

🔥Tweetorial: Atypical Anti-Glomerular Basement Membrane Disease
kireports.org @kdjhaveri @purvasharma821 @Yihe28745445 @HofstraKidney #NephTwitter @KIReports
kireports.org @kdjhaveri @purvasharma821 @Yihe28745445 @HofstraKidney #NephTwitter @KIReports
1) Circulating anti-GBM antibodies are directly pathogenic in anti-GBM disease.
However, about 10% of patients with anti-GBM disease do not have circulating anti-
GBM antibodies
However, about 10% of patients with anti-GBM disease do not have circulating anti-
GBM antibodies

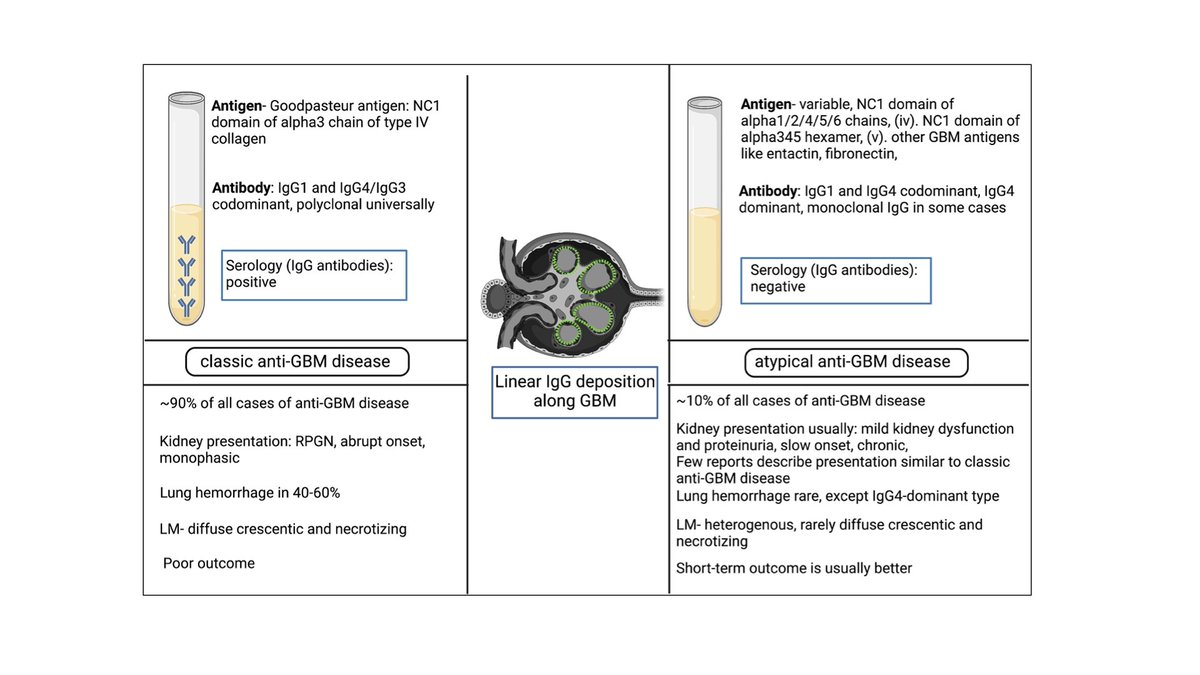
2)Atypical anti-GBM disease is considered when patients have linear IgG deposition along the glomerular basement membrane without anti-GBM antibodies in the circulation. #nephrology #kidney #kidneydisease
3)Atypical anti-GBM disease comprises 8% to 12% of all anti-GBM disease cases. About 2% to 8% of patients with anti-GBM disease have negative serology despite rigorous testing
4)Pathogenesis: (i)different composition of antigen/epitope: a)Antibodies against
the NC1 domain of other alpha chains like alpha1, alpha4, or alpha5 chains of type IV
collagen or to the NC1 domain of alpha345 hexamers, b)Linear epitopes of the
collagenous domain, or C)entactin
the NC1 domain of other alpha chains like alpha1, alpha4, or alpha5 chains of type IV
collagen or to the NC1 domain of alpha345 hexamers, b)Linear epitopes of the
collagenous domain, or C)entactin
5)Pathogenesis: (ii)different affinity of antibodies: a) high-affinity autoantibodies
trapped in the kidneys and present with low titer in circulation, or (b)Autoantibodies could also have a low affinity for the substrate in the assay
trapped in the kidneys and present with low titer in circulation, or (b)Autoantibodies could also have a low affinity for the substrate in the assay
6)Pathogenesis: (iii) different types of antibody: a). the dominance of different IgG subclass
such as IgG4 or IgG1 and frequent presence of IgG2, b) presence of IgA or IgM dominance which is not exactly atypical anti-GBM diseases in terms of clinical/pathological presentation
such as IgG4 or IgG1 and frequent presence of IgG2, b) presence of IgA or IgM dominance which is not exactly atypical anti-GBM diseases in terms of clinical/pathological presentation
7)Modified assays to detect a wide range of antigens or epitopes or antibodies and sensitive techniques like biosensors can unmask circulating anti-GBM antibodies in some cases and should be attempted.
