

Should radiology residents in India subspecialize? Are we heading to hypersaturation?
A look at an insightful IJRI article
First off, wondering what an anatomist,ENT surgeon & forensic doc contribute to an article on radiology residents? This is India, we are like this only😉🤟
A look at an insightful IJRI article
First off, wondering what an anatomist,ENT surgeon & forensic doc contribute to an article on radiology residents? This is India, we are like this only😉🤟
2/n
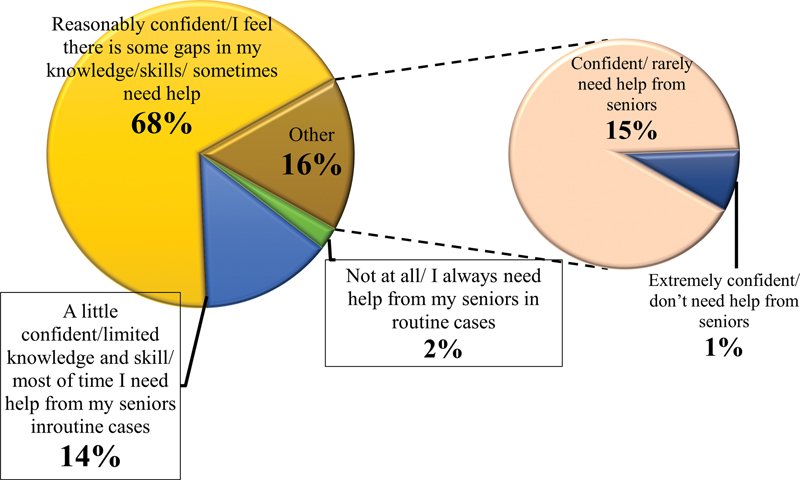
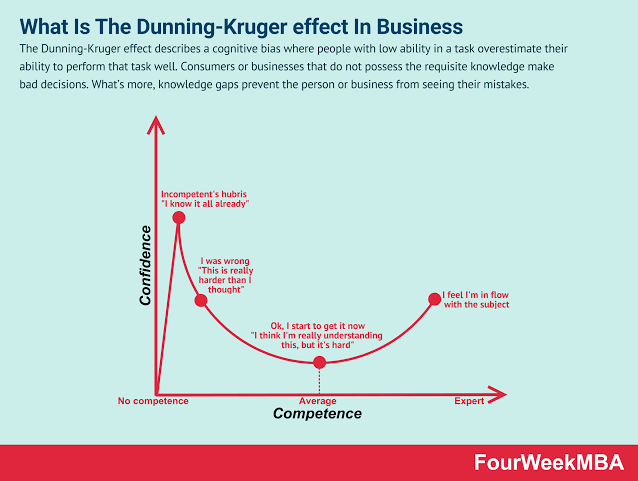
3rd year MD/DNB residents were surveyed. In India residency is 3 years. It is 4 to 5 years in the West. The 16% who think they don't need to train further in radiology are still on the first hill of the Dunning Kruger curve (unconscious incompetence)
3rd year MD/DNB residents were surveyed. In India residency is 3 years. It is 4 to 5 years in the West. The 16% who think they don't need to train further in radiology are still on the first hill of the Dunning Kruger curve (unconscious incompetence)
3/n
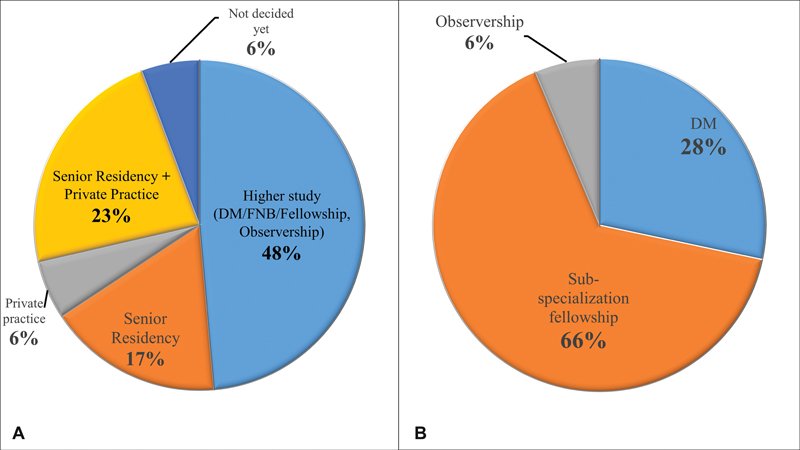
Glad to know most are thinking to specialize.
