

This presentation has been discussed at
@ASTRO_org @ACRORadOnc @RadiumSociety
@ARRO_org @ACROresident
Thanks to these experts for the contents.
References:
bit.ly
@ASTRO_org @ACRORadOnc @RadiumSociety
@ARRO_org @ACROresident
Thanks to these experts for the contents.
References:
bit.ly

@ASTRO_org @ACRORadOnc @RadiumSociety @ARRO_org @ACROresident Starting with the best advice received for the job search.
Life:
Life:
@ASTRO_org @ACRORadOnc @RadiumSociety @ARRO_org @ACROresident @WCInvestor Effort and reward
Residents should write down what they want in a job.
Residents should write down what they want in a job.
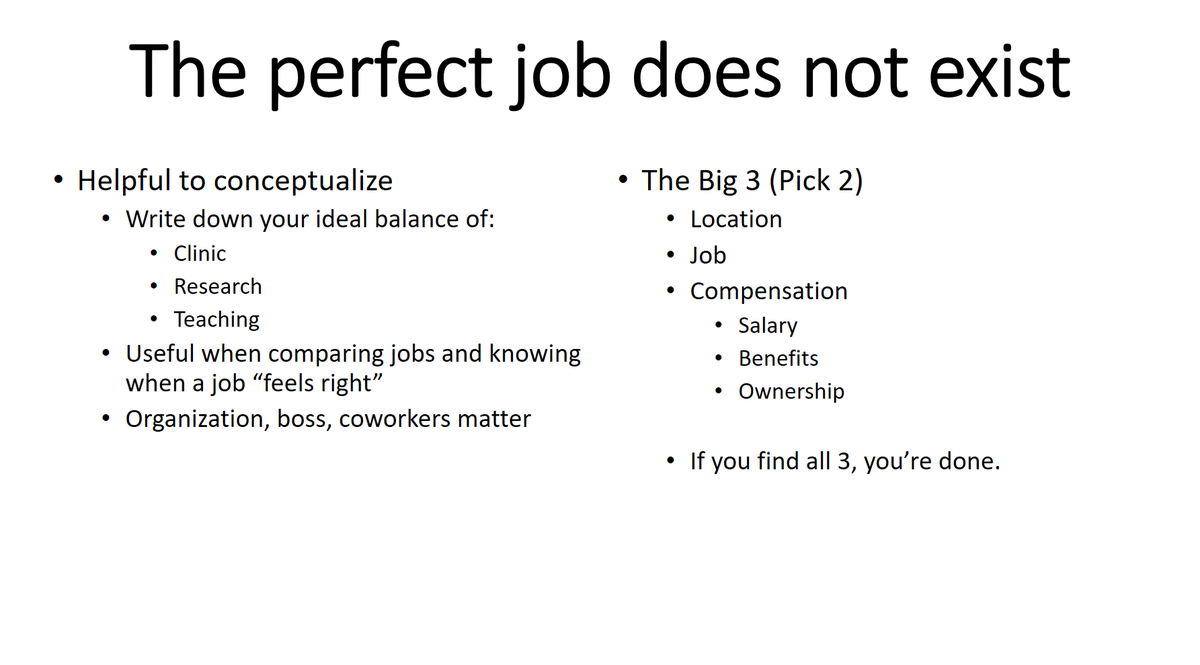
Here are the top 10 predictors of happiness for a radiation oncologist taking a job
In the US, there is a wide range of employment types. Most residents are somewhat familiar with the academic model because it has provided them training.
For remainder of this talk:
🔴star will be more pertinent for academics
🔵star will be more pertinent to non-academics
For remainder of this talk:
🔴star will be more pertinent for academics
🔵star will be more pertinent to non-academics
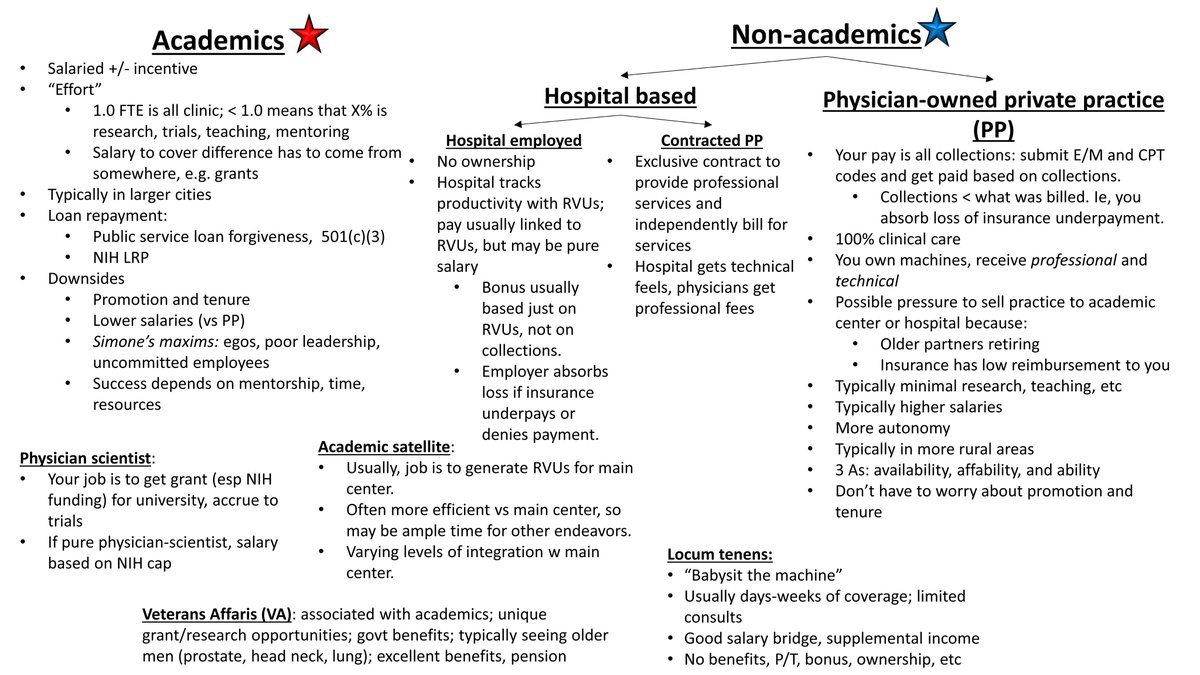
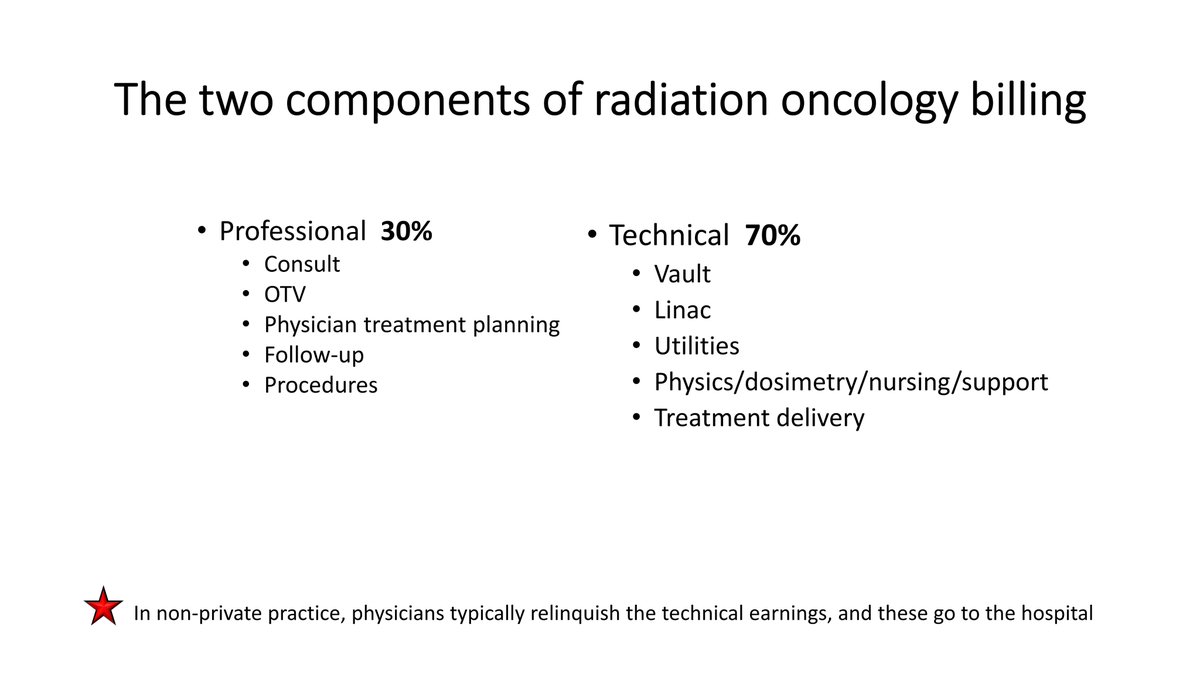
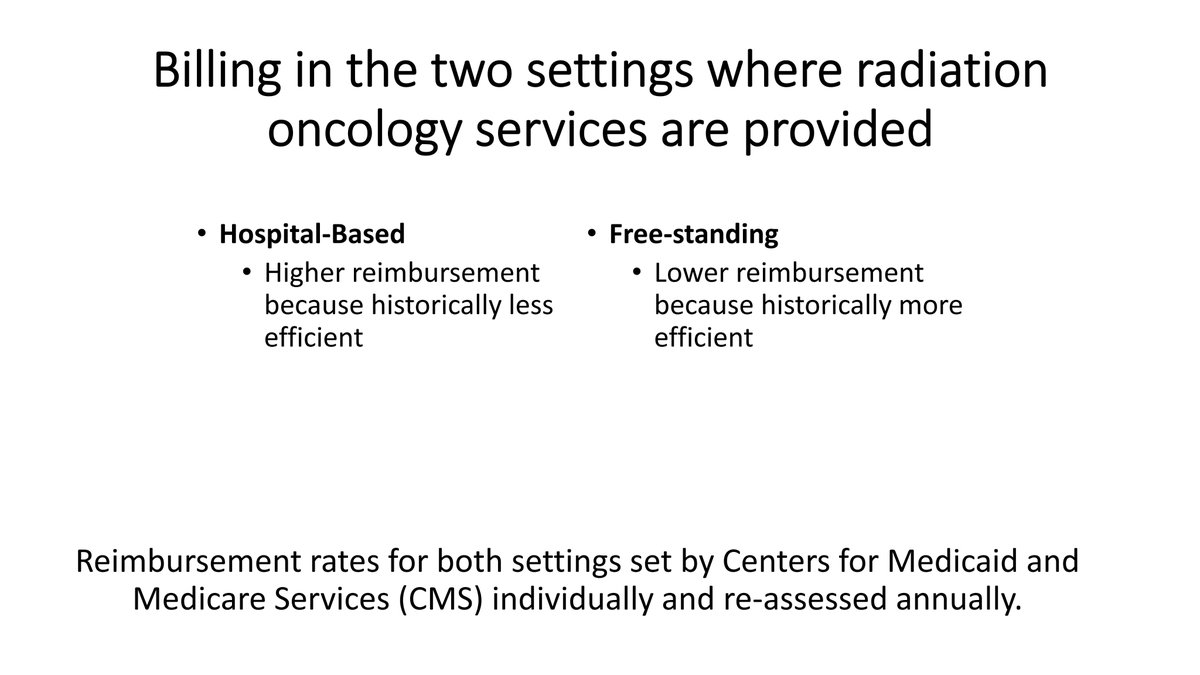
There are two main components of radiation oncology billing, and there are different settings where services can be provided.
