

1/11
A young man presents with hematuria and is found to have these painful skin lesions on physical exam.
A young man presents with hematuria and is found to have these painful skin lesions on physical exam.


2/11
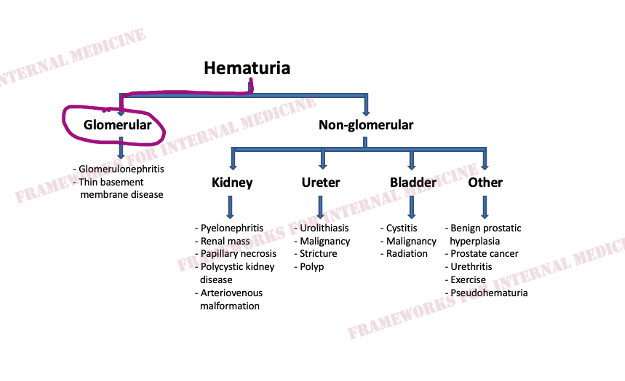
In a patient with hematuria, the first question I always ask is as follows: what is the source of that blood?
Is it glomerular or non-glomerular?
In a patient with hematuria, the first question I always ask is as follows: what is the source of that blood?
Is it glomerular or non-glomerular?

3/11
How can we tell if the bleeding is glomerular or not?
We have to evaluate the urine sediment.
But the eyes can't see what the mind doesn't know. So what are we looking for?
(Images courtesy of @OHSUNephrology.)
How can we tell if the bleeding is glomerular or not?
We have to evaluate the urine sediment.
But the eyes can't see what the mind doesn't know. So what are we looking for?
(Images courtesy of @OHSUNephrology.)

