

🫠 Approach to Hypotension 🫠
Recent ICU shifts = newfound appreciation for this clinical dilemma.
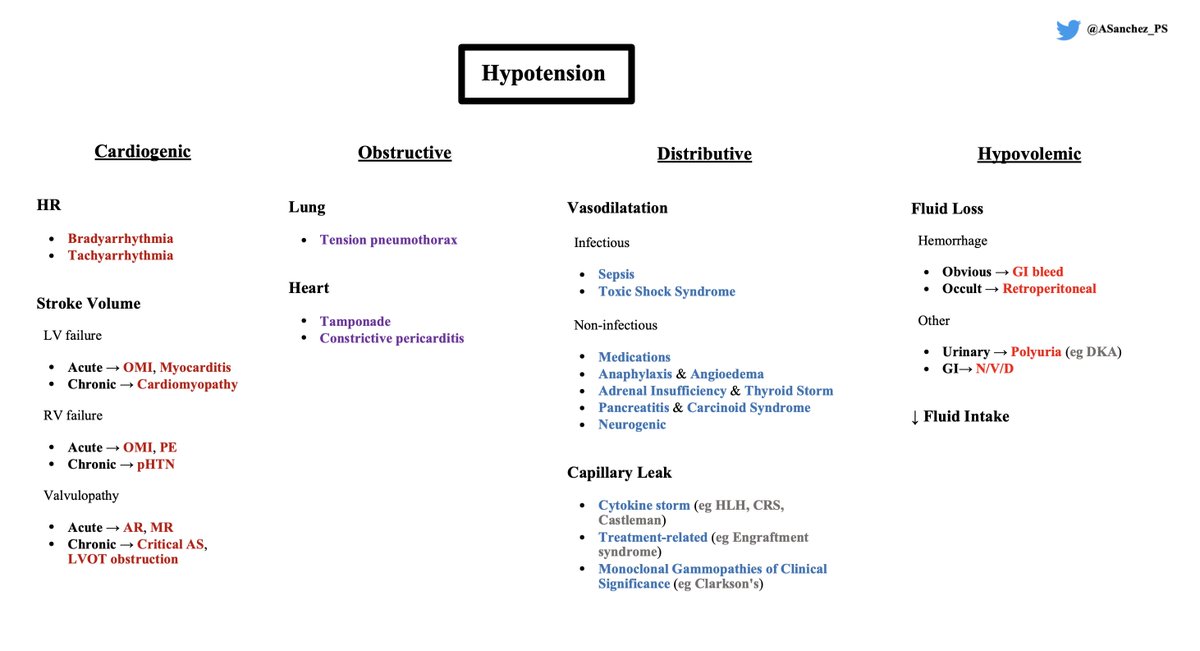
The traditional breakdown of hypotension/shock is very classic: my schema aims to sub-divide this framework & cover some new buckets.
Read on! 🧵
Recent ICU shifts = newfound appreciation for this clinical dilemma.
The traditional breakdown of hypotension/shock is very classic: my schema aims to sub-divide this framework & cover some new buckets.
Read on! 🧵

First, recall BP is a product of Cardiac Output * Systemic Vascular Resistance.
When assessing hypotension, cardiogenic etiologies should come to mind first because a markedly abnormal Heart Rate derangement may provide an up-front answer.
Think extremes:
- HR < 30
- HR > 150
When assessing hypotension, cardiogenic etiologies should come to mind first because a markedly abnormal Heart Rate derangement may provide an up-front answer.