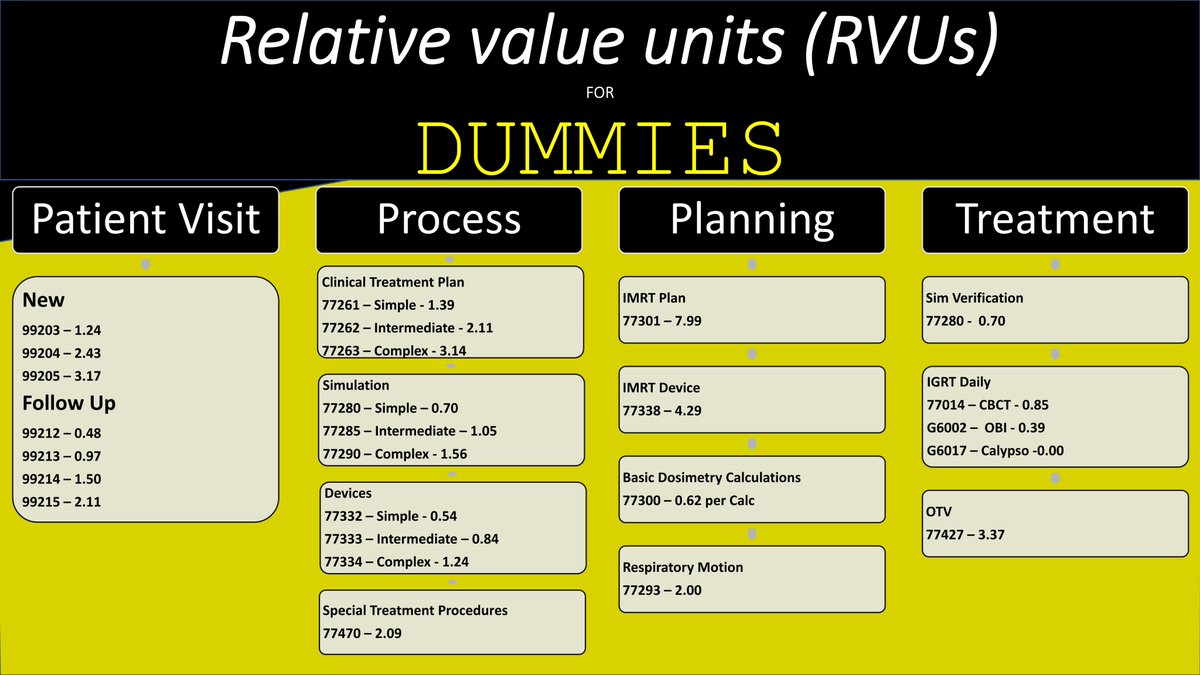
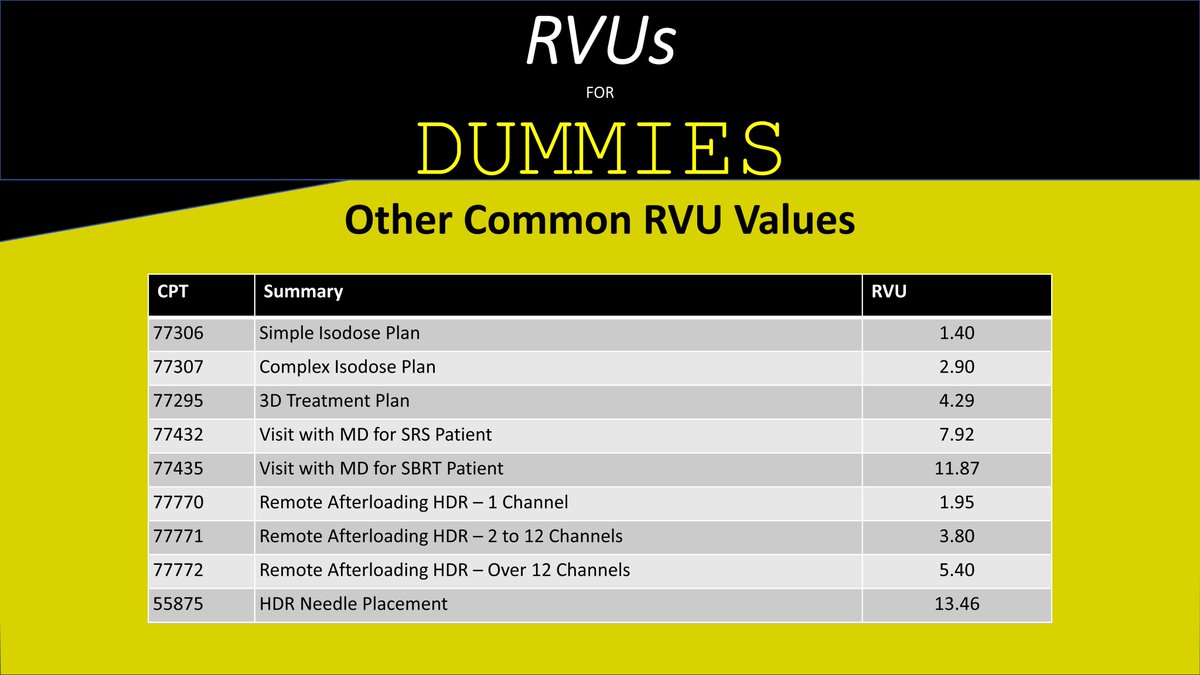
@DigiaimoRon @RevenueCycleInc is a #radonc finance expert and can tell you all the details of billing and RVUs.
@DigiaimoRon @RevenueCycleInc is a #radonc finance expert and can tell you all the details of billing and RVUs.
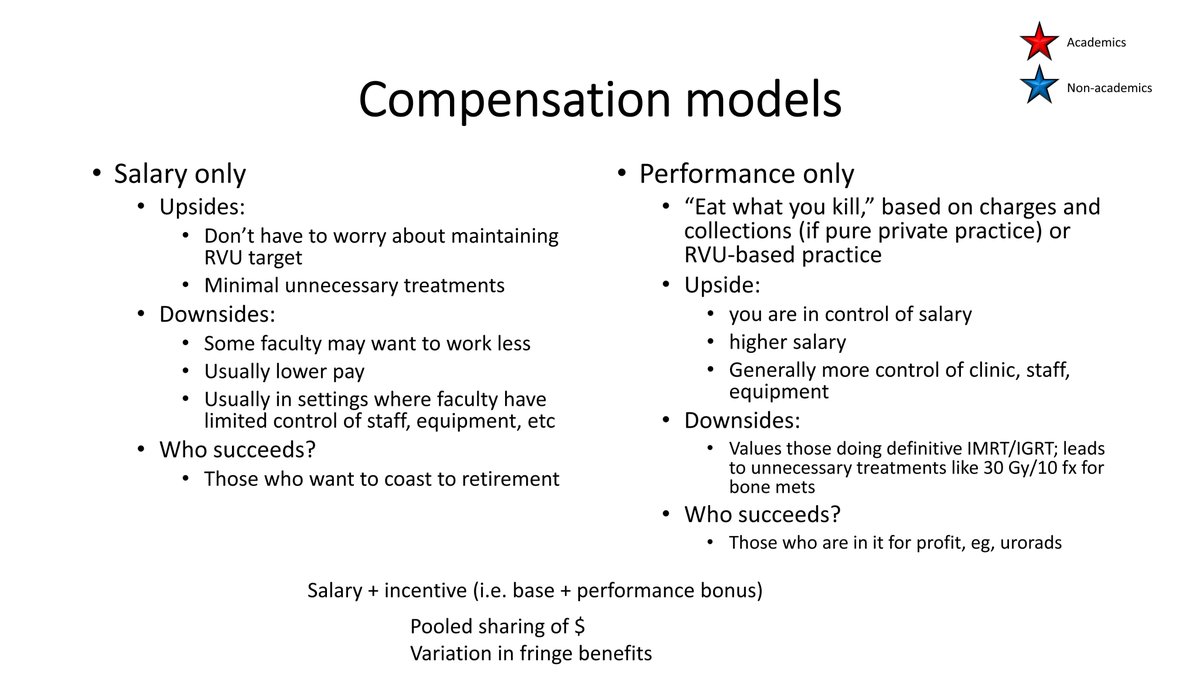
@DigiaimoRon @RevenueCycleInc With either academics🔴 or non-academics🔵, there are usually two types of compensation models.
Both models have potential upsides and downsides.
Many practices use a hybrid model of salary + incentive.
Both models have potential upsides and downsides.
Many practices use a hybrid model of salary + incentive.
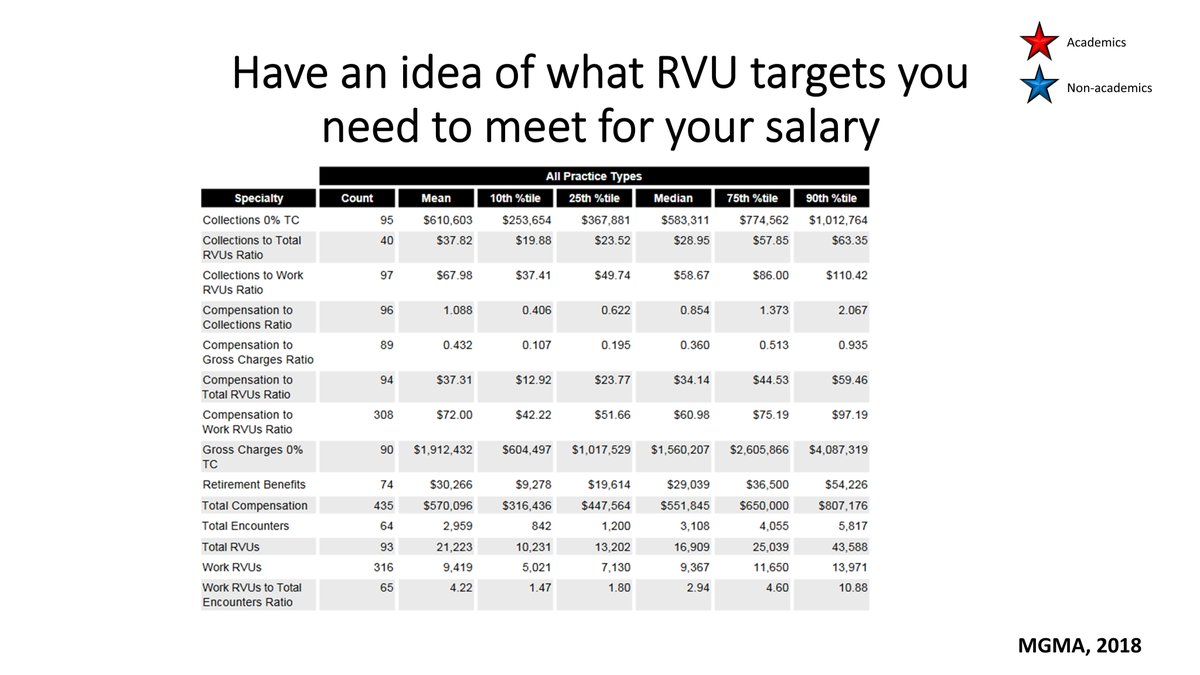
Details of compensation and RVUs are available from different sources.
doximity.com
doximity.com

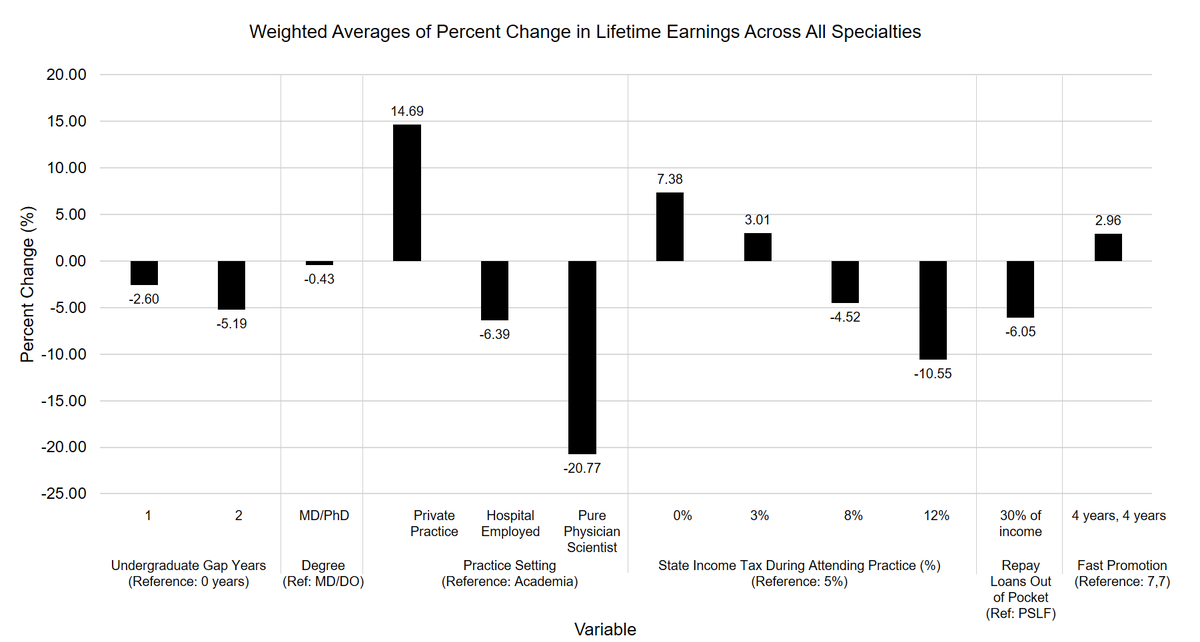
Our group is also making a model to compare different career paths and impact on lifetime earnings. Here are prelim results for all medical specialties.
