a viral infection
- Tx - duonebs, steroids, abx
- Trial NIPPV if needed, but don't delay intubation
19/19
- Clinical Dx - dyspnea, cough, sputum
- DDx for hypoxia and resp distress includes CHF, PNA, PTX, PE
- Most common etiology is a viral infection
- Tx - duonebs, steroids, abx
- Trial NIPPV if needed, but don't delay intubation
19/19
I hope you've found this thread valuable!
Follow me @ROKeefeMD for more clinical threads and pearls.
Like/Retweet the first tweet below if you can:
Follow me @ROKeefeMD for more clinical threads and pearls.
Like/Retweet the first tweet below if you can:
You can read the unrolled version of this thread here: typefully.com
Loading suggestions...