Think extremes:
- HR < 30
- HR > 150

While the other cardiogenic etiologies cause ↓ MAP via Contractility/Preload issues, I find it more intuitive to group the leftover etiologies by:
- LV vs. RV failure
- Chronicity
If you group the DDx this way, you'll easily appreciate the common causes:
- LV vs. RV failure
- Chronicity
If you group the DDx this way, you'll easily appreciate the common causes:
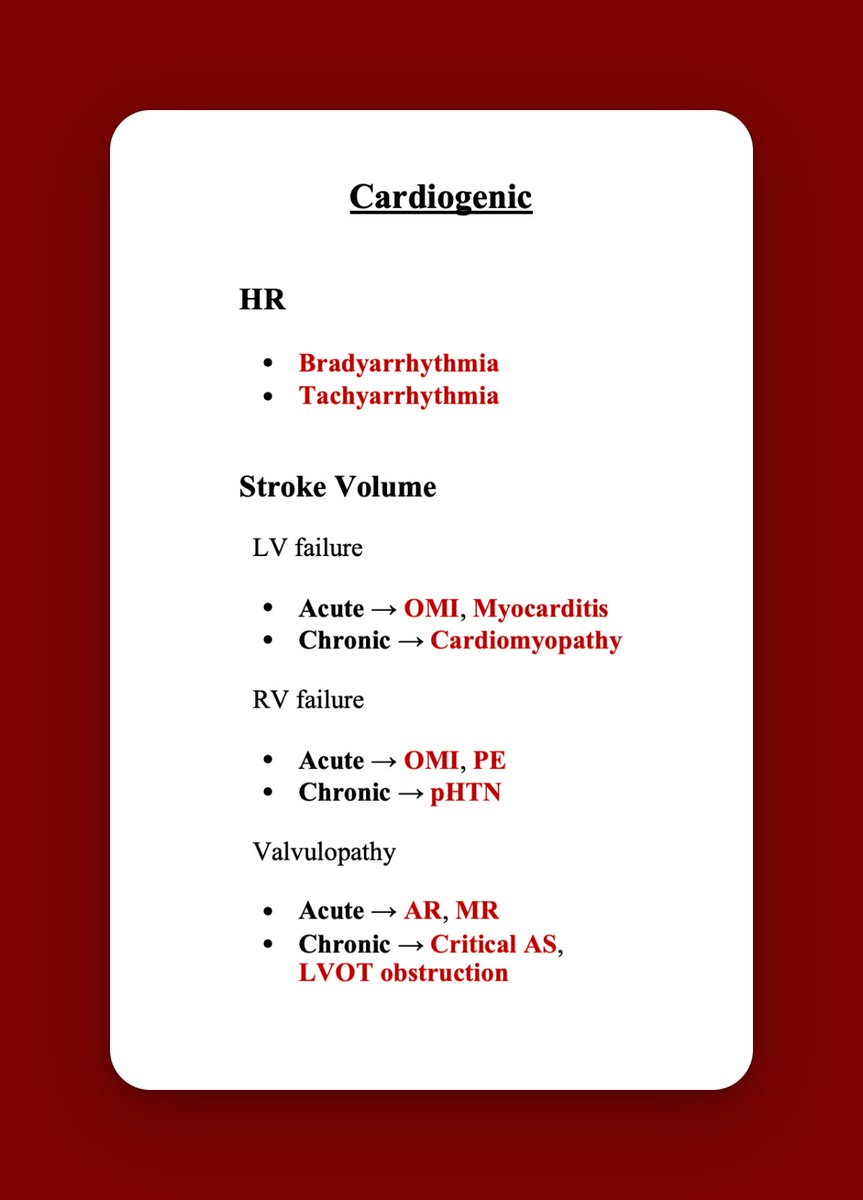
Cardiogenic pearls/pitfalls ⚪
⚪ Auscultate closely! Hemodynamically-significant valvulopathy is likely audible!
⚪ Acute AR & MR is often due to endocarditis, occlusive MI (OMI), & aortic dissection
⚪ Don't rely on troponin to rule-out OMI! ECG = queen!
⚪ Auscultate closely! Hemodynamically-significant valvulopathy is likely audible!
⚪ Acute AR & MR is often due to endocarditis, occlusive MI (OMI), & aortic dissection
⚪ Don't rely on troponin to rule-out OMI! ECG = queen!
Obstructive etiologies come next because you should be assessing for absent breath sounds (pneumothorax) & decreased heart sounds (tamponade) while listening for valvulopathy.