@ChristineLin08 does incredible work.
@ChristineLin08 does incredible work.
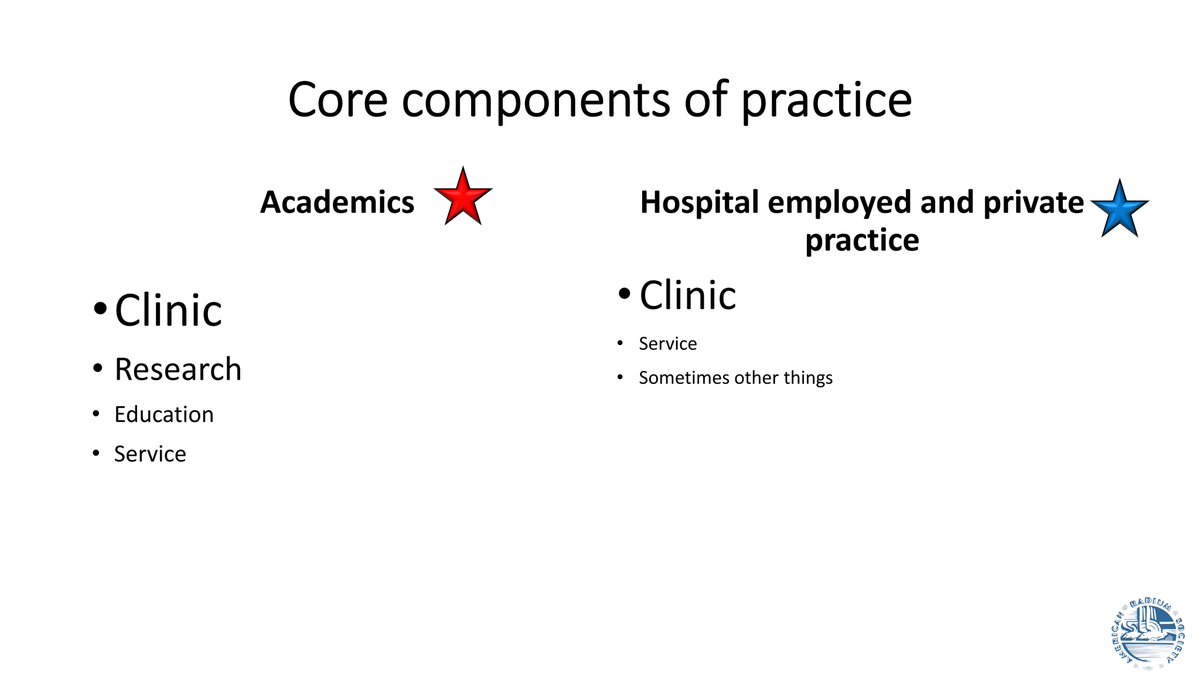
@ChristineLin08 Academic and non-academic practices have several core components of practice. In both settings, clinical care is usually a top priority.
@ChristineLin08 Academic medical centers🔴include most specialty centers and hospitals in the US, and they have their own unwritten rules:
@ChristineLin08 In an oversimplified world, academic medical centers are usually composed of two core entities: the university and the hospital.
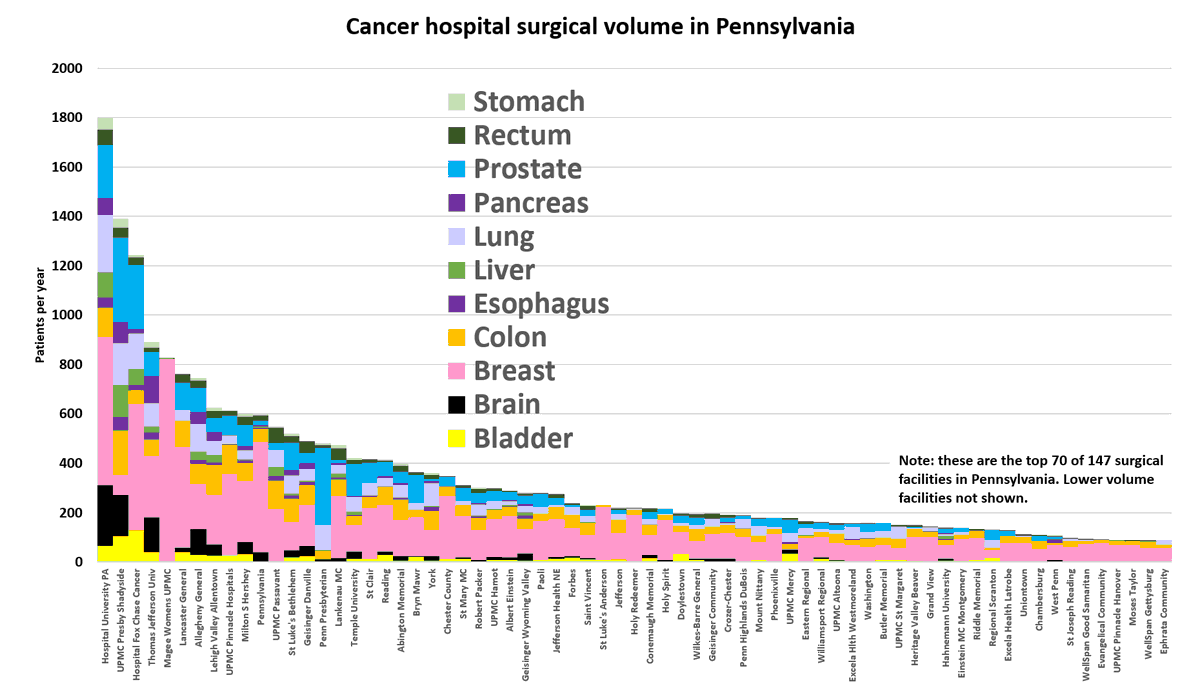
@ChristineLin08 In oncology, academic medical centers are also usually high volume facilities, both with respect to surgery...
@ChristineLin08 and radiation therapy:
@ChristineLin08 The data above come from the NCDB, which anonymizes the facilities.
However, many states report facility volume per hospital. Data from @PennsylvaniaGov for:
@PennMedicine
@UPMCnews
@FoxChaseCancer
@TJUHospital
@LVHN
@PennStHershey
@TempleMedSchool
and others
However, many states report facility volume per hospital. Data from @PennsylvaniaGov for:
@PennMedicine
@UPMCnews
@FoxChaseCancer
@TJUHospital
@LVHN
@PennStHershey
@TempleMedSchool
and others
@ChristineLin08 @PennsylvaniaGov @PennMedicine @UPMCnews @FoxChaseCancer @TJUHospital @LVHN @PennStHershey @templemedschool Many oncologists work at academic medical centers because they want a mix of:
clinical care
research
education
All non-clinical time, should be "protected."
However, protecting time means having a lower FTE and generating fewer RVUs.
clinical care
research
education
All non-clinical time, should be "protected."
However, protecting time means having a lower FTE and generating fewer RVUs.
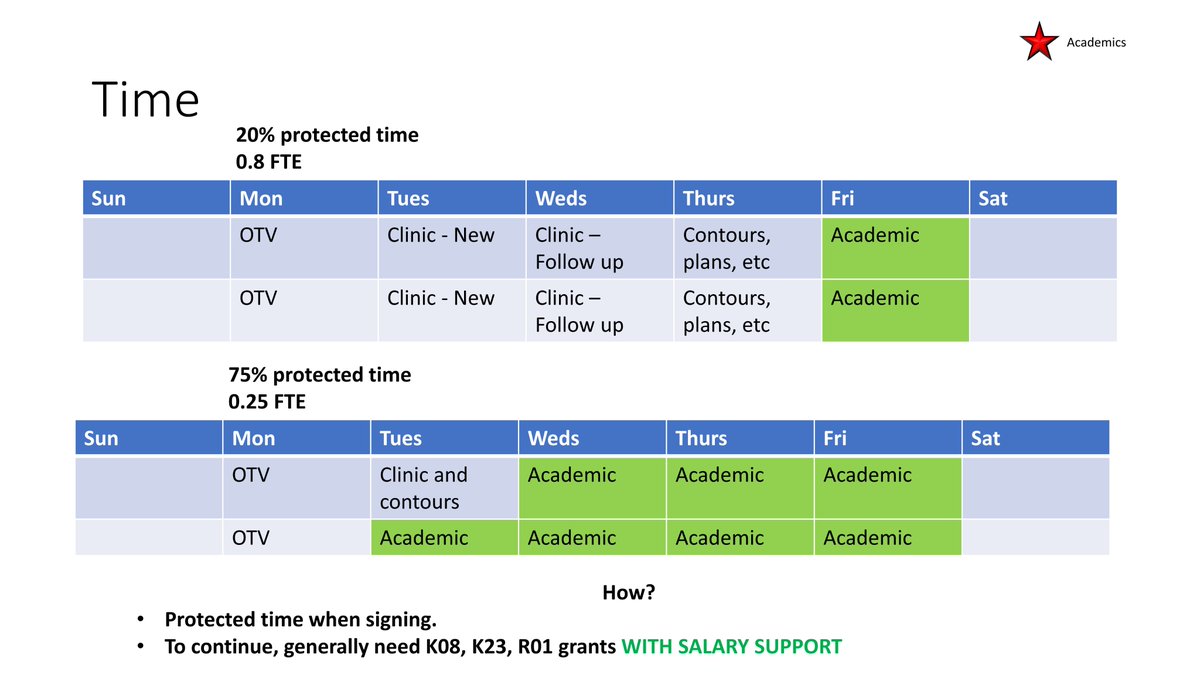
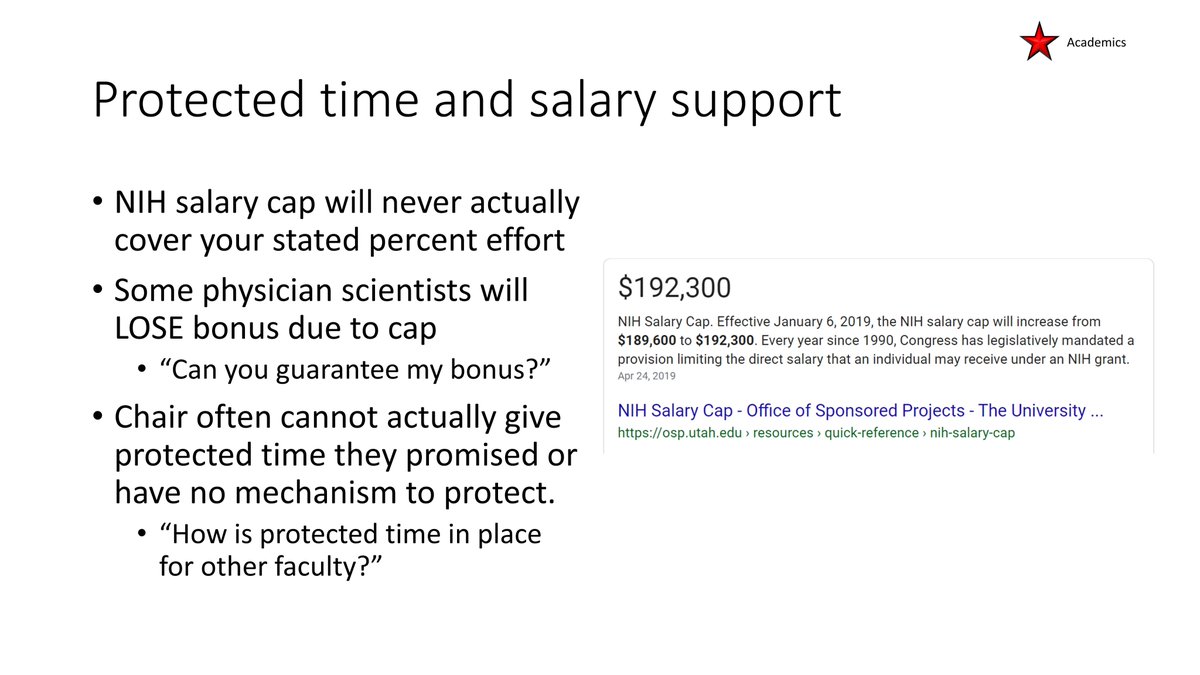
@ChristineLin08 @PennsylvaniaGov @PennMedicine @UPMCnews @FoxChaseCancer @TJUHospital @LVHN @PennStHershey @templemedschool To protect research time, academic researchers need to obtain grant funding and solve the convoluted problem of the @NIH cap gap.
