

Complicated case in this patient with ear pain, fever, and headache
#neurology #ent #neurosurgery #peds #radres #futureradres @ASHNRSociety @TheASNR #MedTwitter
#neurology #ent #neurosurgery #peds #radres #futureradres @ASHNRSociety @TheASNR #MedTwitter
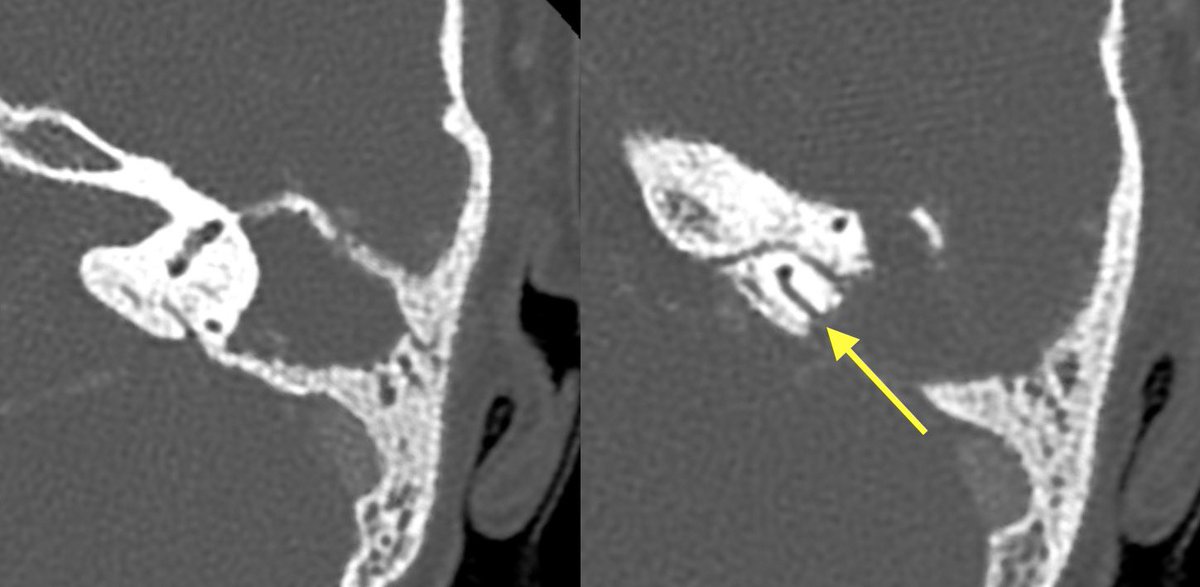
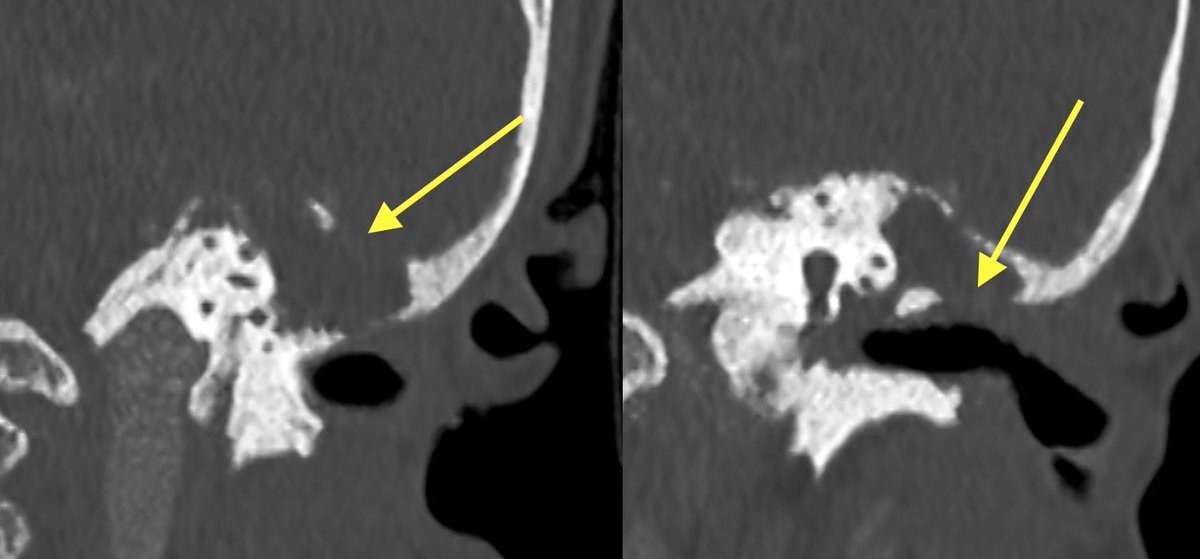
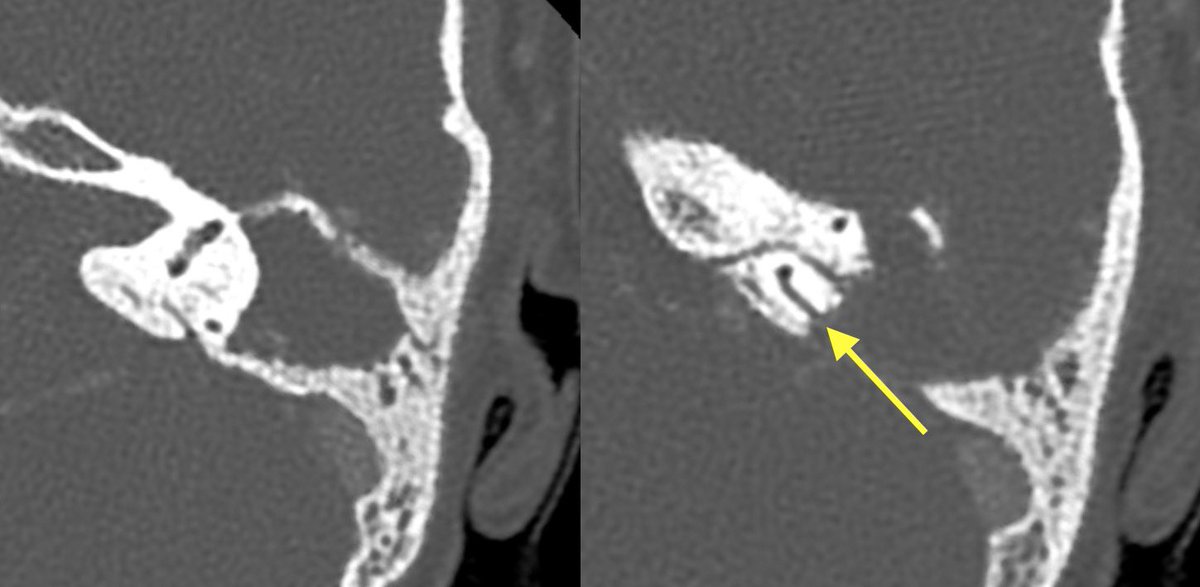
Initial T bone CT:
▶️Coalescence of mastoid air cells
▶️diffuse dehiscence of Tegmen tympani
▶️Middle ear ossicle erosions
▶️dehiscence of the roof of the EAC
▶️dehiscence of semicircular canals and tympanic segment of facial nerve
▶️Coalescence of mastoid air cells
▶️diffuse dehiscence of Tegmen tympani