Looking for an elevated JVP provides another important data point in your global assessment!
Looking for an elevated JVP provides another important data point in your global assessment!
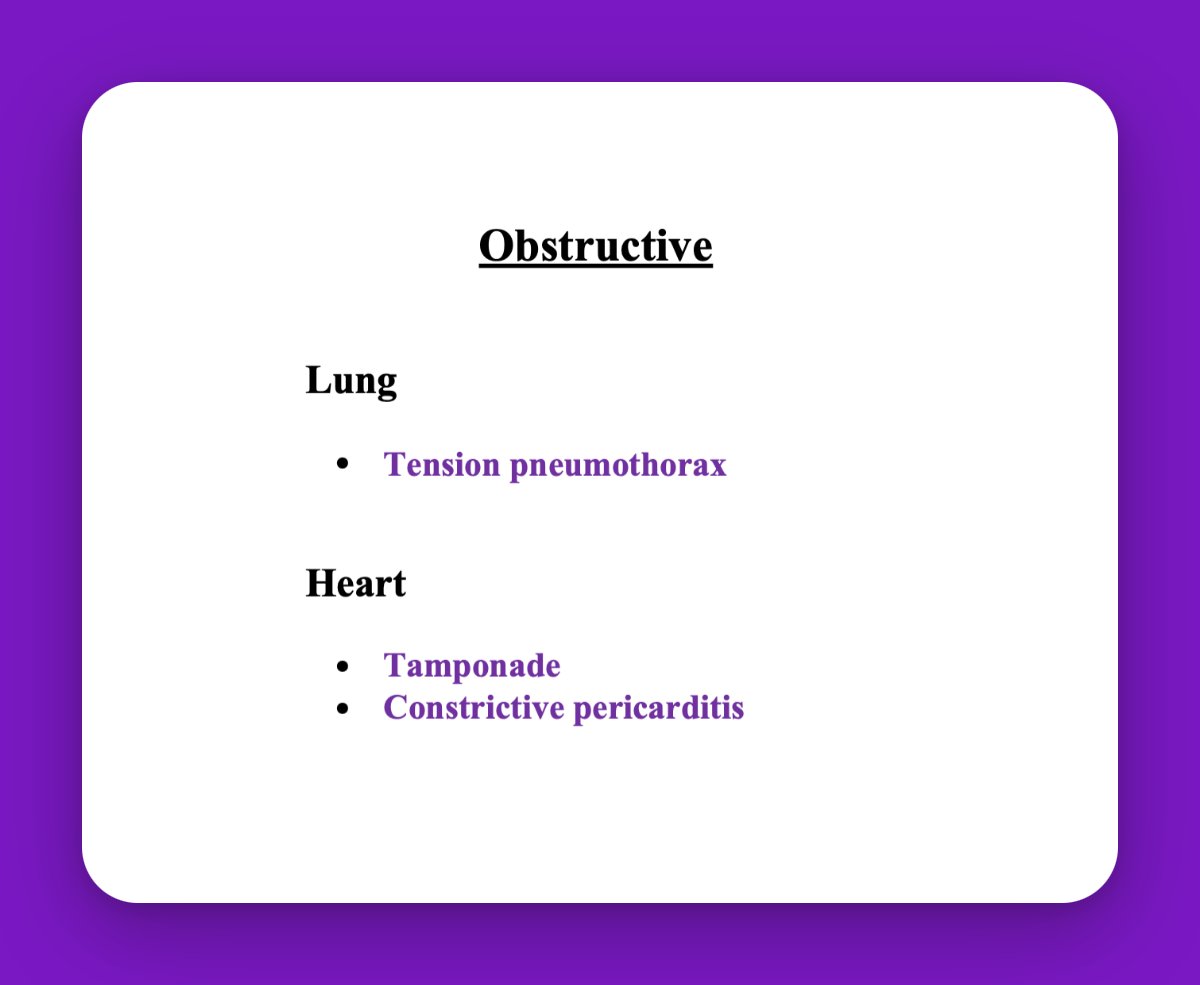
Obstructive pearl ⚪
⚪ POCUS can be helpful: a non-plethoric IVC can be used to essentially rule-out obstructive etiologies
(This makes sense given the pathophysiology of obstruction necessitating a "back pressure" into the IVC.)
