

Ultimate Cardiac Thread for USMLE Step 2 CK
- This thread will help you become a MONSTER at cardio on the NBME's / IM shelf / Family Med shelf
- This thread will help you become a MONSTER at cardio on the NBME's / IM shelf / Family Med shelf
1) Long-QT syndrome --> implant cardiac defibrillator to prevent torsades!
For family med shelf: advise patient not to play sports due to risk of sudden cardiac death
For family med shelf: advise patient not to play sports due to risk of sudden cardiac death
2) Easy point: FIXED, split S2 = ASD (atrial septal defect)
3) Teenager with asymptomatic murmur that isn't affected by preload/afterload exercises (aka inspiration or valsalva)
Tx: NOTHING.
*If it's holosystolic, diastolic murmur or congenital heart issues, this will require workup aka ECHO (the answer seems to always be ECHO lol)
Tx: NOTHING.
*If it's holosystolic, diastolic murmur or congenital heart issues, this will require workup aka ECHO (the answer seems to always be ECHO lol)
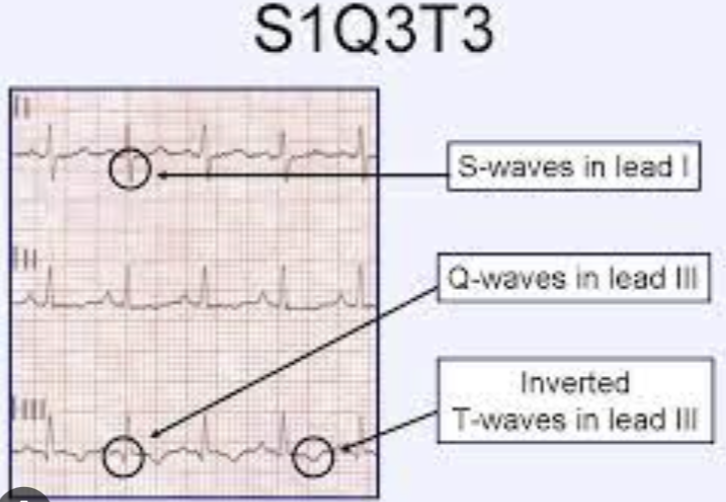
4) Chest pain + Decreased PCO2, decreased PO2, tachycardia, EKG with S1Q3T3 findings
--> This is NOT cardiac in nature! These findings indicate a Pulmonary Embolism.
Don't be fooled by the chest pain and EKG changes
--> This is NOT cardiac in nature! These findings indicate a Pulmonary Embolism.
Don't be fooled by the chest pain and EKG changes
5) Hepatojugular reflux & S3 or S4 = CHF
Bout to drop some knowledge...
Other conditions with hepatojugular reflux:
- R sided heart unable to accomodate increased preload:
a) CHF
b) R sided infarct
c) constrictive pericarditis
d) restrictive cardiomyopathy
Bout to drop some knowledge...
Other conditions with hepatojugular reflux:
- R sided heart unable to accomodate increased preload:
a) CHF
b) R sided infarct
c) constrictive pericarditis
d) restrictive cardiomyopathy
5a) NOTE: Cardiac Tamponade does NOT have increased hepatojugular reflux. Ez way to get tripped up **
6) SOB + Fever + HR > 100, Hypotension, perihilar fluid & cardiomegaly, decreased EF (usually 15-35% on questions) on ECHO =
ACUTE MYOCARDITIS
Question may give you coxsackievirus, parvo B19, doxorubicin usage, SLE/Sarcoid OR just a febrile illness as a clue
ACUTE MYOCARDITIS
Question may give you coxsackievirus, parvo B19, doxorubicin usage, SLE/Sarcoid OR just a febrile illness as a clue
6a) Myocarditis can be mild or legit heart failure (USUALLY tested in a younger patient to show you it's not an acute coronary syndrome!)
*Watch out for TQ saying "What is this condition associated with?"