The low @NIH @theNCI salary cap is one of the chief reasons few physicians stay on the path to being physician scientists.
The low @NIH @theNCI salary cap is one of the chief reasons few physicians stay on the path to being physician scientists.
@ChristineLin08 @PennsylvaniaGov @PennMedicine @UPMCnews @FoxChaseCancer @TJUHospital @LVHN @PennStHershey @templemedschool @NIH @theNCI Interestingly, one of the benefits of working in academics is loan repayment through PSLF and @NIH_LRP.
Thus, the US has an excellent solution for training clinical researchers + paying their loans (via a non MD/PhD path), but it struggles with retention.
Thus, the US has an excellent solution for training clinical researchers + paying their loans (via a non MD/PhD path), but it struggles with retention.
Here are some considerations to run a #radonc clinic.
In academics there is emphasis on FTE, but this is technically a time-based measurement from the university, not the hospital.
In both academics and non-academics, RVUs are the main consideration for clinical productivity.
In academics there is emphasis on FTE, but this is technically a time-based measurement from the university, not the hospital.
In both academics and non-academics, RVUs are the main consideration for clinical productivity.
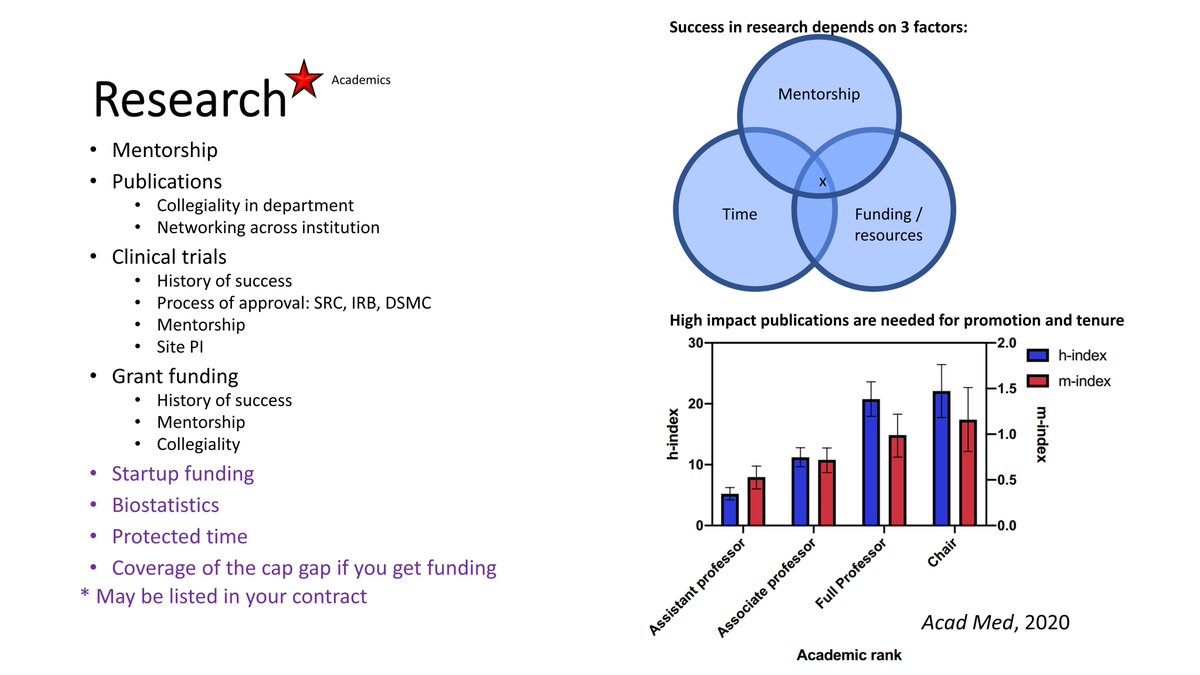
Research mostly applies to academicians (vs PP).
Success in research depends on mentorship, time, and resources. @freddyeescorcia
Research publication productivity affects promotion and tenure:
Success in research depends on mentorship, time, and resources. @freddyeescorcia
Research publication productivity affects promotion and tenure:
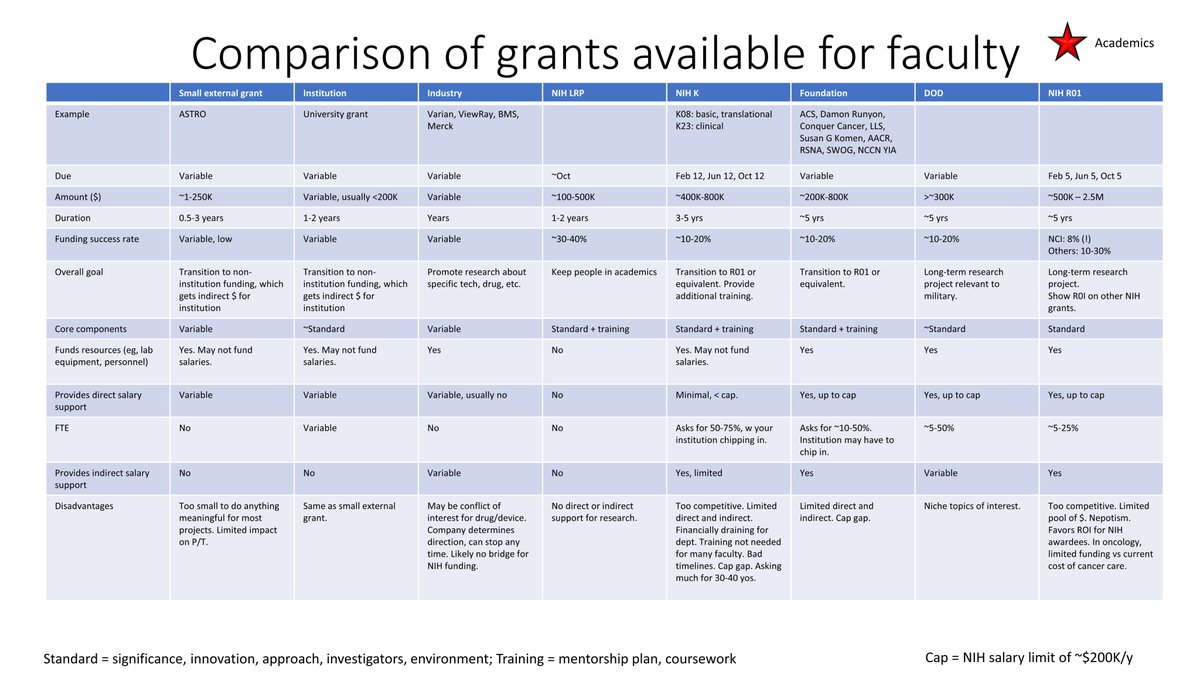
@freddyeescorcia There are different grants available for junior radiation oncologists.
However, #radonc is overall an underfunded field from @NIH @theNCI, and many burn out from this career path.
However, #radonc is overall an underfunded field from @NIH @theNCI, and many burn out from this career path.
@freddyeescorcia @NIH @theNCI Consider this:
1, how many @NIH R01-funded rad oncs do you know?
2, for simple questions in oncology where radiation is treatment option, why don't we have trials?
eg skin ca:
3, why is the cost of the field < just a few drugs?
1, how many @NIH R01-funded rad oncs do you know?
2, for simple questions in oncology where radiation is treatment option, why don't we have trials?
eg skin ca:
3, why is the cost of the field < just a few drugs?
Additionally, academicians have a role in education:
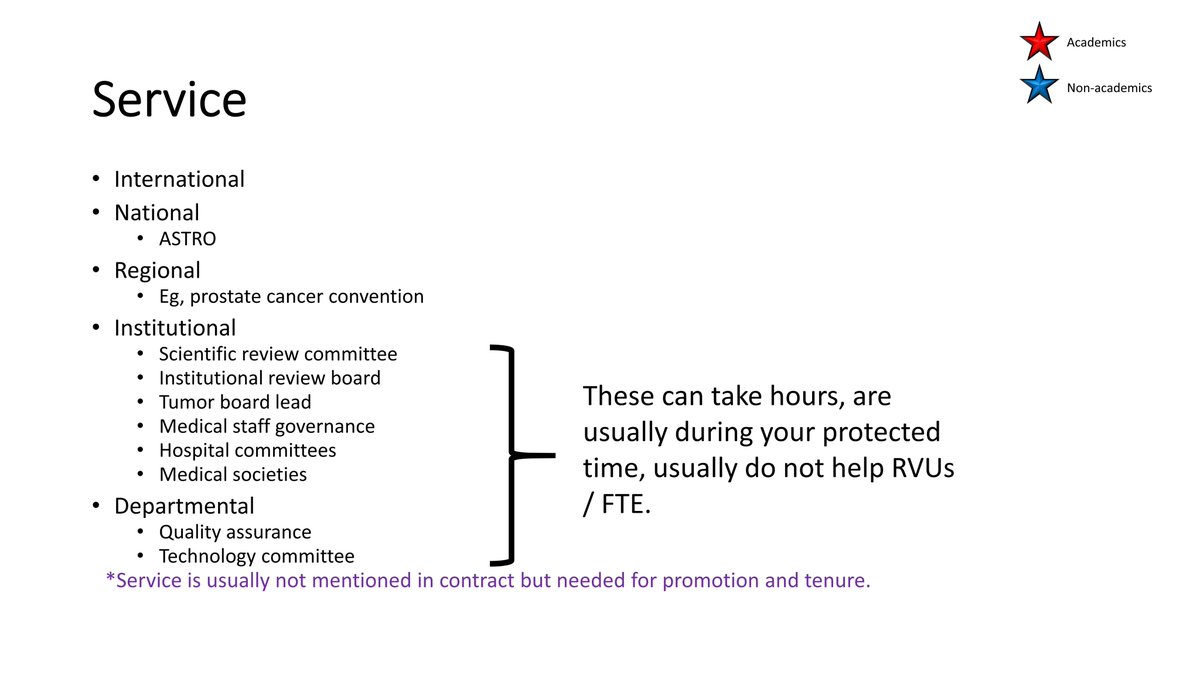
Both academicians and non-academicians also have a dedication to service:
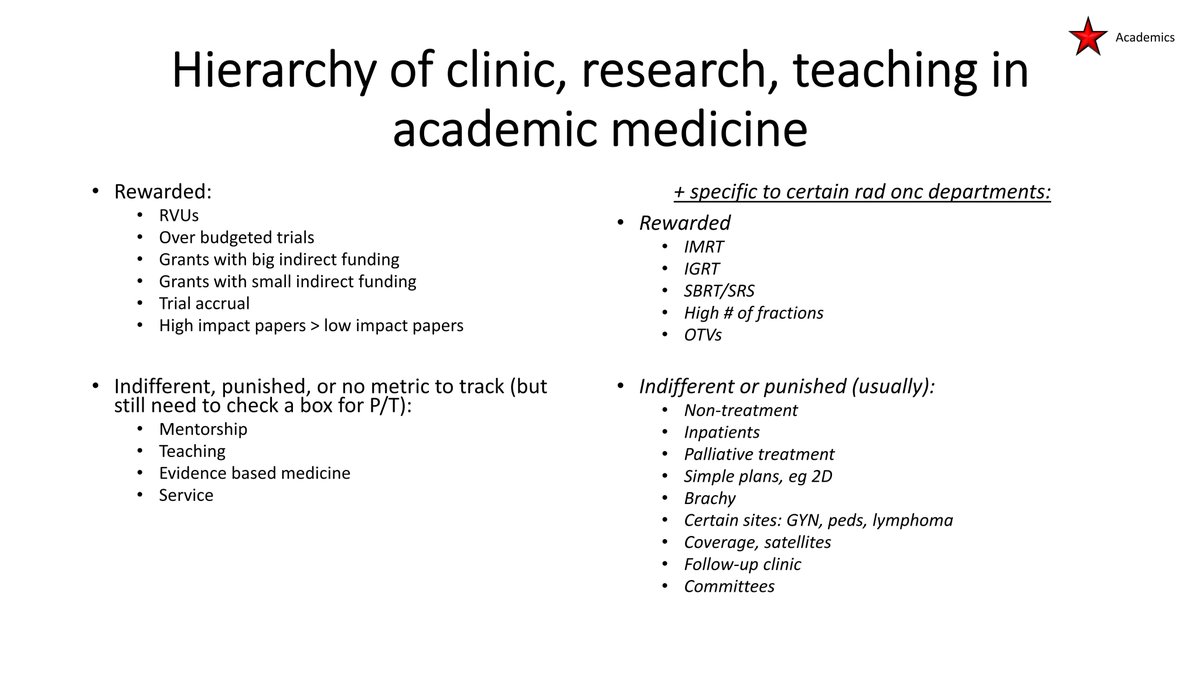
Academic medicine has a hierarchy for rewarding junior physicians.