⚪ POCUS can be helpful: a non-plethoric IVC can be used to essentially rule-out obstructive etiologies
(This makes sense given the pathophysiology of obstruction necessitating a "back pressure" into the IVC.)
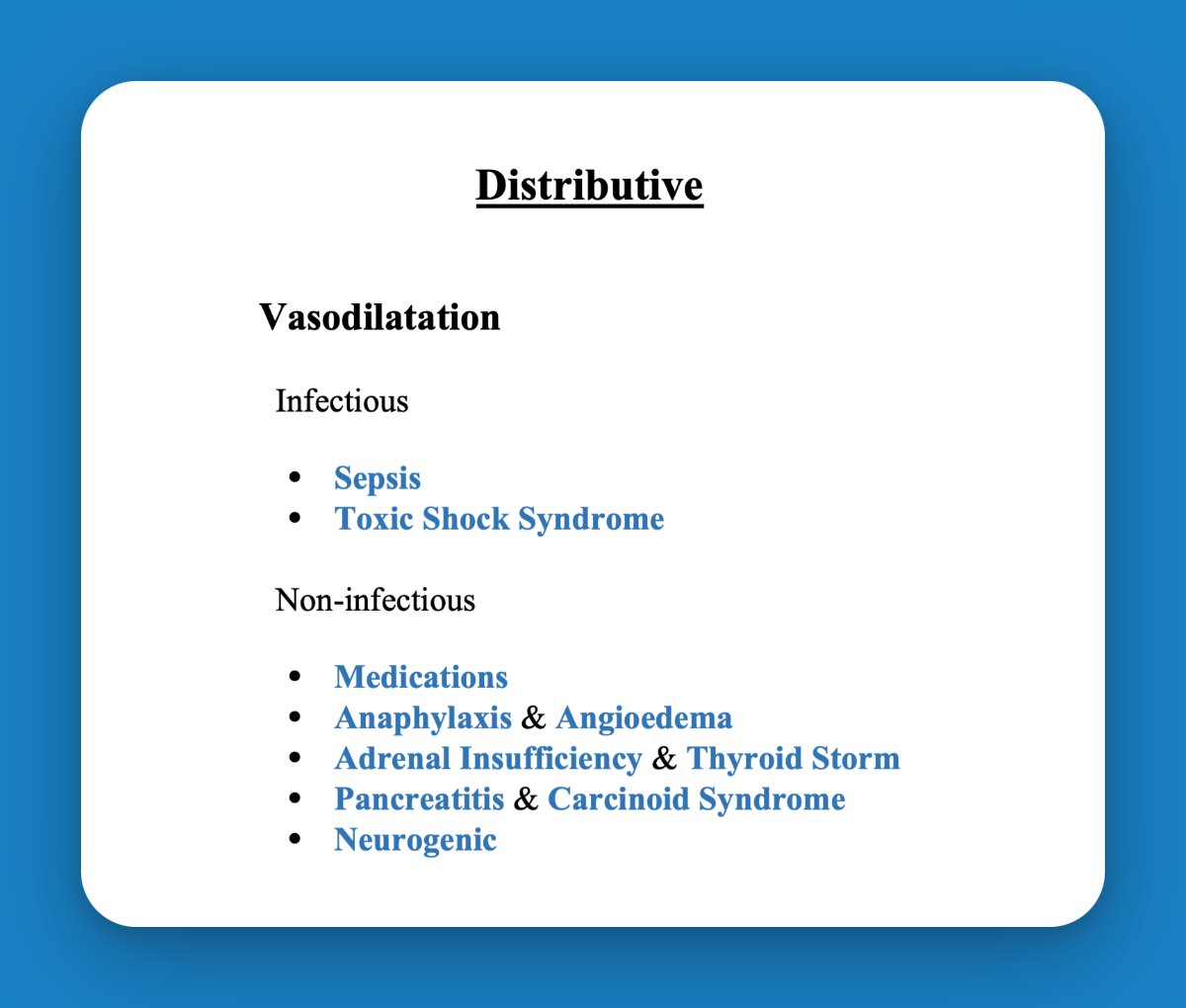
Distributive etiologies cause ↓ MAP via ↓ Systemic Vascular Resistance.