Most striking line is there are now 1500 MD&DNB Rad seats in India. We are heading for catastrophic saturation.
For perspective,a decade back I just scraped into MD radiology in Mumbai at AIR 73. Needed AIR 250 to get MD Rad then
Glad to know most are thinking to specialize.
Most striking line is there are now 1500 MD&DNB Rad seats in India. We are heading for catastrophic saturation.
For perspective,a decade back I just scraped into MD radiology in Mumbai at AIR 73. Needed AIR 250 to get MD Rad then
4/n
We will have 15000+ new radiologists in a decade.
I fear that not just radiology but all MD, MS, DM, MCH branches in India are going the dental way of extreme saturation (no offense to my dentist friends). There are just not enough hospitals to accomodate that many doctors.
We will have 15000+ new radiologists in a decade.
I fear that not just radiology but all MD, MS, DM, MCH branches in India are going the dental way of extreme saturation (no offense to my dentist friends). There are just not enough hospitals to accomodate that many doctors.
5/n
High volume work in India is also becoming a myth, at least in Maharashtra with increase in seats and hospitals
What can rad residents do? If planning to settle in tier 3 cities or smaller, no issues. However in metros & tier2, subspecialization gives you something of a moat
High volume work in India is also becoming a myth, at least in Maharashtra with increase in seats and hospitals
What can rad residents do? If planning to settle in tier 3 cities or smaller, no issues. However in metros & tier2, subspecialization gives you something of a moat
6/n
What is a moat?
A moat in investment finance is a competitive advantage which an entity has relative to its competitors.
Subspecialization gives you an added advantage in some scenarios for employment & entrepreneurship.
What is a moat?
A moat in investment finance is a competitive advantage which an entity has relative to its competitors.
Subspecialization gives you an added advantage in some scenarios for employment & entrepreneurship.
7/n
However if this goes on (no reason to see why it won't), there will be mass migration of doctors abroad instead of doctors moving to rural areas as the government intends.
Let's look at a realistic scenario which is happening today itself👇
However if this goes on (no reason to see why it won't), there will be mass migration of doctors abroad instead of doctors moving to rural areas as the government intends.
Let's look at a realistic scenario which is happening today itself👇
8/n
Suppose there is a DM interventional neuroradiologist who has trained for 12 years from start of MBBS till end of DM. He/she has further completed 2 years of government bond service. After 14 years they return to own tier 2 city (population 3 million) to practice.
Suppose there is a DM interventional neuroradiologist who has trained for 12 years from start of MBBS till end of DM. He/she has further completed 2 years of government bond service. After 14 years they return to own tier 2 city (population 3 million) to practice.
9/n
But there are already 2 fellowship trained IRs who do neurointerventions + 3 neurologists & neurosurgeons who do own neurointerventions in the city. For pop 3 million this is more than enough. The new doc struggles to get patients. There are no vacancies in govt hospitals too
But there are already 2 fellowship trained IRs who do neurointerventions + 3 neurologists & neurosurgeons who do own neurointerventions in the city. For pop 3 million this is more than enough. The new doc struggles to get patients. There are no vacancies in govt hospitals too
10/n
Moving to rural areas is not an option- what will a DM interventional neuroradiologist do in rural areas ? No INR work facilities created by the government, no appropriate schools for children. Contrast this with UK where even small towns have very high quality facilities
Moving to rural areas is not an option- what will a DM interventional neuroradiologist do in rural areas ? No INR work facilities created by the government, no appropriate schools for children. Contrast this with UK where even small towns have very high quality facilities
11/n
At such time they have no option but to migrate abroad. Can be anywhere from USA,UK,Canada,Aus to Middle East. This is easier in radiology,pathology but extremely difficult for those in surgical branches. The situation is grim and sad reality for those recently completing PG
At such time they have no option but to migrate abroad. Can be anywhere from USA,UK,Canada,Aus to Middle East. This is easier in radiology,pathology but extremely difficult for those in surgical branches. The situation is grim and sad reality for those recently completing PG
Loading suggestions...