▶️Middle ear ossicle erosions
▶️dehiscence of the roof of the EAC
▶️dehiscence of semicircular canals and tympanic segment of facial nerve

With findings this extensive it can be difficult to differentiate cholesteatoma from coalescent otomastoiditis
Helpful clues in cholesteatoma
💡 MORE MASS EFFECT (expansion of aditus ad antrum, displacement of middle ear ossicles with enlarged middle ear cavity)
💡 MORE EROSIONS (middle ear ossicles, facial nerve canal, semicircular canals)
💡 More likely to have retracted or ruptured TM
💡 MORE MASS EFFECT (expansion of aditus ad antrum, displacement of middle ear ossicles with enlarged middle ear cavity)
💡 MORE EROSIONS (middle ear ossicles, facial nerve canal, semicircular canals)
💡 More likely to have retracted or ruptured TM
Cholesteatoma was favored in this case given the extent of erosions and lack of significant surrounding inflammatory change. However, symptoms were concerning for superimposed infection and meningitis
LP was done and MR ordered
LP was done and MR ordered
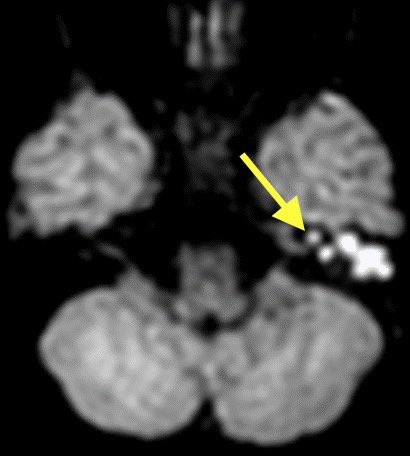
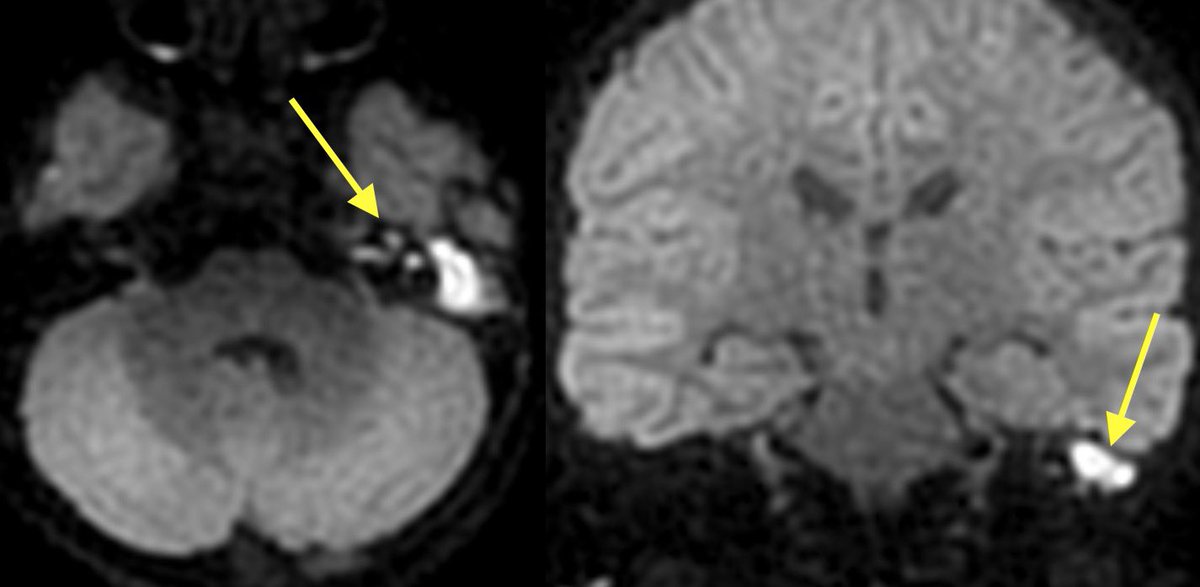
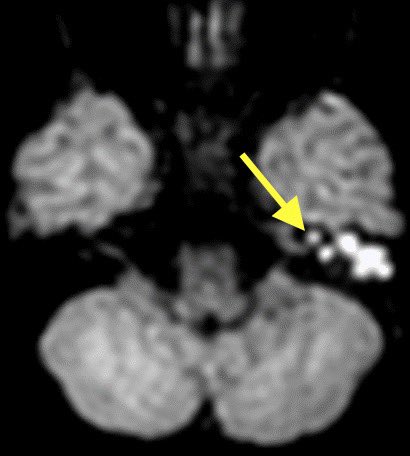
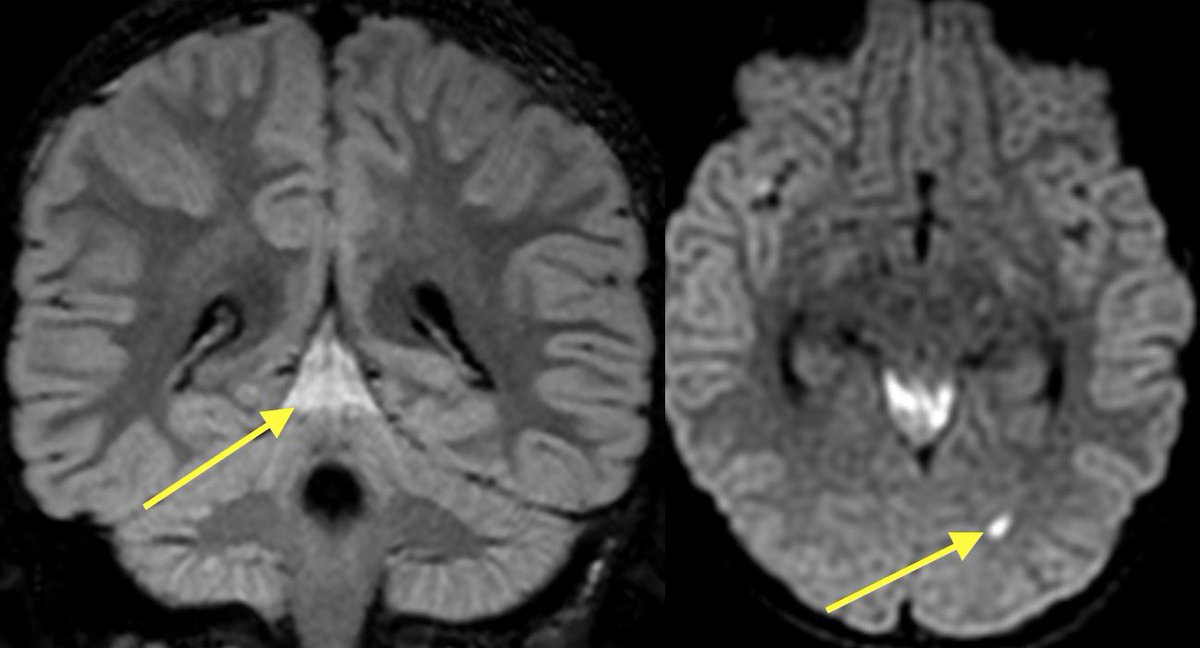
💡 When concerned for cholesteatoma make sure to get the NON ECHO PLANAR DWI to reduce artifact around the T bone which increases sensitivity for cholesteatoma. Cholesteatomas are very bright on DWI (think of them as extracranial epidermoid cysts)