4/11
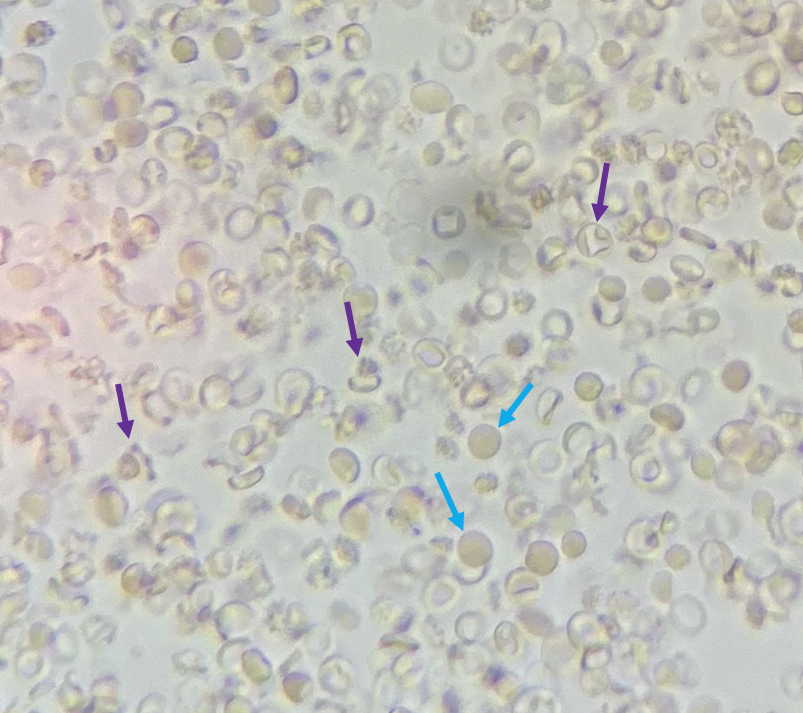
What is the shape of the RBCs? Normal shape (isomorphic)? Or are they abnormal in shape (dysmorphic) because they have squeezed through an inflamed glomerulus?
If we look closely some of these RBCs are indeed dysmorphic (purple arrows). Blue arrows point to isomorphic RBCs.
What is the shape of the RBCs? Normal shape (isomorphic)? Or are they abnormal in shape (dysmorphic) because they have squeezed through an inflamed glomerulus?
If we look closely some of these RBCs are indeed dysmorphic (purple arrows). Blue arrows point to isomorphic RBCs.
5/11
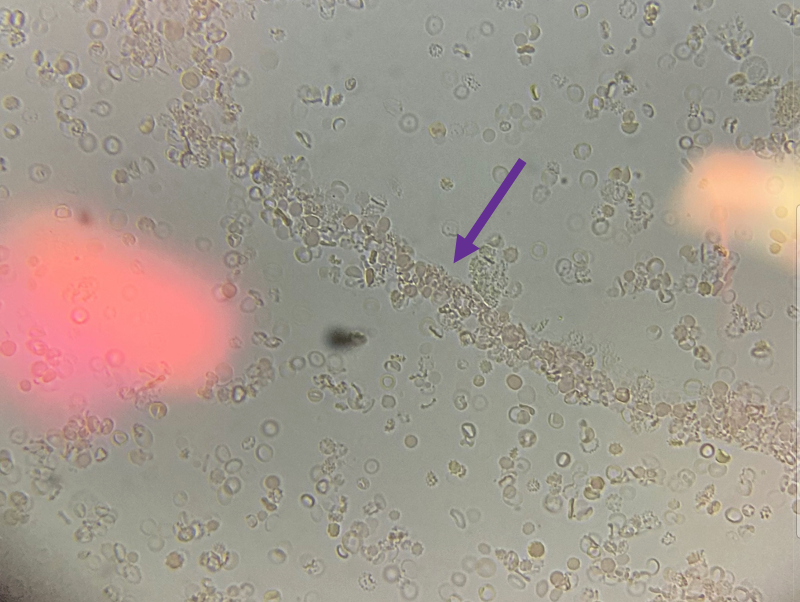
When those RBCs squeeze through the glomerulus they end up in the tubules, where they can form casts.
Check out what @OHSUNephrology found below. That's an RBC cast ! Another clue that our bleeding source is glomerular.
When those RBCs squeeze through the glomerulus they end up in the tubules, where they can form casts.
Check out what @OHSUNephrology found below. That's an RBC cast ! Another clue that our bleeding source is glomerular.
6/11
Our patient has hematuria of glomerular origin.
Our patient has hematuria of glomerular origin.
7/11
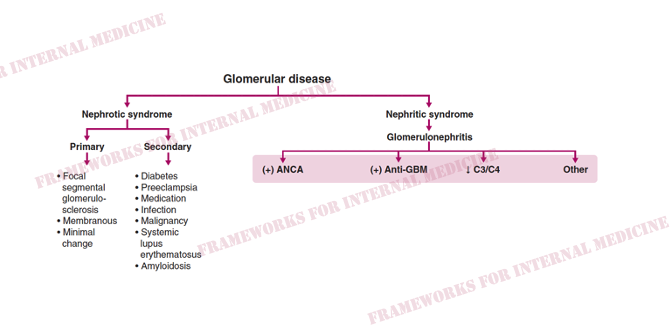
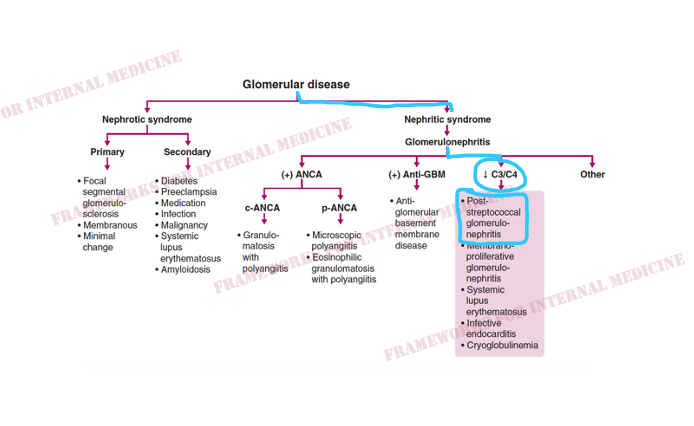
I like to approach GN serologically.
I like to approach GN serologically.
8/11
But instead of just ordering all of those labs simultaneously at a high cost, history and physical exam should guide that workup. Let's revisit the exam. What is this skin lesion?
But instead of just ordering all of those labs simultaneously at a high cost, history and physical exam should guide that workup. Let's revisit the exam. What is this skin lesion?

9/11
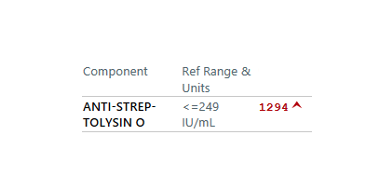
Our derm colleagues come by and confidently diagnose ecthyma. What organism most commonly causes echythma? Streptococcus. Can we connect the dots now?
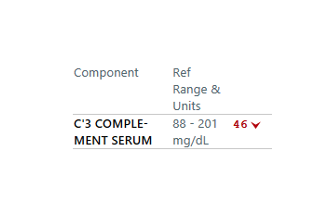
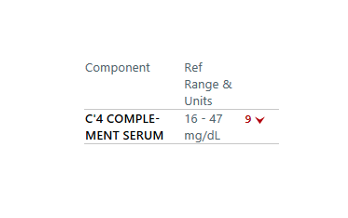
Our hypothesis drives us to order serum complement levels and ASO titers.
Our derm colleagues come by and confidently diagnose ecthyma. What organism most commonly causes echythma? Streptococcus. Can we connect the dots now?
Our hypothesis drives us to order serum complement levels and ASO titers.
10/11
And we have our diagnosis.
And we have our diagnosis.
11/11
This is how I use #FrameworksForInternalMedicine to help me work through cases.
For more: amazon.com
This is how I use #FrameworksForInternalMedicine to help me work through cases.
For more: amazon.com

Loading suggestions...