For clinical care, until RVUs and payments can be made more equitable through @CMSGov and insurance companies, some services and physicians unfortunately will remain under-appreciated.
For clinical care, until RVUs and payments can be made more equitable through @CMSGov and insurance companies, some services and physicians unfortunately will remain under-appreciated.
Part 3: what to do in residency
Document everything:
Make a folder with licensure-related items.
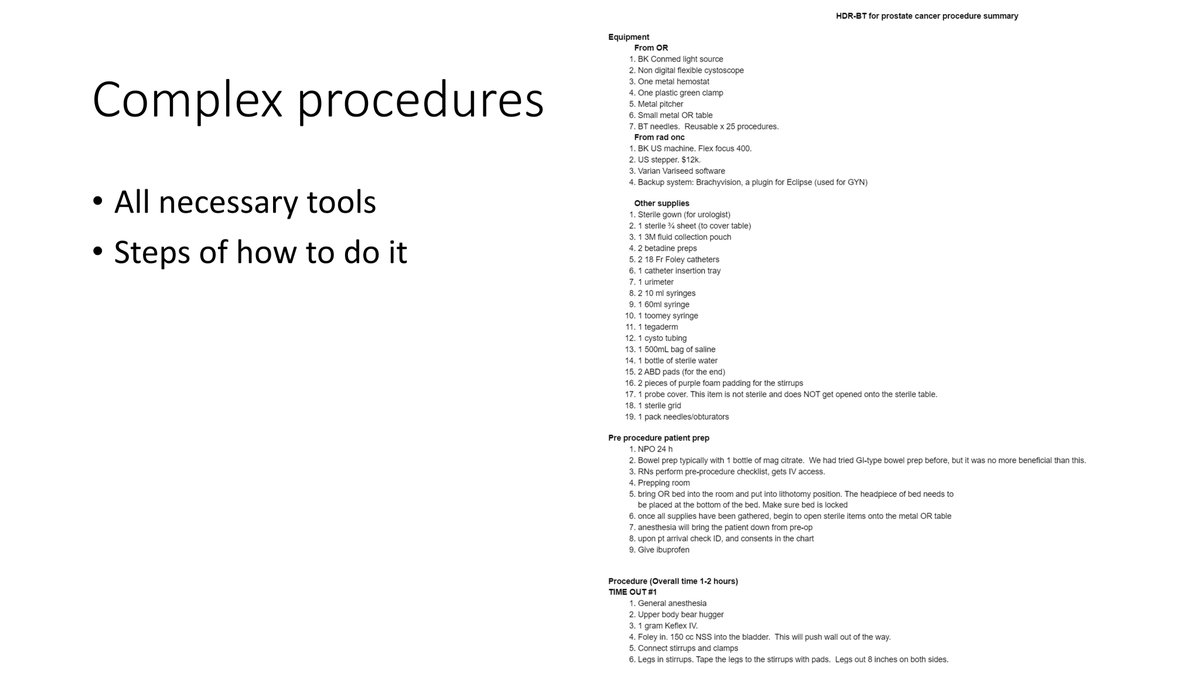