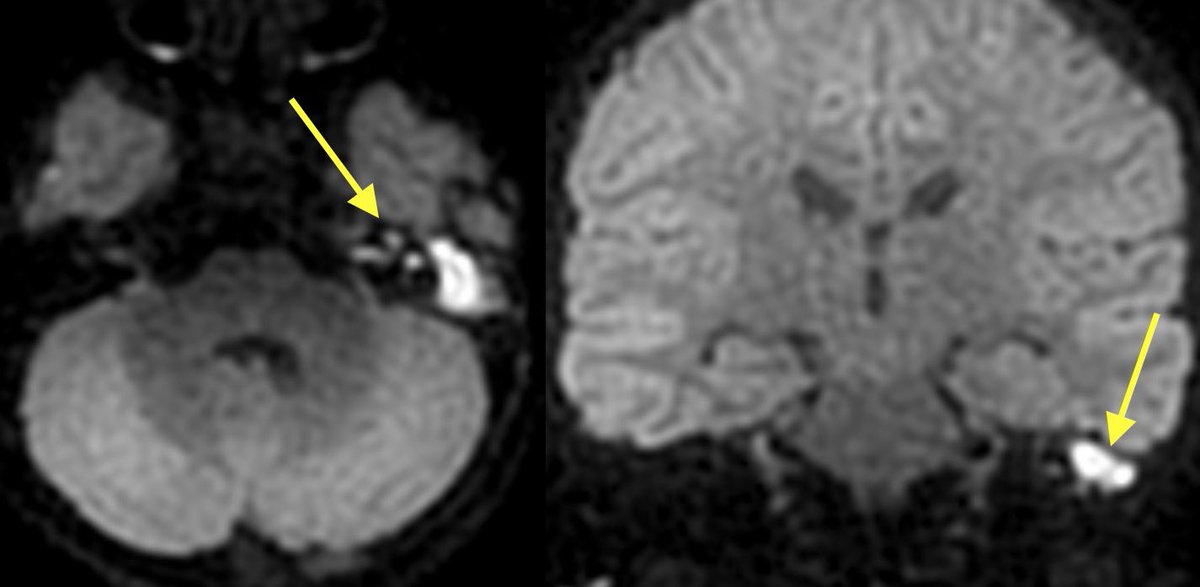
1️⃣DWI shows restricted diffusion of the left mastoid air cells (can be seen in cholesteatoma or purulent mastoiditis)
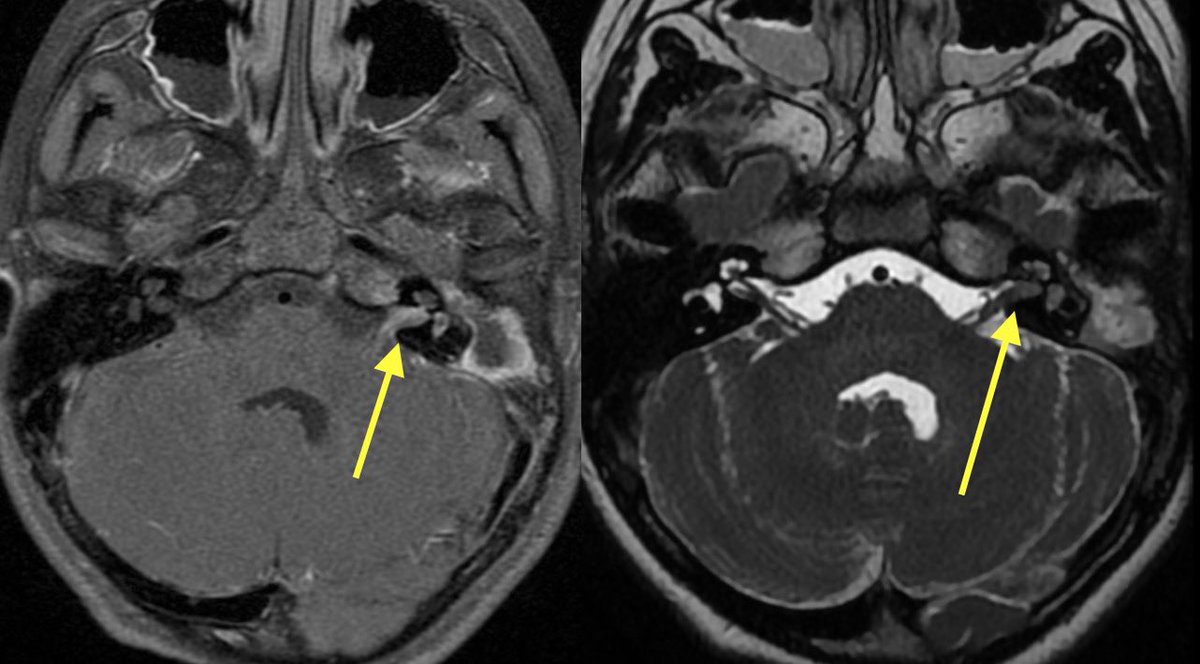
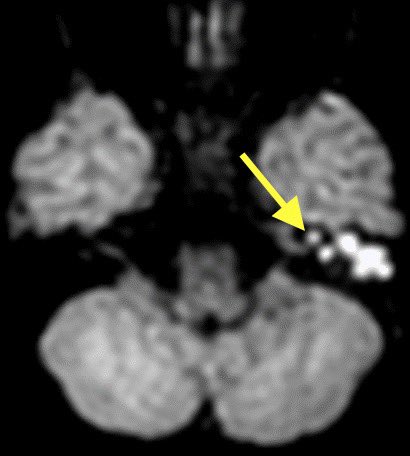
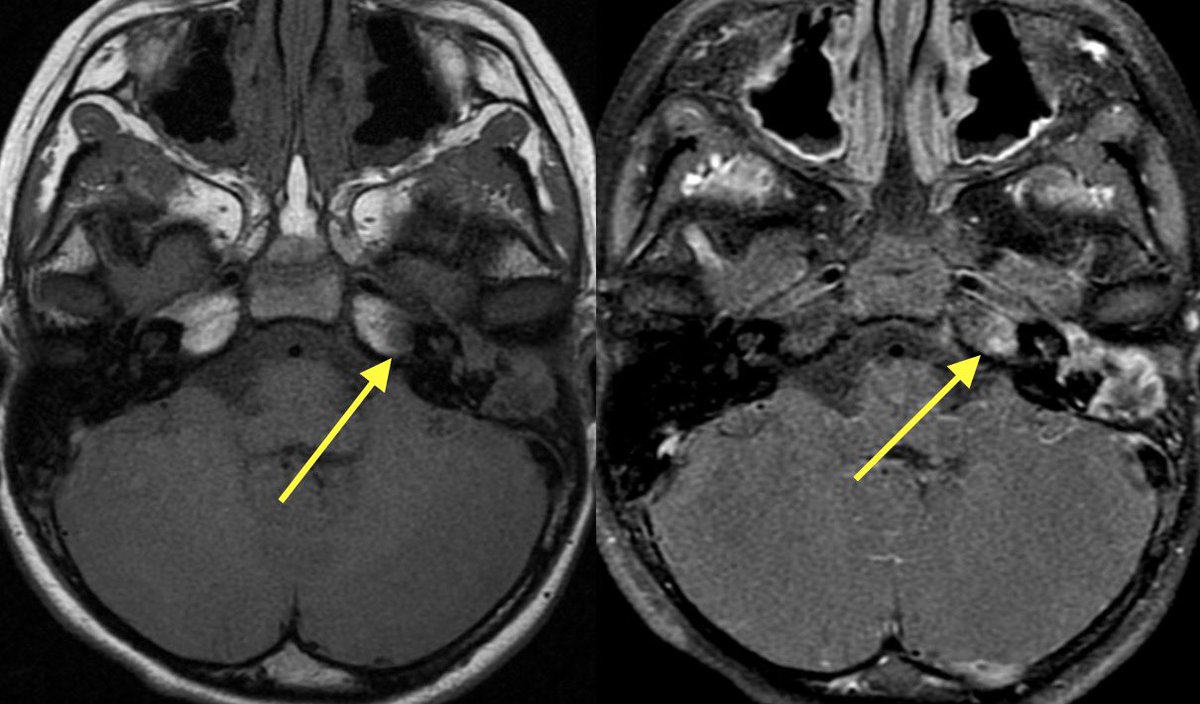
2️⃣However, additional restriction, enhancement, and loss of normal CSF signal in the left IAC was highly suggestive of suppurative Labyrinthitis
2️⃣However, additional restriction, enhancement, and loss of normal CSF signal in the left IAC was highly suggestive of suppurative Labyrinthitis
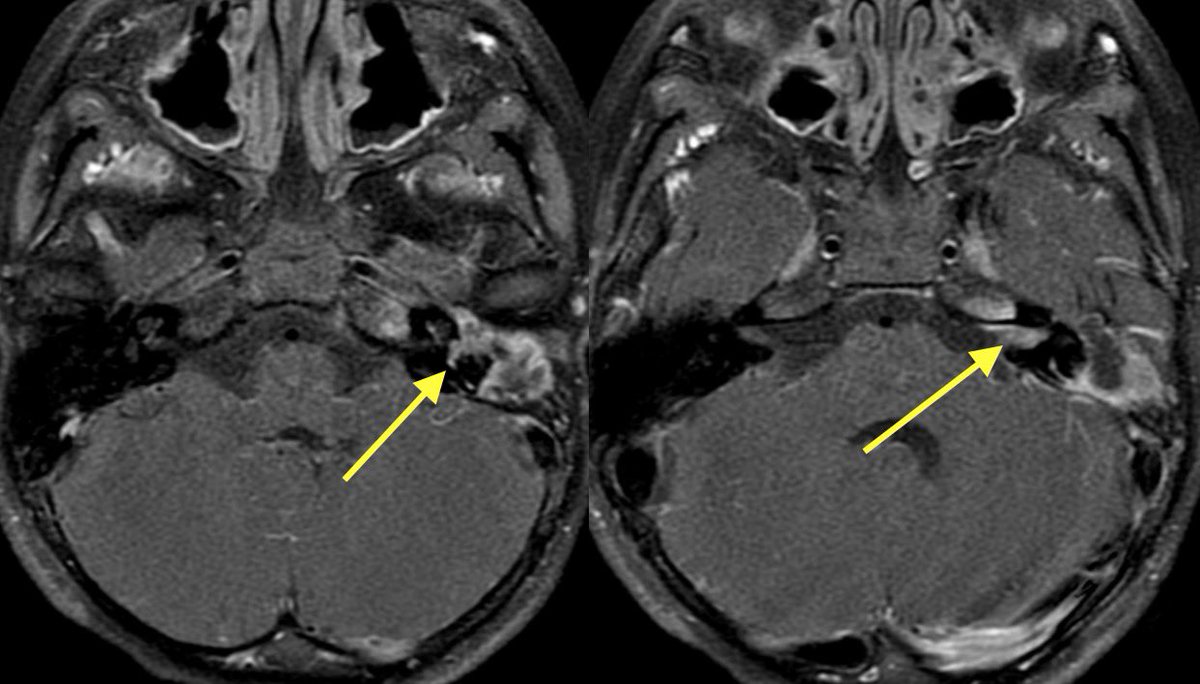
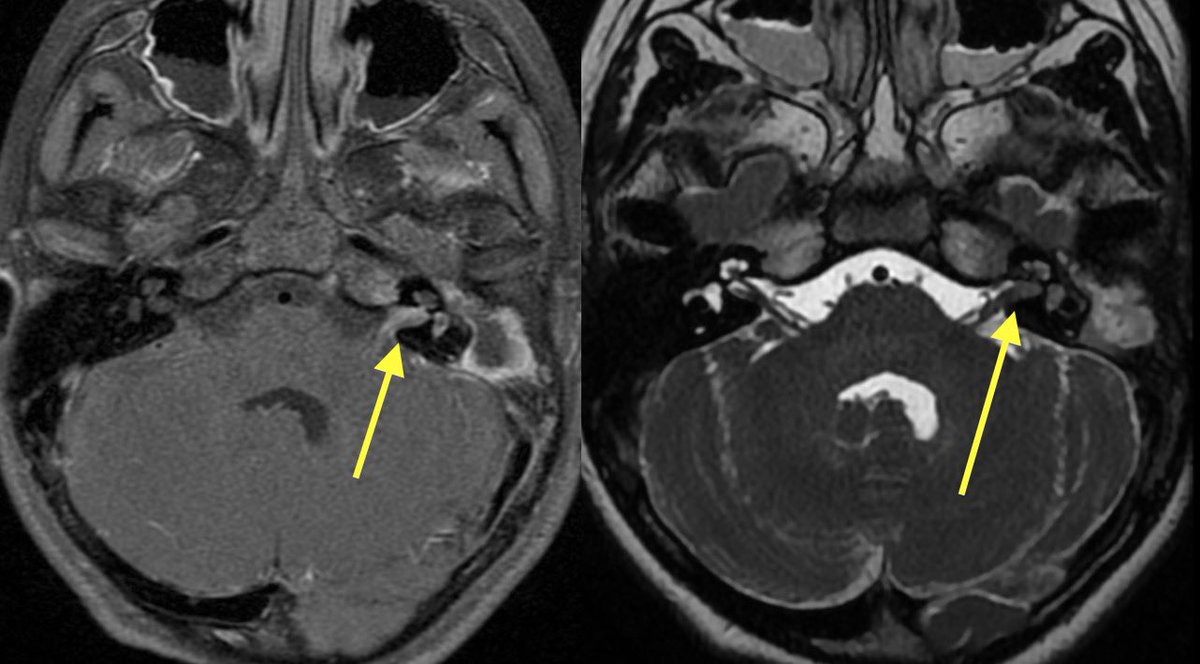
