

What is the most likely diagnosis in this 45 y/o F with severe headache and n/v? 🧠
#neurology #Neurosurgery #radres #neurotwitter #MedEd #MedTwitter @TheASNR @RSNA
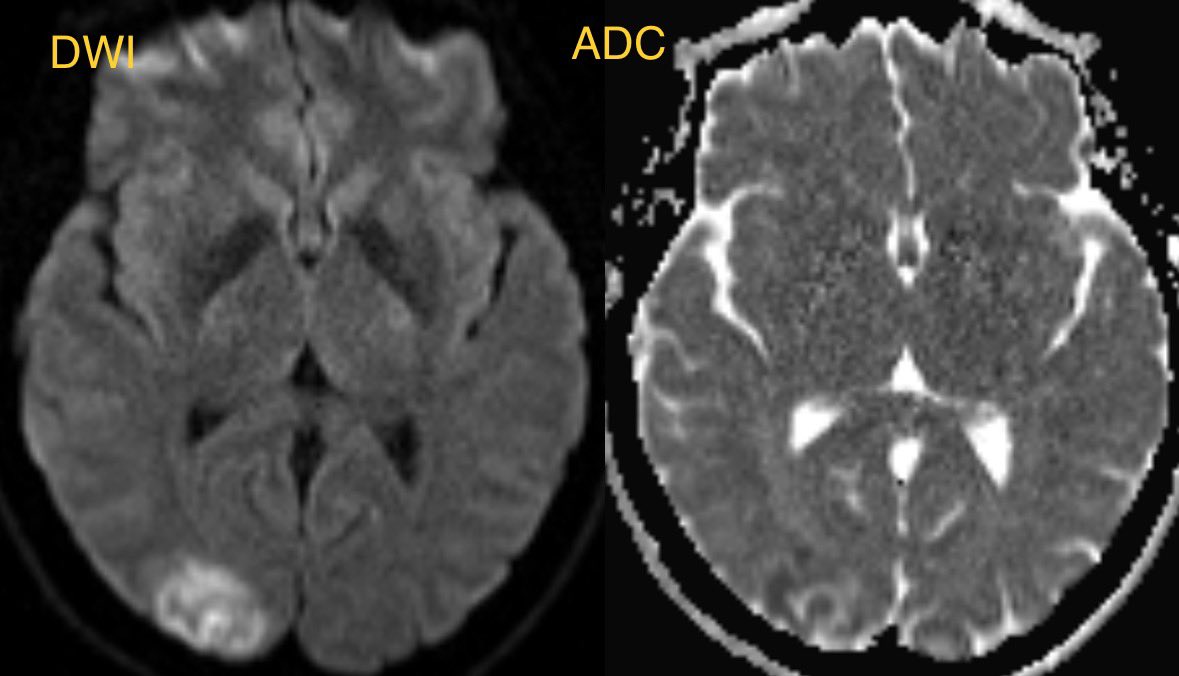
Initial MR shows cortical/subcortical restricted diffusion and edema predominantly in the right Occipital lobe
#neurology #Neurosurgery #radres #neurotwitter #MedEd #MedTwitter @TheASNR @RSNA
Initial MR shows cortical/subcortical restricted diffusion and edema predominantly in the right Occipital lobe
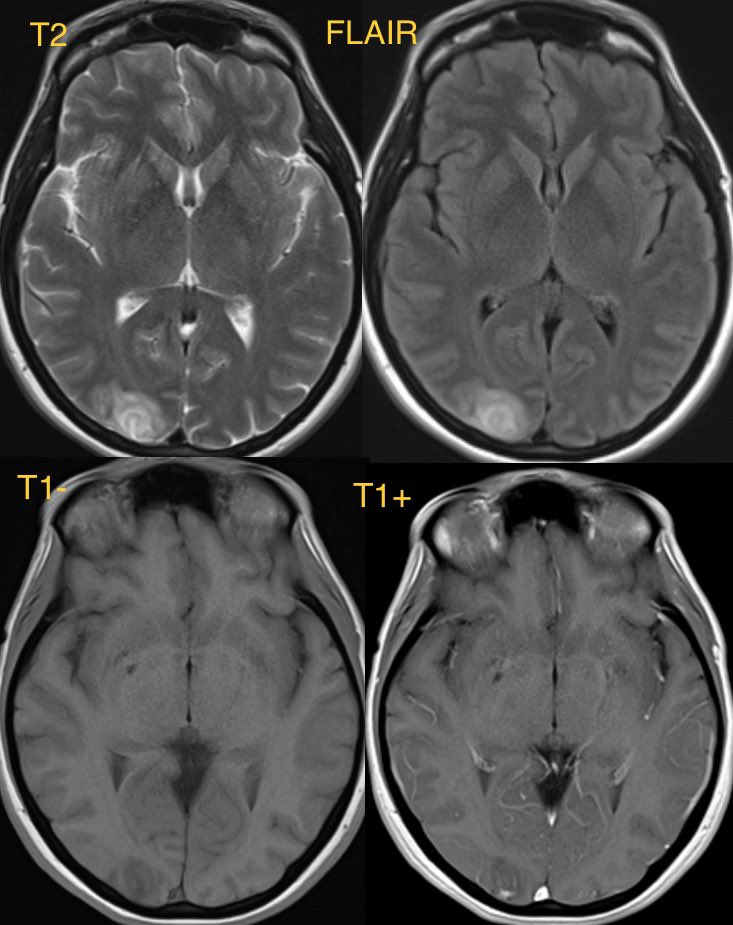
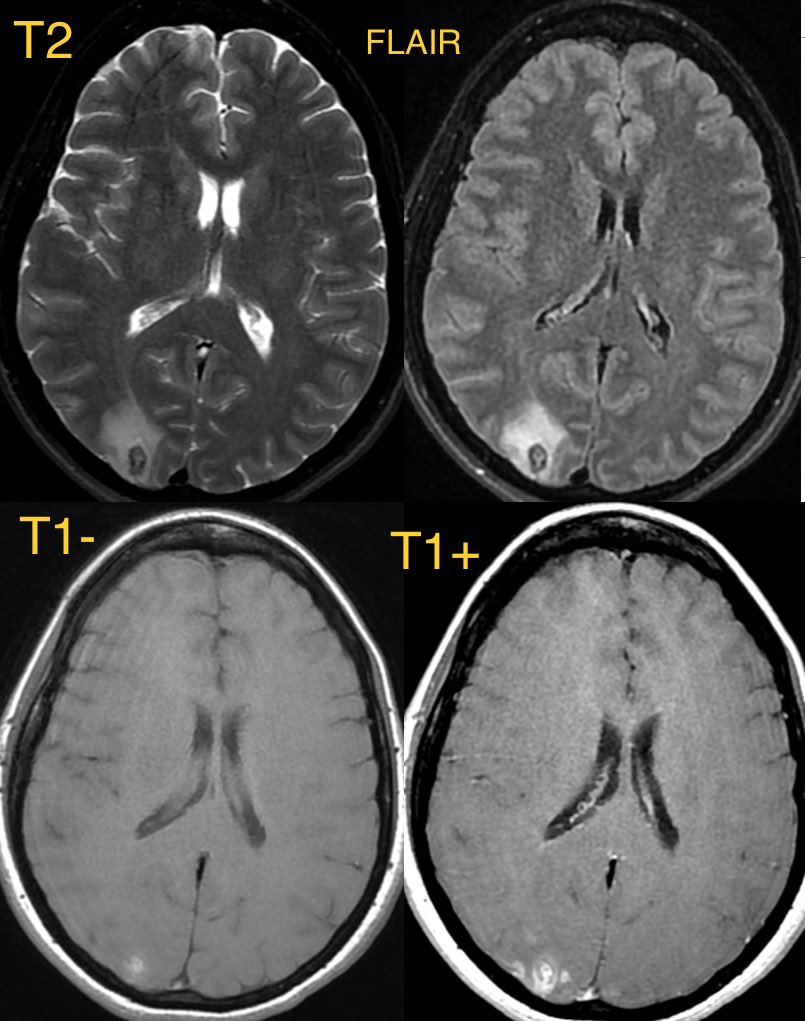
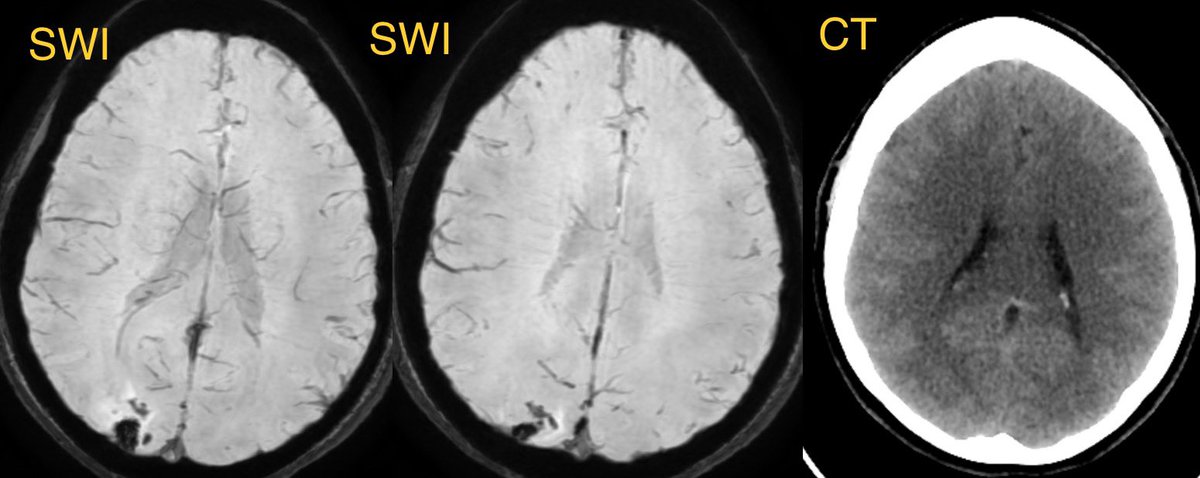
Follow up MR a few days later with worsening symptoms shows progression of right occipital swelling and focal lobar hemorrhage. There is associated cortical and b/l occipital leptomeningeal enhancement