Write down the step-by-step guide of complex procedures.
Update your CV every few months.
Get your program to pay for training/equipment, eg DEA license, device training, books.
😃
amazon.com
Make a folder with licensure-related items.
Write down the step-by-step guide of complex procedures.
Update your CV every few months.
Get your program to pay for training/equipment, eg DEA license, device training, books.
😃
amazon.com

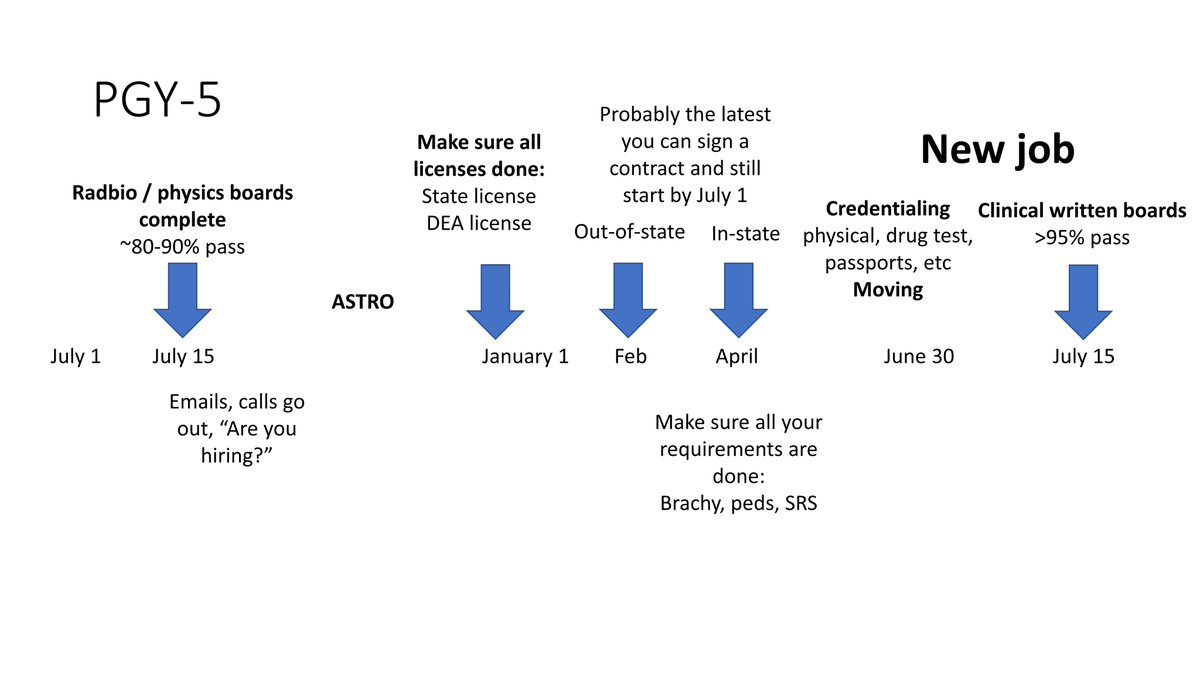
Considerations during PGY 2-5:
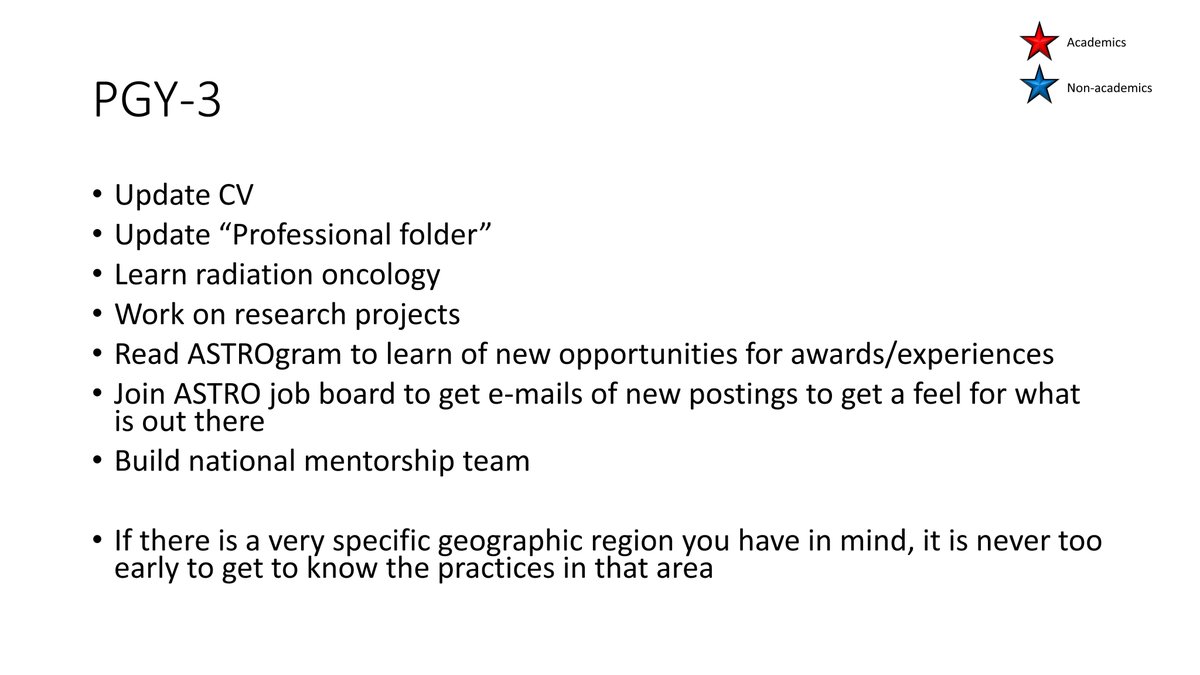
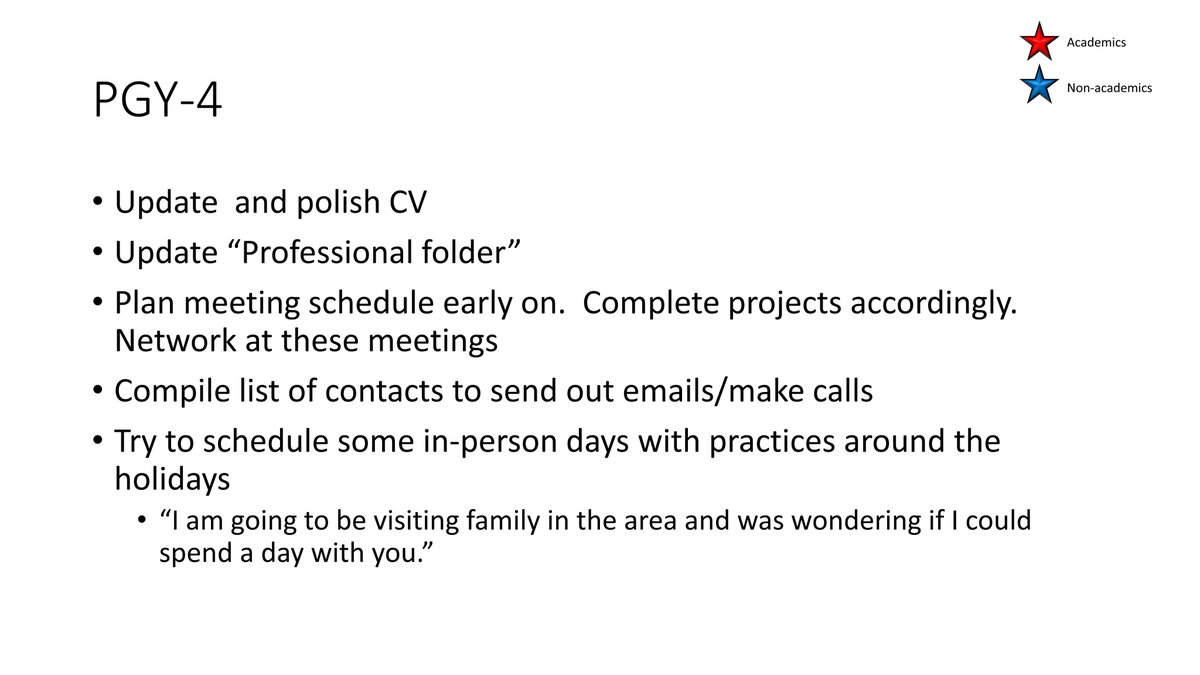
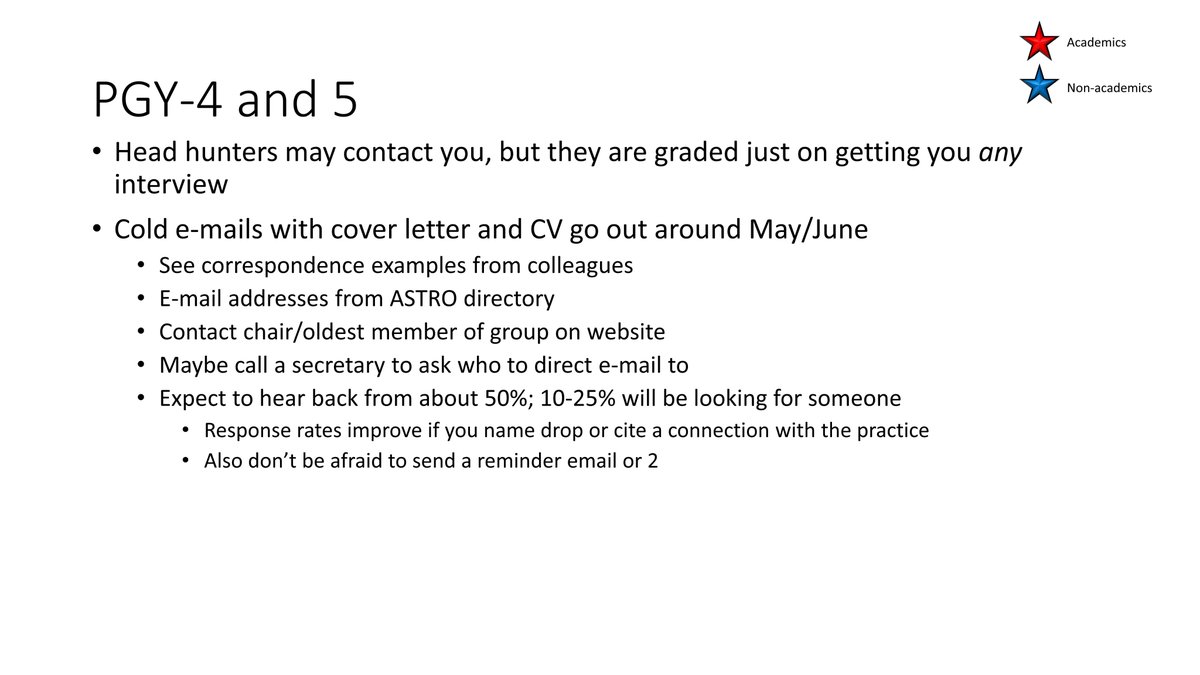
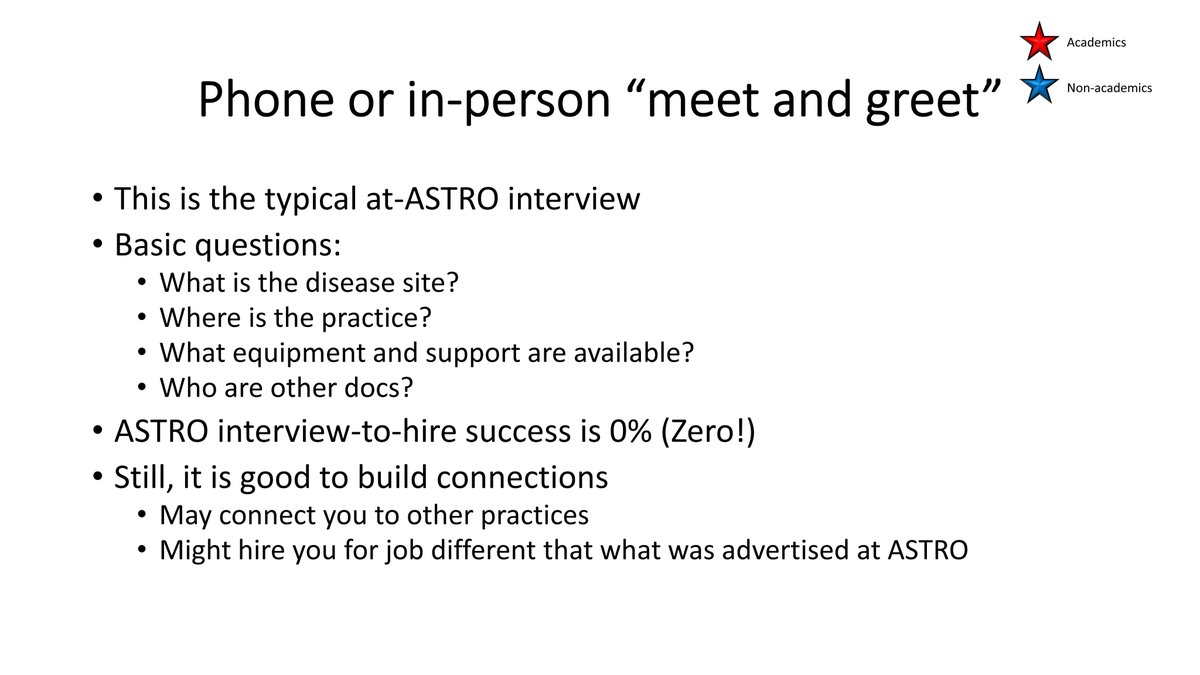
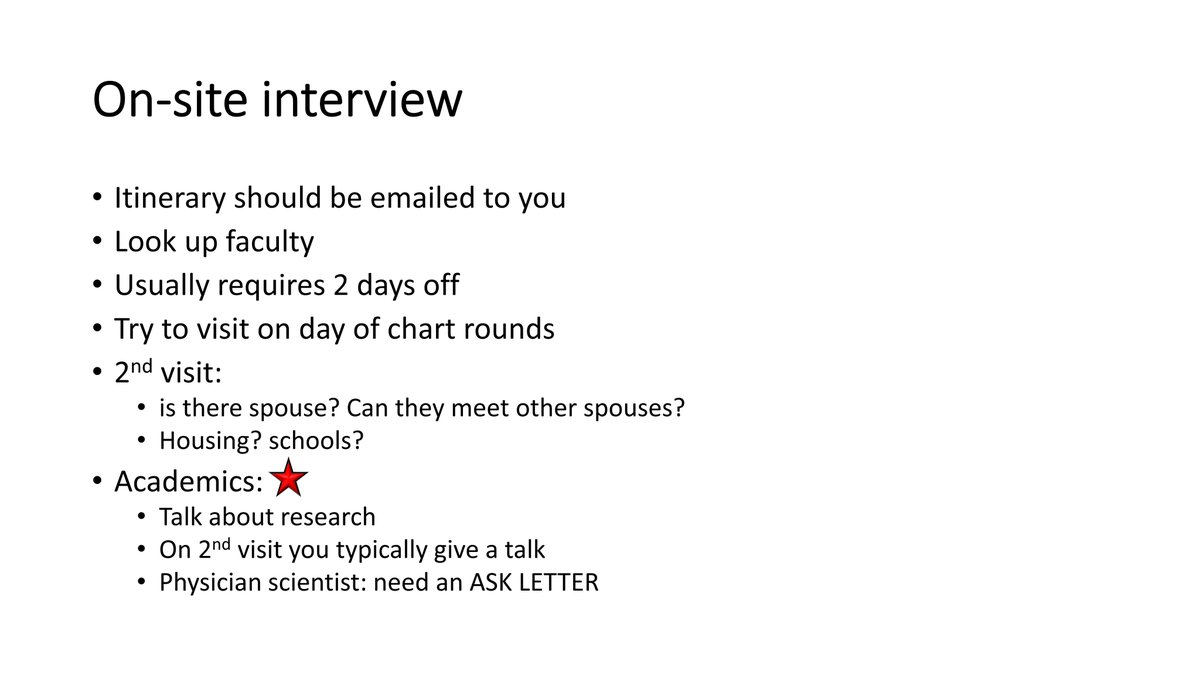
Usually PGY-5 is when most people are working on applications:
Each year at @ASTRO_org meeting, usually on Saturday before everything starts, @ARRO_org presents graduating resident surveys
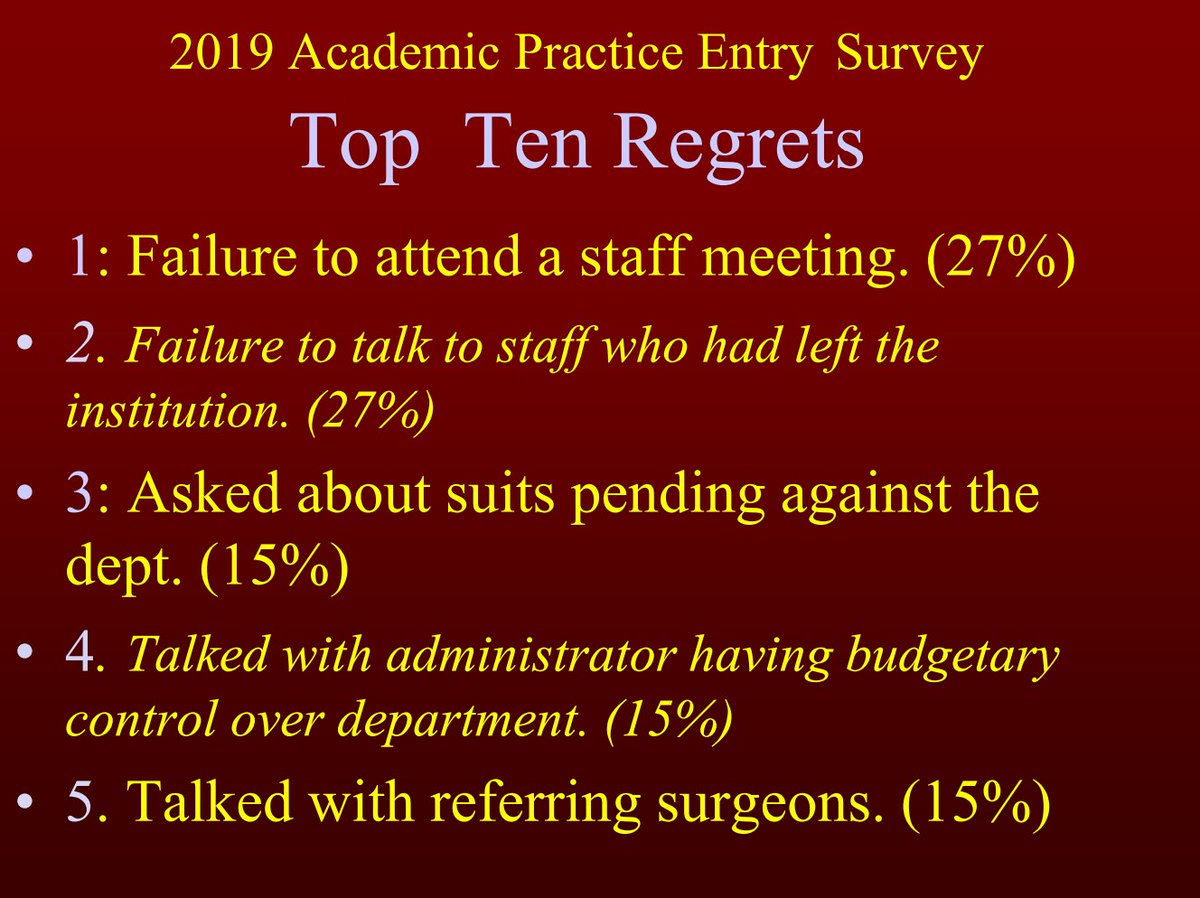
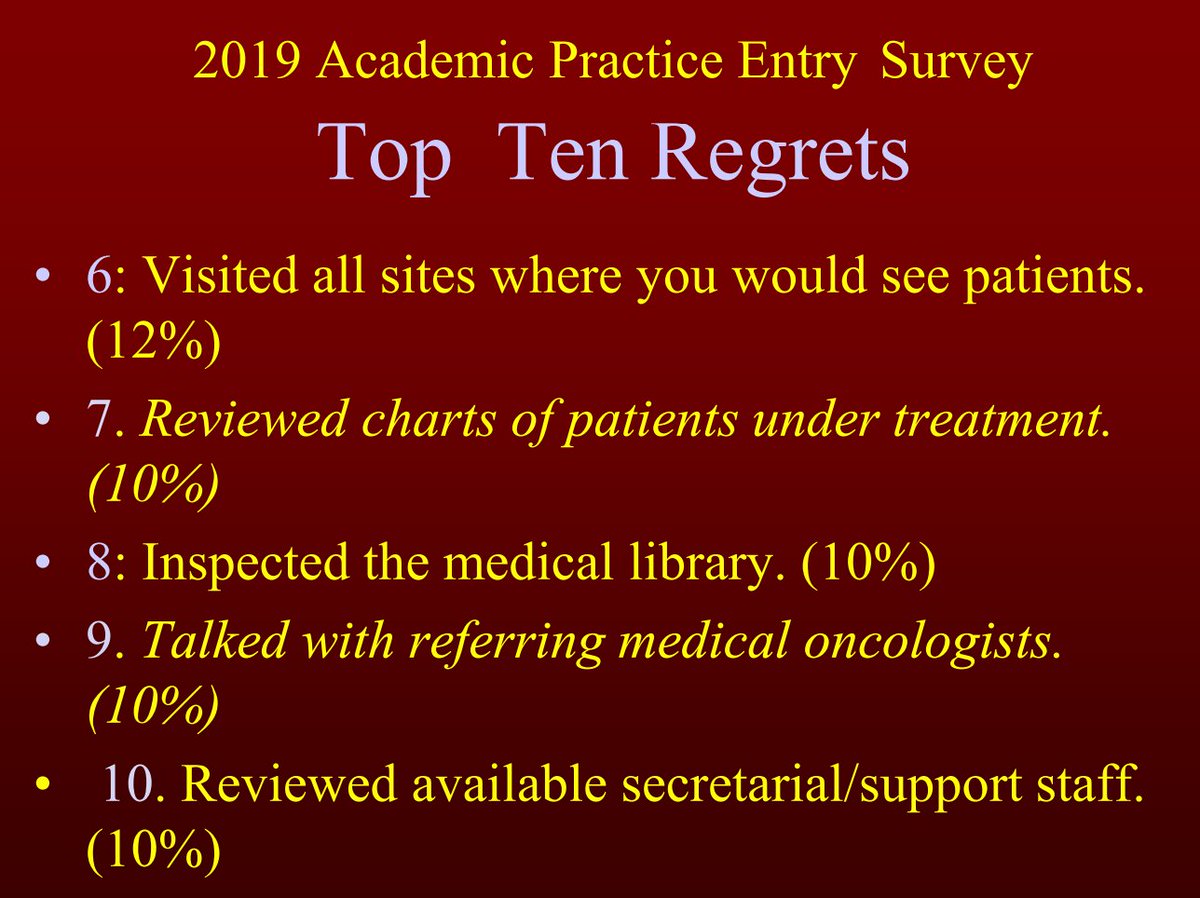
Also, Terry Wall provides the practice entry surveys