- Arrhythmias due to conduction disruption (may mention PVC's for example)
*Watch out for TQ saying "What is this condition associated with?"
- Arrhythmias due to conduction disruption (may mention PVC's for example)
6b) Tx of Acute Myocarditis = supportive + tx underlying cause
**Many students think that because of LOW EF in myocarditis question stems, they need to send patient to cath lab. This is wrong!
**Many students think that because of LOW EF in myocarditis question stems, they need to send patient to cath lab. This is wrong!
7) Acute Pericarditis = can ALSO be SOB + Fever, but EKG will show WIDESPREAD ST elevations & PR depressions!
This is a money shot on your exam. Gotta know it.
Pericarditis will usually have NORMAL EF bc it isn't affecting the myocardium
This is a money shot on your exam. Gotta know it.
Pericarditis will usually have NORMAL EF bc it isn't affecting the myocardium
7a) Tx of Acute Pericarditis = anti-inflammatory meds (indomethacin, steroids or colchicine)
8) Constrictive Pericarditis = Chest pain that is WORSE with inspiration but BETTER with leaning forward
--> Murmur will be coarse, sandpaper friction rub
These patients will often have FEVER + hypotension + tachycardia too. So do NOT get thrown off. Look for key differences
--> Murmur will be coarse, sandpaper friction rub
These patients will often have FEVER + hypotension + tachycardia too. So do NOT get thrown off. Look for key differences
8a) Summary of high yield differences:
diastolic friction rub = constrictive pericarditis
widespread ST elevation = acute pericarditis
decreased EF = acute myocarditis
**Chest Pain WORSE when lying down = pericarditis until proven otherwise (get's better with leaning forward)
diastolic friction rub = constrictive pericarditis
widespread ST elevation = acute pericarditis
decreased EF = acute myocarditis
**Chest Pain WORSE when lying down = pericarditis until proven otherwise (get's better with leaning forward)
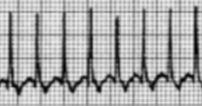
9) Regular, narrow complex EKG, exacerbated by EtOH / nicotine / caffeine / stress = PSVT (paroxysmal supraventricular tachycardia)
Tx: Vagal move (ice water over face, carotid sinus massage, coughing, valsalva)
If vagals fail --> adenosine
If UNSTABLE (low BP) = cardioversion
Tx: Vagal move (ice water over face, carotid sinus massage, coughing, valsalva)
If vagals fail --> adenosine
If UNSTABLE (low BP) = cardioversion
10) Murmur that is QUIETER with increased preload AND afterload = HOCM
11) Infective Endocarditis + New Murmur --> STAT REPEAT ECHO (likely has severe valvular damage)
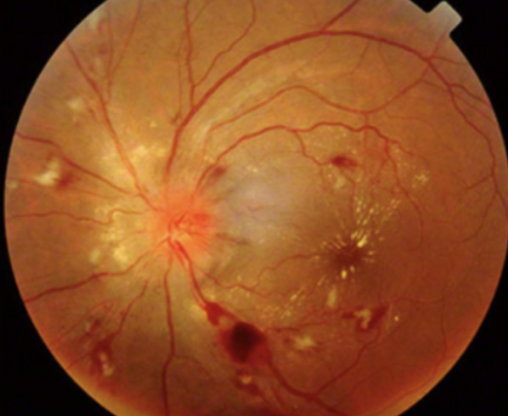
12) SEVERE HTN + Retinopathy:
- retinal hemorrhage (seen below)
- constricted retinal arterioles
- lobular choroidal infarcts
- hard exudates
**LINEAR INNER RETINA HEMORRHAGES ARE SEEN IN HTN RETINOPATHY
**Round hemorrhages of middle retina = diabetic retinopathy
- retinal hemorrhage (seen below)
- constricted retinal arterioles
- lobular choroidal infarcts
- hard exudates
**LINEAR INNER RETINA HEMORRHAGES ARE SEEN IN HTN RETINOPATHY
**Round hemorrhages of middle retina = diabetic retinopathy
13) BP Goal in adult < 140/90
BP goal in DM or CKD < 130/80
*They love this for Family Med Shelf
BP goal in DM or CKD < 130/80
*They love this for Family Med Shelf
14) Test-taking tip:
On the USMLE, don't pick slow ass scans like "radionuclide myocardial scan" or CTA, for patients in cardiac shock or having an MI!