8)Pathology: (i). lack diffuse crescentic and
necrotizing glomerulonephritis, (ii). Light microscopy heterogenous: mesangial and/or endocapillary proliferative GN, MPGN, FSGS, mesangial sclerosis; and glomerular endothelial changes resembling TMA are common
necrotizing glomerulonephritis, (ii). Light microscopy heterogenous: mesangial and/or endocapillary proliferative GN, MPGN, FSGS, mesangial sclerosis; and glomerular endothelial changes resembling TMA are common
9)Monotypic atypical anti-GBM disease: Monotypic Ig deposits along the GBM are increasingly observed to cause a disease pattern similar to atypical anti-GBM. Needs further study to confirm if it is a form of monoclonal gammopathy of renal significance (MGRS)
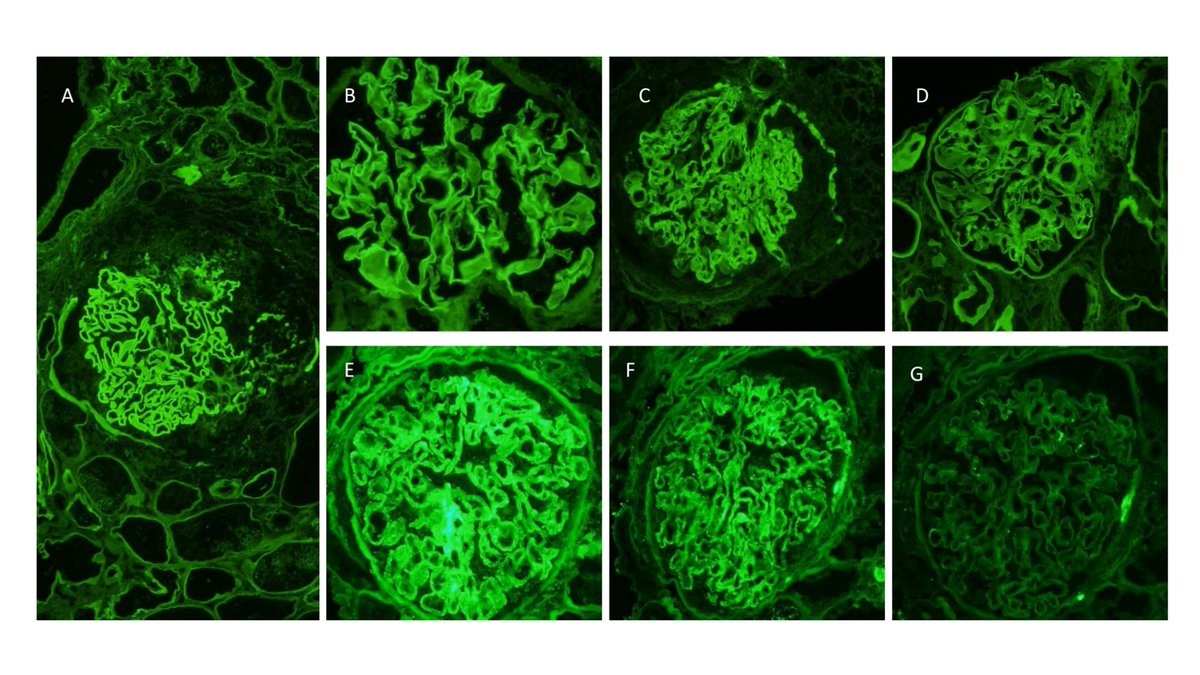
10)Differential diagnoses for linear IgG deposition along GBM: (i)diabetic nephropathy (D)
(ii)monoclonal immunoglobulin deposition disease ("MIDD by IF only") (E-G) and (iii)fibrillary GN (B) (iv) atypical anti-GBM ds (C) (v) classic anti-GBM ds (A)
(ii)monoclonal immunoglobulin deposition disease ("MIDD by IF only") (E-G) and (iii)fibrillary GN (B) (iv) atypical anti-GBM ds (C) (v) classic anti-GBM ds (A)
11)Kidney dysfunction is usually milder and evolves slower than classic anti-GBM disease; however, presentation as RPGN has also been reported. Proteinuria and nephrotic syndrome are more frequent than classic anti-GBM disease.
12)Treatment: is individualized and typically consists of immunosuppressive agents used to treat classic anti-GBM disease or monotherapy with renin-angiotensin-aldosterone blockers
13)Looking forward: A prospective multicenter study on a large cohort of patients with atypical anti-GBM disease would be worthwhile to understand its pathogenesis,clinical course, and outcome.
Loading suggestions...