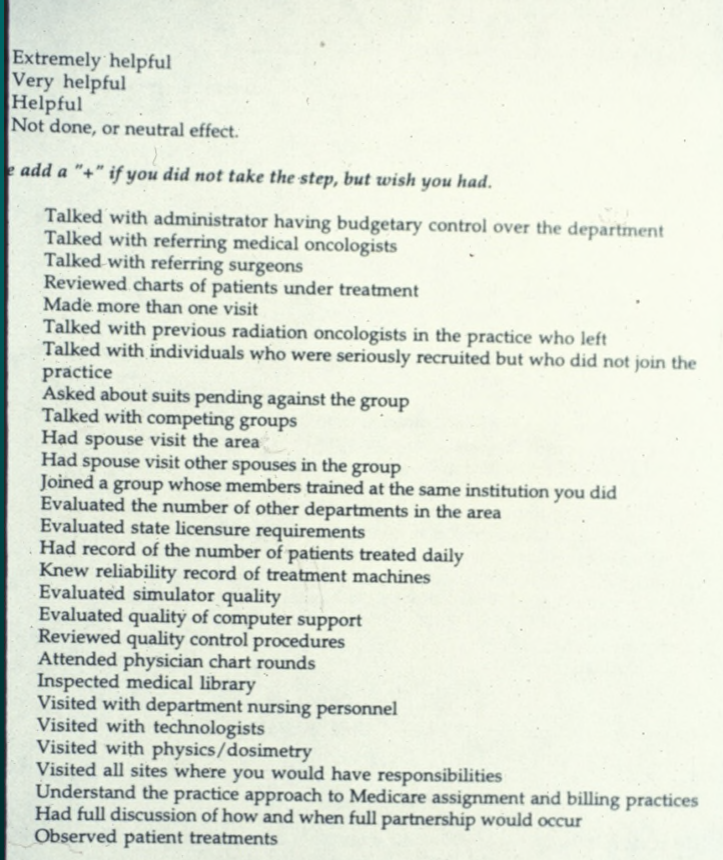
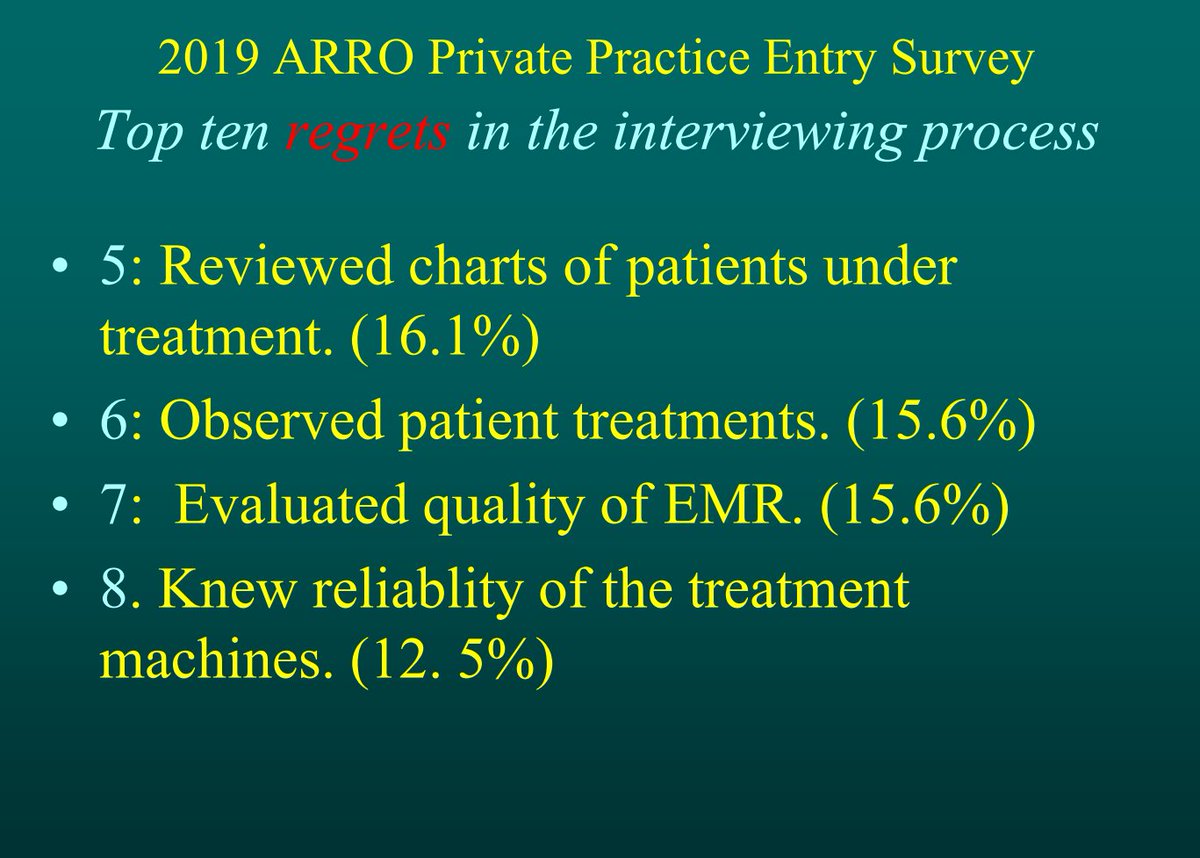
2019 ARRO private practice entry survey results for interview steps:

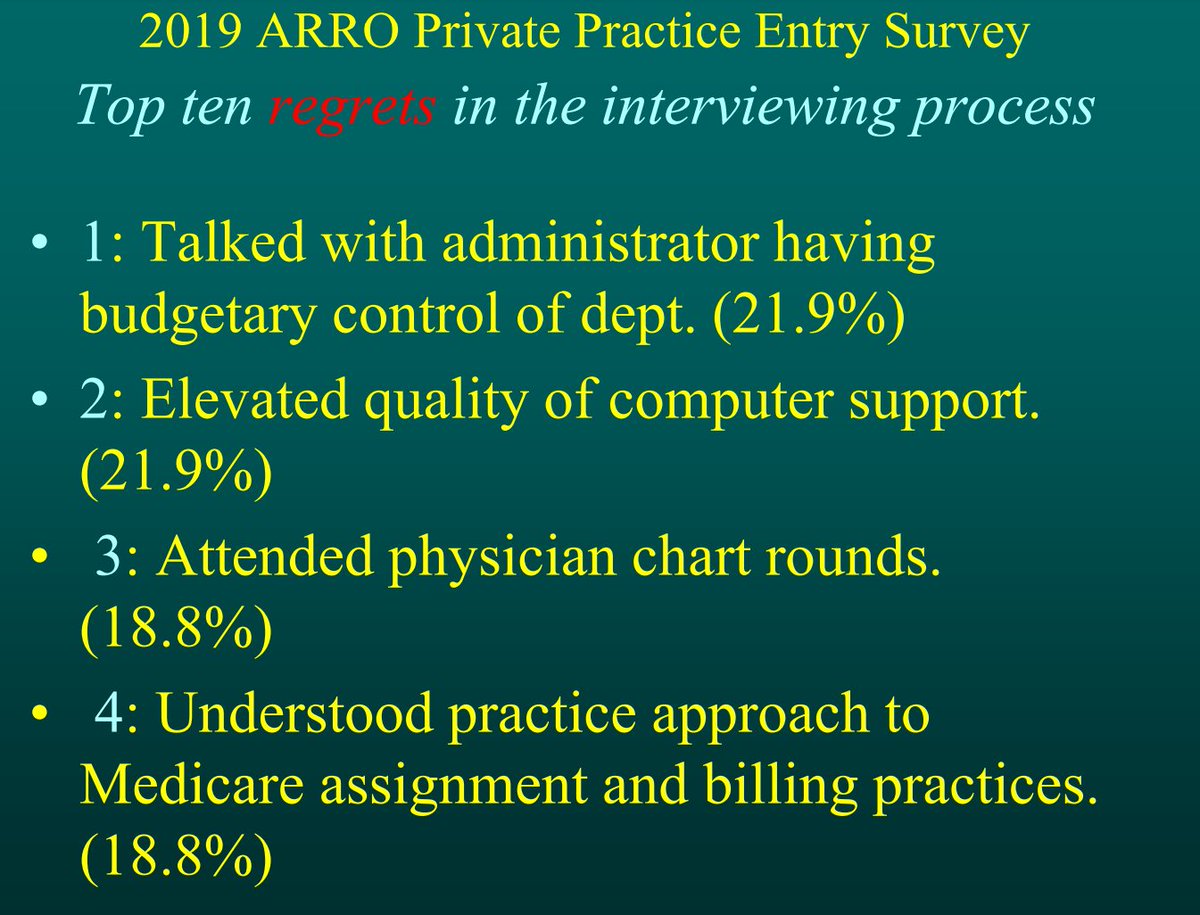
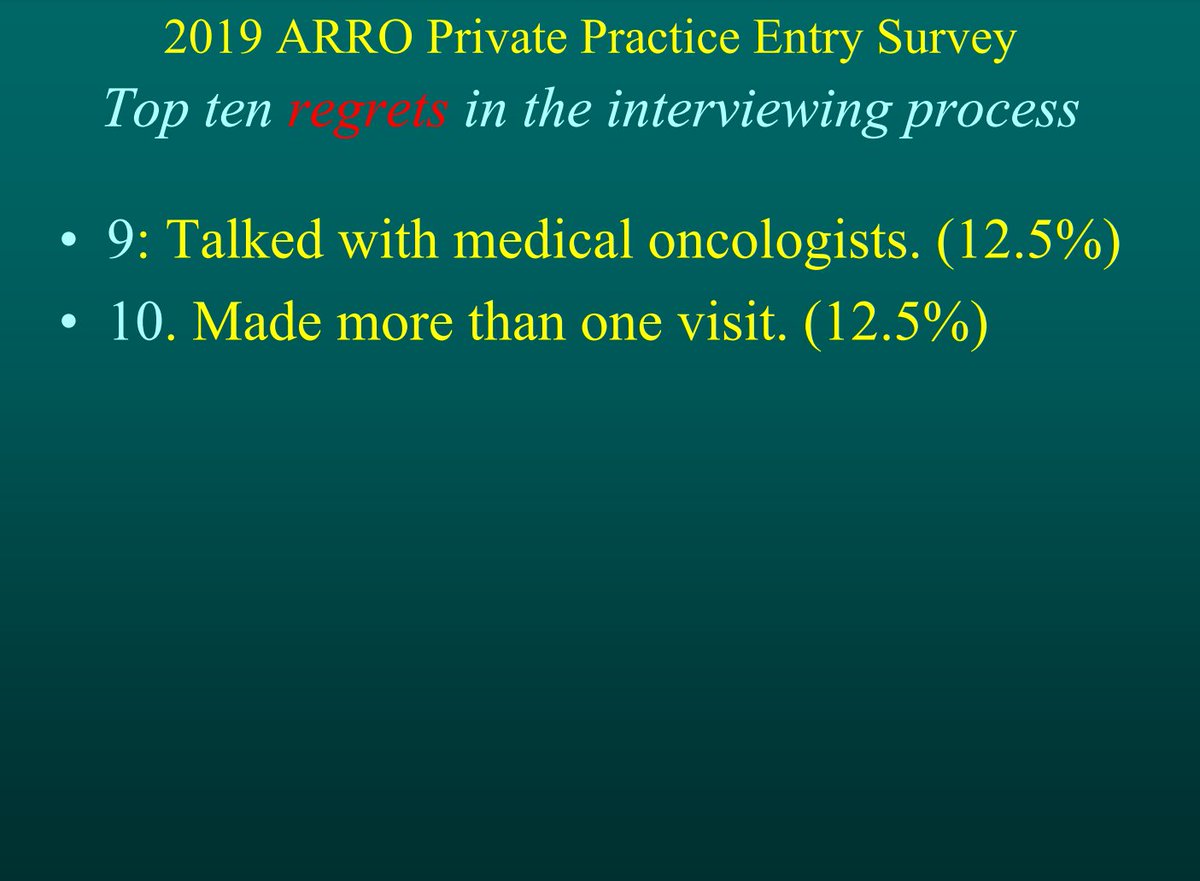
Top 10 interview regrets:
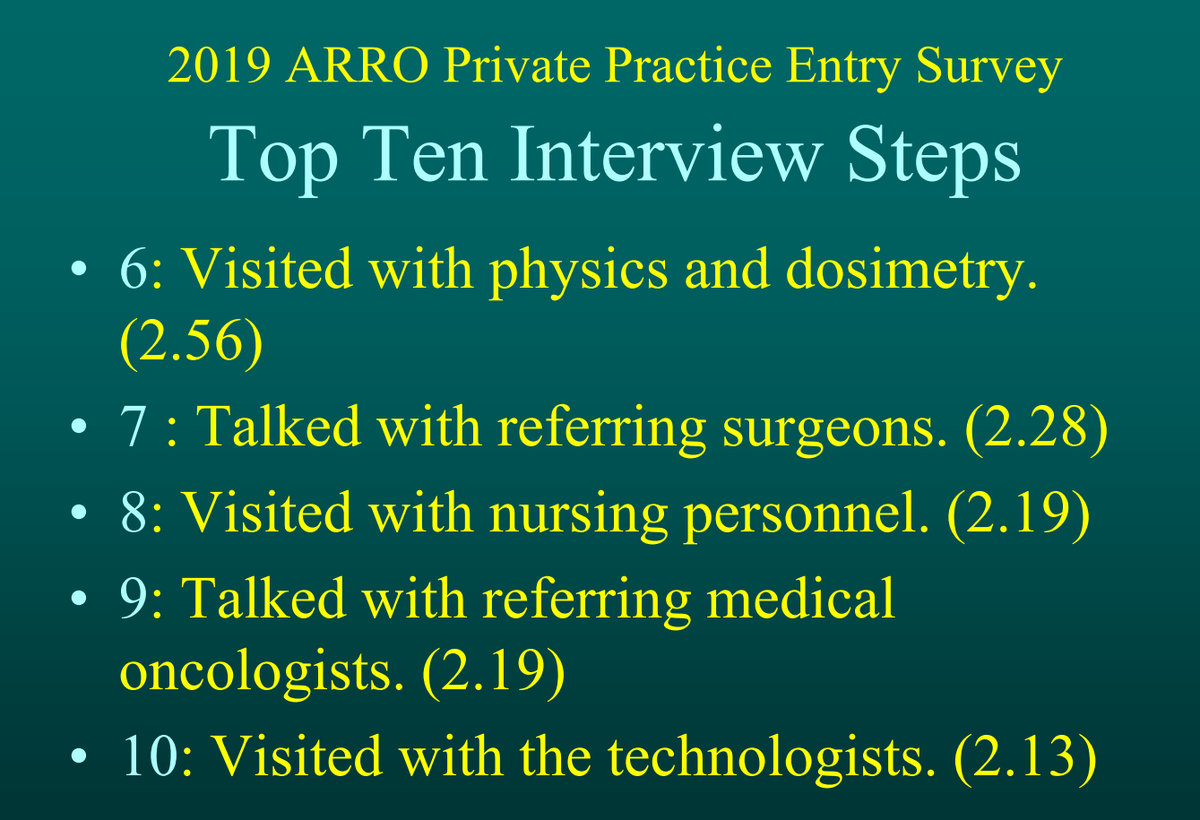
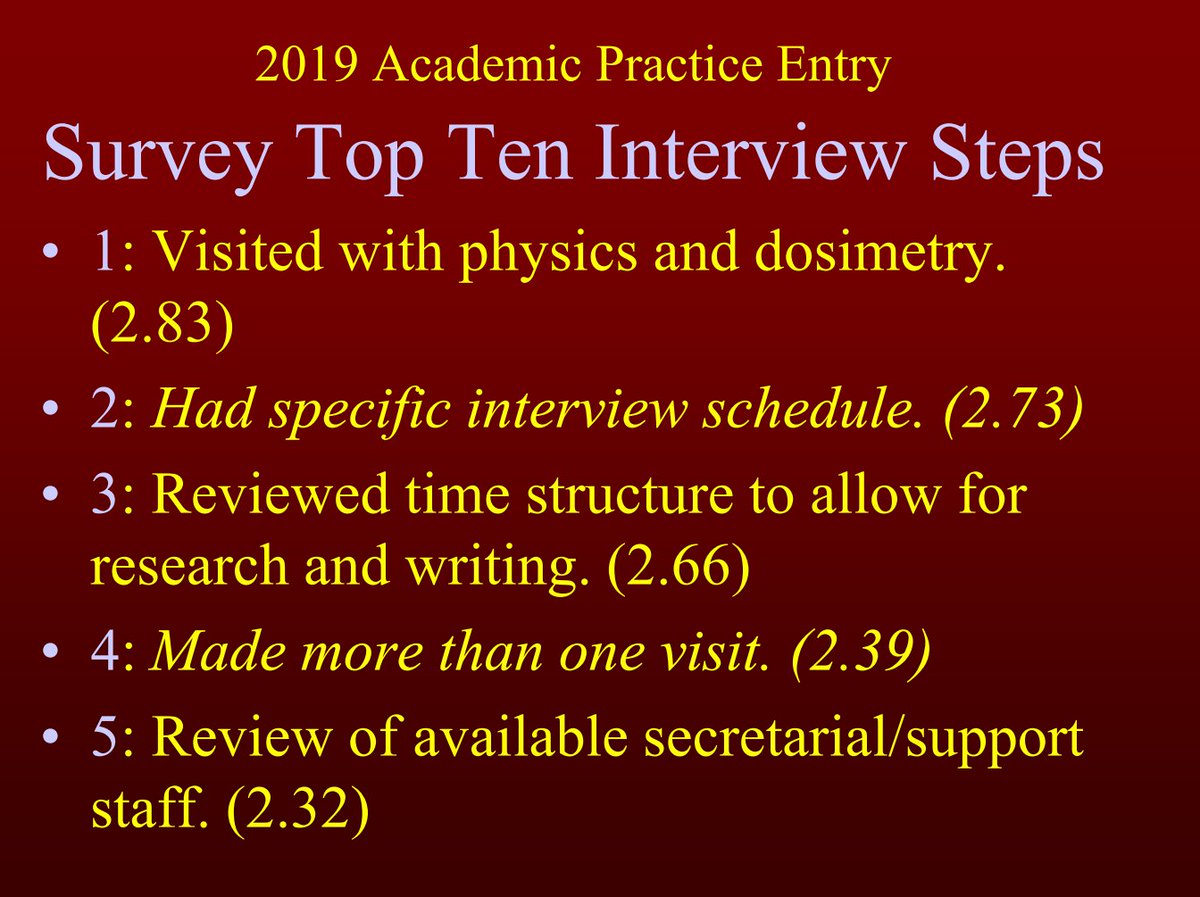
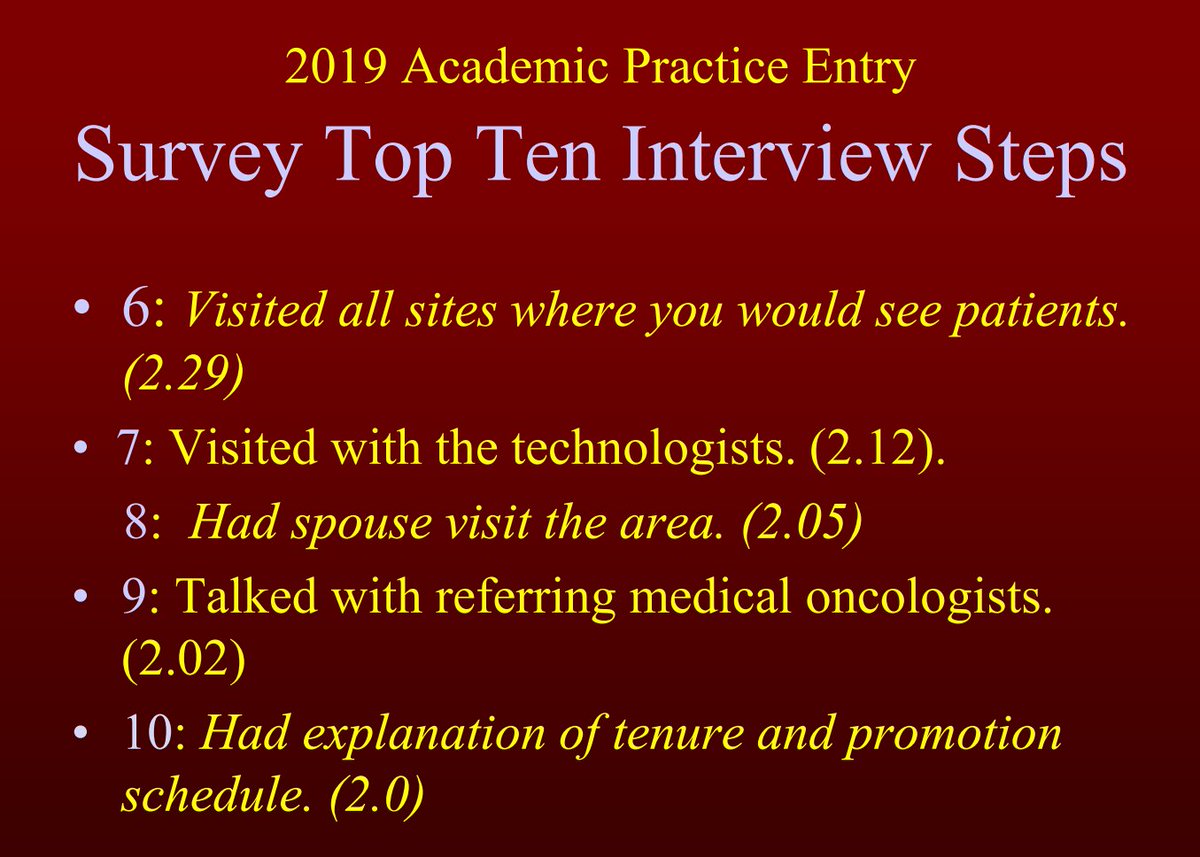
Top 10 interview steps in academics:
And the top 10 regrets in academics:
Loading suggestions...