They're more useful for outpatient workup of angina / CAD
On the USMLE, don't pick slow ass scans like "radionuclide myocardial scan" or CTA, for patients in cardiac shock or having an MI!
They're more useful for outpatient workup of angina / CAD
15) VSD can cause Failure to thrive! Look for a lil baby that fell off her weight/growth curve, SWEATS & FATIGUES during feeding + holosystolic murmur
- Cause L to R shunt = increased PAH --> can reverse the shunt from R to L (Eisenmenger syndrome)
- Cause L to R shunt = increased PAH --> can reverse the shunt from R to L (Eisenmenger syndrome)
16) Which Glycogen Storage Disease has cardiomegaly + cardiomyopathy?
POMPE! "it wrecks your PUMP" aka the heart
POMPE! "it wrecks your PUMP" aka the heart
17) This TQ is worth bookmarking
What has Kussmaul's sign?
(impaired RV filling)
- Restrictive cardiomyopathy
- RV infarct
- HUGE PE
- Tricuspid stenosis
- R sided CHF
- Chronic constrictive pericarditis (tx: pericardiectomy)
P.S. wtf is Kussmaul sign? JVD w/ inspiration
What has Kussmaul's sign?
(impaired RV filling)
- Restrictive cardiomyopathy
- RV infarct
- HUGE PE
- Tricuspid stenosis
- R sided CHF
- Chronic constrictive pericarditis (tx: pericardiectomy)
P.S. wtf is Kussmaul sign? JVD w/ inspiration
18) Treatment of cardiac tamponade
- Pericardiocentesis!
Watch for SBP decreasing 10mmHg during inspiration to dx aka pulsus paradoxus.
- Pericardiocentesis!
Watch for SBP decreasing 10mmHg during inspiration to dx aka pulsus paradoxus.
I had even more to add to this but Twitter wouldn’t let me make the thread any longer hahah
Lmk if this helped! I can work on some for the other systems for the USMLE.
- like/bookmark
- retweet
- drop a comment with any questions my friends!
Lmk if this helped! I can work on some for the other systems for the USMLE.
- like/bookmark
- retweet
- drop a comment with any questions my friends!
If you're a med student and would like to book a free call to discuss study strategy/classes/USMLE/COMLEX/rotations:
actionpotentialmentoring.com
actionpotentialmentoring.com

If you wanna ace the surgery questions, check this thread out too 🥳🥳
Here’s a Heme/onc thread I put together using previously tested concepts:
🩸🧵🩸🧵
🩸🧵🩸🧵
If you like this style of teaching & want to go through some high yields live, check this session out 👇👇
USMLE Step 2 CK - Top 20 TQ's to Know from NBME 12 in 2023
youtu.be
USMLE Step 2 CK - Top 20 TQ's to Know from NBME 12 in 2023
youtu.be
youtube.com
Don’t forget long QT syndrome!! It’s a bit more rare but I’ve seen it on NBME questions ;)
Don’t forget long QT syndrome!! It’s a bit more rare but I’ve seen it on NBME questions ;)

JUST RECORDED THE CARDIAC STEP 2 / IM Shelf REVIEW!
Subscribe on YouTube so you don’t miss it :)
@ActionPotentialMentoring" target="_blank" rel="noopener" onclick="event.stopPropagation()">youtube.com
Subscribe on YouTube so you don’t miss it :)
@ActionPotentialMentoring" target="_blank" rel="noopener" onclick="event.stopPropagation()">youtube.com

GI REVIEW 💩💩🔥
The Cardiac Review is LIVE on YouTube!
youtu.be
youtu.be
Loading suggestions...