Classically, this is due to vasodilatation.
I recommend stratifying vasodilatory causes into Infectious & Non-infectious etiologies.
These are your 1st-pass, can't miss diseases:
Classically, this is due to vasodilatation.
I recommend stratifying vasodilatory causes into Infectious & Non-infectious etiologies.
These are your 1st-pass, can't miss diseases:
If your 1st-pass review isn't explanatory, consider Capillary Leak Syndromes.
Clues include:
💧 Multi-organ dysfunction
💧 Cytopenias
💧 Capillary leak (eg anasarca)
Clues include:
💧 Multi-organ dysfunction
💧 Cytopenias
💧 Capillary leak (eg anasarca)
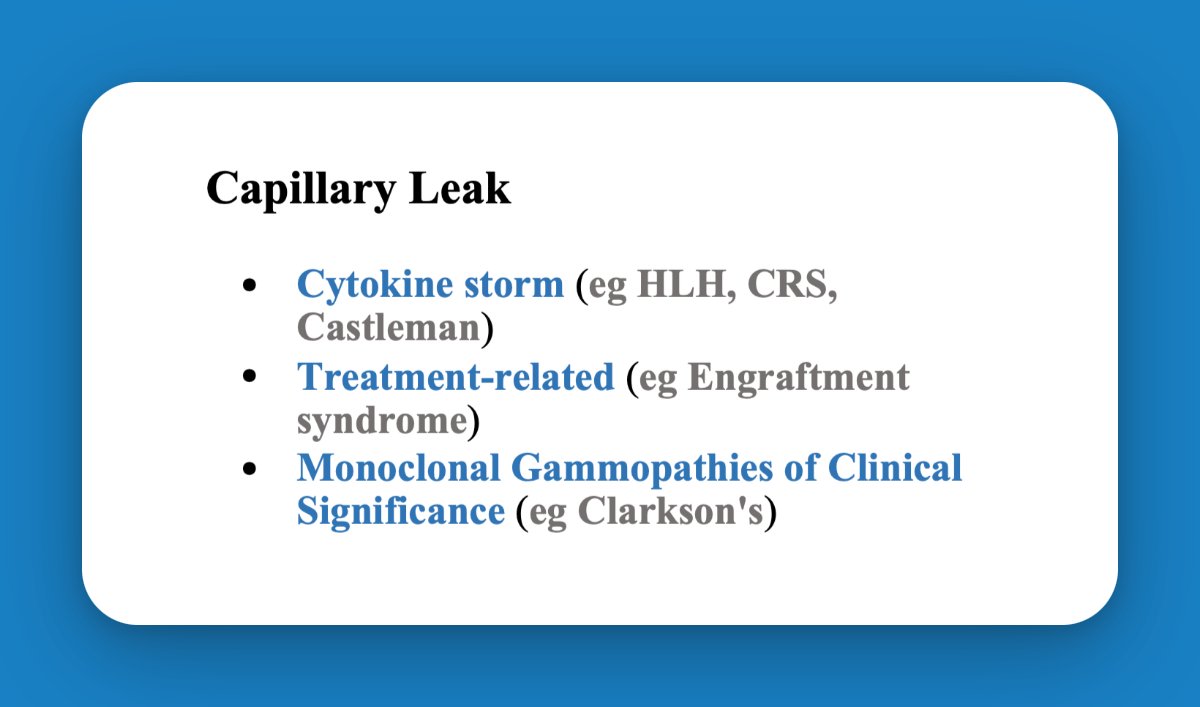
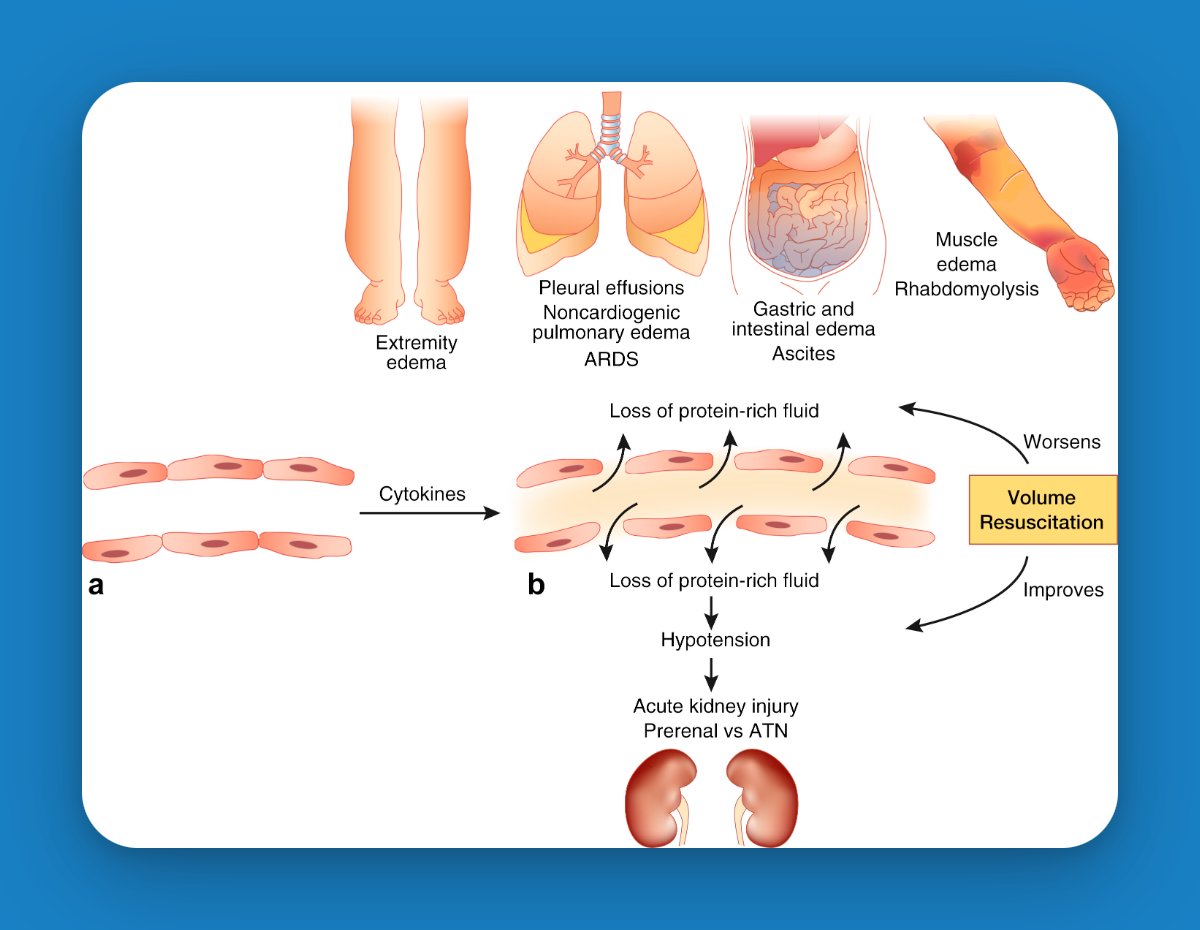
💧 More on Capillary Leak Syndrome here:
kidney-international.org
💥 More on Monoclonal Gammopathies of Clinical Significance here:
kidney-international.org
💥 More on Monoclonal Gammopathies of Clinical Significance here:
Finally, hypovolemic causes of hypotension = Fluid Loss vs. ↓ Fluid Intake.