Cholesteatoma with superimposed infection was also complicated by meningitis (seen best at quadrigeminal plate cistern), ventriculitis, skull base osteomyelitis (petrous apicitis) and probably some other itisis that I’m forgetting
Patient developed acute left sided weakness and thus stroke code was activated
💡 Meningitis is a risk factor for stroke
💡 Meningitis can induce vasospasm from arterial irritation (just like SAH)
💡 Can also cause infectious vasculitis
💡 Meningitis is a risk factor for stroke
💡 Meningitis can induce vasospasm from arterial irritation (just like SAH)
💡 Can also cause infectious vasculitis
▶️CT-: Subtle loss of GW in the right caudate nucleus
▶️CTA: Severe spasm of right ICA terminus and MCA and to a lesser degree, the left side as well
▶️CT perfusion: elevated Tmax in the bilateral (right greater than left MCA territories)
▶️CTA: Severe spasm of right ICA terminus and MCA and to a lesser degree, the left side as well
▶️CT perfusion: elevated Tmax in the bilateral (right greater than left MCA territories)
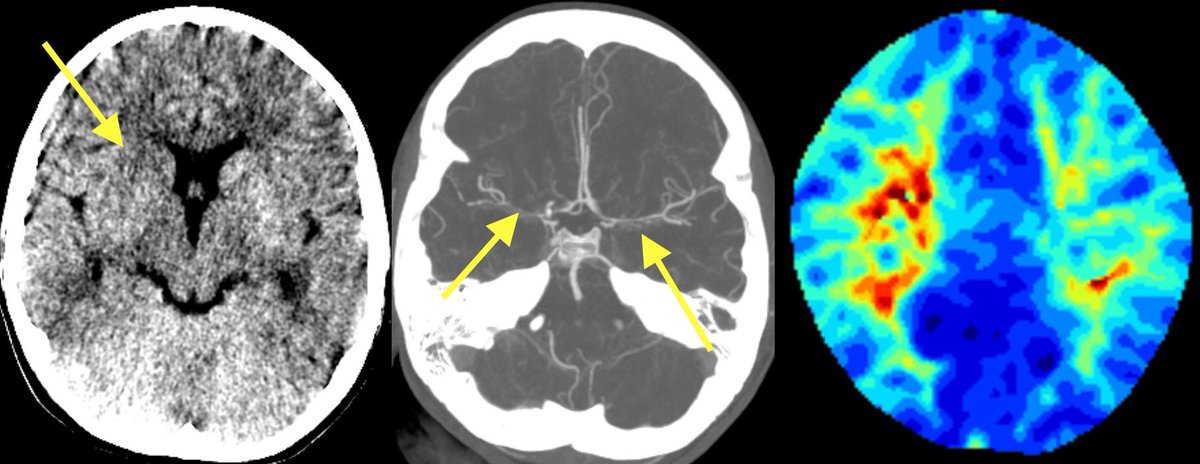
Of note, caution must be taken when interpreting CT perfusion in peds patients if the injection rates are slower than those used in adults (can mess with transit times)
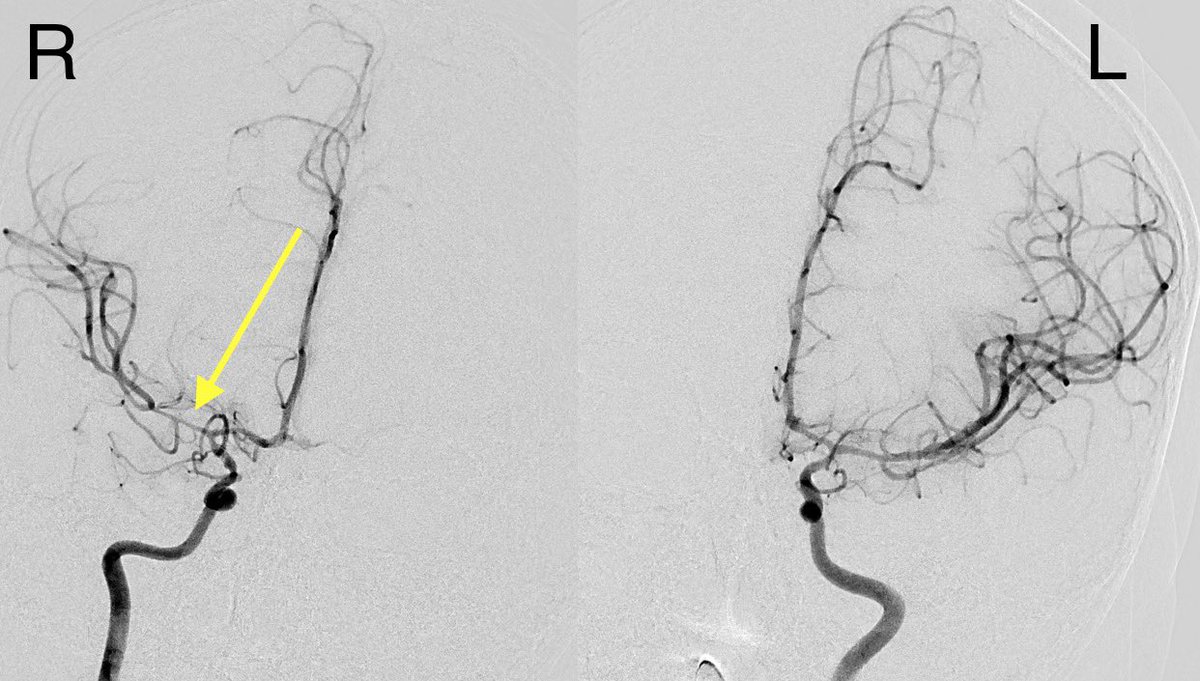
▶️Spasm was confirmed on angio in the right ICA terminus and MCA (greater than left) …treated with verapamil