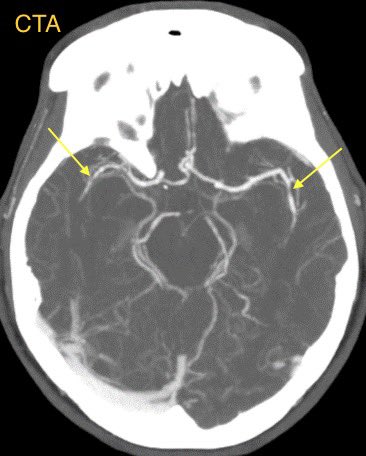
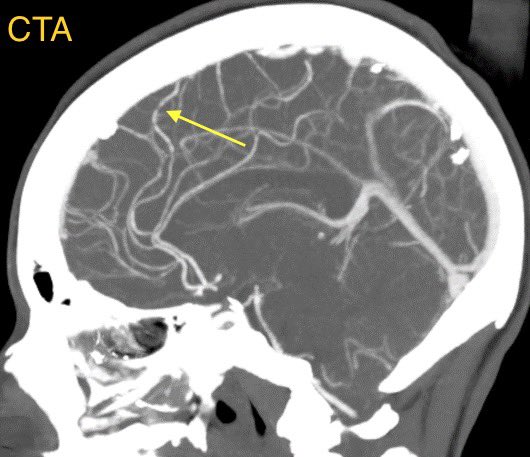
CTA was done displaying multifocal areas of stenosis most notable in the MCA and ACA territories

Answer: There are multiple correct answers in this case that an argument can be made for (RCVS, vasculitis, PRES) though personally feel RCVS fits the imaging and history best (others may disagree) 🧠
RCVS: presents as an acute severe headache
imaging:
▶️convexity SAH, lobar hemorrhage, edema, and infarcts
▶️CTA/MRA may show vasospasm
💡 RCVS is due to many etiologies which induce a disturbance of control in vascular tone leading to vasoconstriction
imaging:
▶️convexity SAH, lobar hemorrhage, edema, and infarcts
▶️CTA/MRA may show vasospasm
💡 RCVS is due to many etiologies which induce a disturbance of control in vascular tone leading to vasoconstriction
💡 Differentiating RCVS from vasculitis is probably easiest clinically as RCVS is acute severe headache while vasculitis is a more indolent process (would love a neurologist’s input here)
💡 On imaging, MR with VESSEL WALL IMAGING can help to differentiate RCVS from vasculitis which displays much more enhancement while RCVS typically shows little to no enhancement
💡 PRES also has a lot of overlap with RCVS and they can be associated with each other
PRES usually has more edema, more often bilateral, and less often has restricted diffusion and hemorrhage (though it can)
PRES usually has more edema, more often bilateral, and less often has restricted diffusion and hemorrhage (though it can)
Loading suggestions...