These etiologies are usually apparent on history (eg gastroenteritis), physical (eg melena), or labs (eg DKA).
However, consider retroperitoneal hemorrhage as an occult etiology in the right patient!
These etiologies are usually apparent on history (eg gastroenteritis), physical (eg melena), or labs (eg DKA).
However, consider retroperitoneal hemorrhage as an occult etiology in the right patient!

Summary 🏁
🏁 Cardiogenic DDx = HR vs. Stroke Volume issue. (Stratify SV by LV vs. RV failure, & by acuity.)
🏁 Obstructive = ruled-out if IVC non-plethoric. Auscultate & consider CXR.
🏁 Distributive 1st-pass = Vasodilatation. (2nd-pass = Capillary Leak.)
🏁 Cardiogenic DDx = HR vs. Stroke Volume issue. (Stratify SV by LV vs. RV failure, & by acuity.)
🏁 Obstructive = ruled-out if IVC non-plethoric. Auscultate & consider CXR.
🏁 Distributive 1st-pass = Vasodilatation. (2nd-pass = Capillary Leak.)
🏁 Hypovolemic DDx = likely obvious on history/physical/labs. (But consider RP hemorrhage if concern for occult bleed.)
🚨 Disclaimer: I do realize the placement of some etiologies (eg PE) is likely to be debated. This is simply how my brain organized everything 🙂
That said...
🚨 Disclaimer: I do realize the placement of some etiologies (eg PE) is likely to be debated. This is simply how my brain organized everything 🙂
That said...
🤝 Please let me know how you'd adapt this schema!
🤝 Please drop any diagnostic pearls! Real-life work-up of this problem can be complex
🤝 Please drop any diagnostic pearls! Real-life work-up of this problem can be complex
nejm.org/doi/full/10.10…
Case 16-2022: A 55-Year-Old Man with Fevers, Night Sweats, and a Mediastinal Mass | NEJM
Case Records of the Massachusetts General Hospital from The New England Journal of Medicine — Case 1...

kidney-international.org/article/S0085-…
Capillary leak syndrome: etiologies, pathophysiology, and management
In various human diseases, an increase in capillary permeability to proteins leads to the loss of pr...

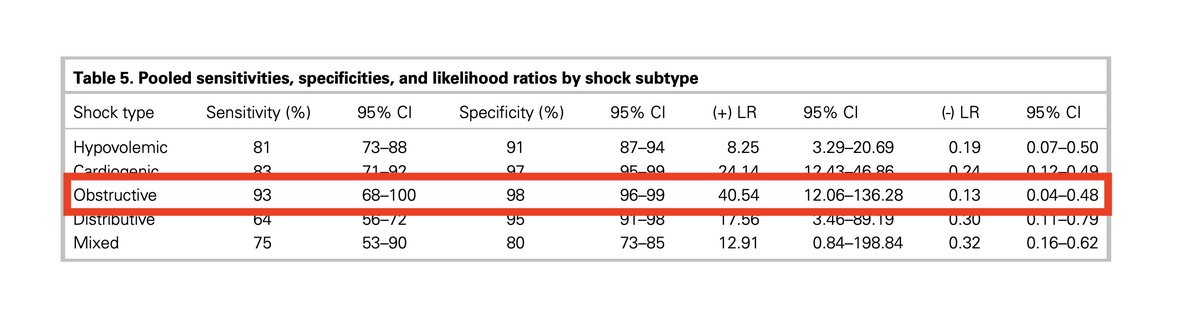
cambridge.org/core/journals/…
The diagnostic accuracy of a point-of-care ultrasound protocol for shock etiology: A systematic review and meta-analysis | Canadian Journal of Emergency Medicine | Cambridge Core
The diagnostic accuracy of a point-of-care ultrasound protocol for shock etiology: A systematic revi...
Loading suggestions...