▶️Spasm was confirmed on angio in the right ICA terminus and MCA (greater than left) …treated with verapamil
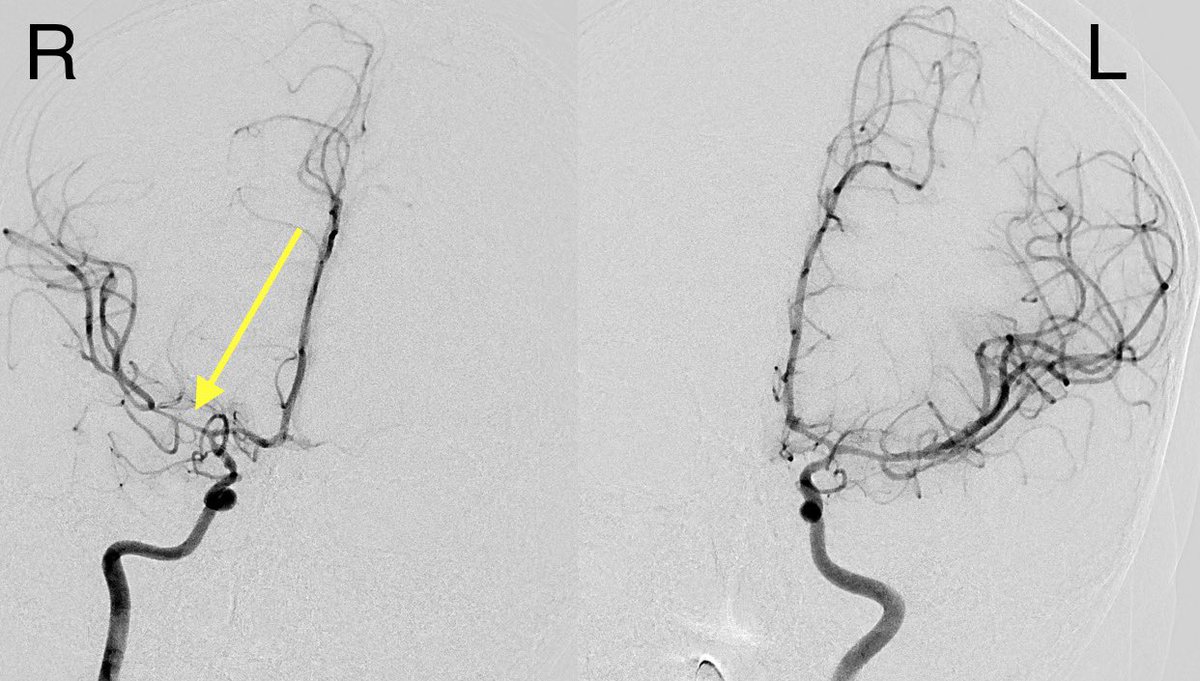
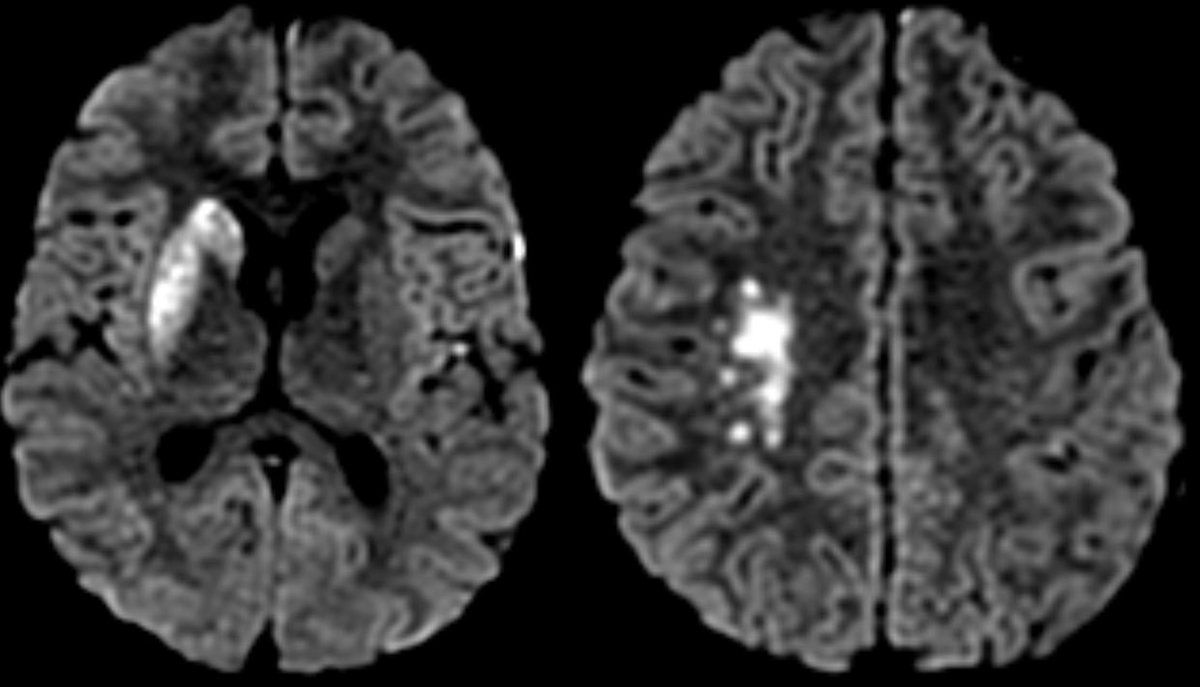
MR shows the extent of the core infarct involving the right BG and MCA-ACA border zone (watershed)
Take home learning points:
💡 Choleastoma typically has more mass effect and erosions than otomastoiditis
💡 make sure to report all areas of dehiscence as it can affect surgical approach
💡 complications of cholesteatoma (infection, labyrinthine fistula, CSF leak, etc.)
💡 Choleastoma typically has more mass effect and erosions than otomastoiditis
💡 make sure to report all areas of dehiscence as it can affect surgical approach
💡 complications of cholesteatoma (infection, labyrinthine fistula, CSF leak, etc.)
💡 Protocol MR with non EP DWI to reduce artifact when concerned for cholesteatoma
💡 look closely for complications as there can be many
💡 Beware of vasospasm or infectious vasculitis in setting of meningitis
💡 CTA MIPS are great for catching spasm, stenosis, vasculitis
💡 look closely for complications as there can be many
💡 Beware of vasospasm or infectious vasculitis in setting of meningitis
💡 CTA MIPS are great for catching spasm, stenosis, vasculitis
Final diagnosis: confirmed following resection complicated choleastoma 🦻🧠
Loading suggestions...