

When I was an intern, I didn't even know what GDMT stood for.
It was challenging for me to keep track of all of the heart failure medications.
There weren't any great resources to help me remember the key medications.
So I made one.
Let's go through them.
- Thread -
1/20
It was challenging for me to keep track of all of the heart failure medications.
There weren't any great resources to help me remember the key medications.
So I made one.
Let's go through them.
- Thread -
1/20
Guideline-directed medical therapy (GDMT) for heart failure with reduced ejection fraction (HFrEF) targets the pathophysiological mechanisms that contribute to heart failure progression.
Check out the @pointofcaremed podcast on GDMT!
spotifyanchor-web.app.link
2/20
Check out the @pointofcaremed podcast on GDMT!
spotifyanchor-web.app.link
2/20


Goals of GDMT in HFrEF:
- improve survival
- reduce hospitalizations
- improve symptoms
GDMT achieves this by:
- reducing oxygen demand and wall stress
- decreasing heart rate and contractility of the heart
- reducing the resistance that the heart needs to pump against
3/20
- improve survival
- reduce hospitalizations
- improve symptoms
GDMT achieves this by:
- reducing oxygen demand and wall stress
- decreasing heart rate and contractility of the heart
- reducing the resistance that the heart needs to pump against
3/20

Some key terminology:
Preload - the volume of blood that is returned to the heart and present at the end of filling.
Afterload - the resistance the heart must overcome to eject blood during systole.
4/20
Preload - the volume of blood that is returned to the heart and present at the end of filling.
Afterload - the resistance the heart must overcome to eject blood during systole.
4/20

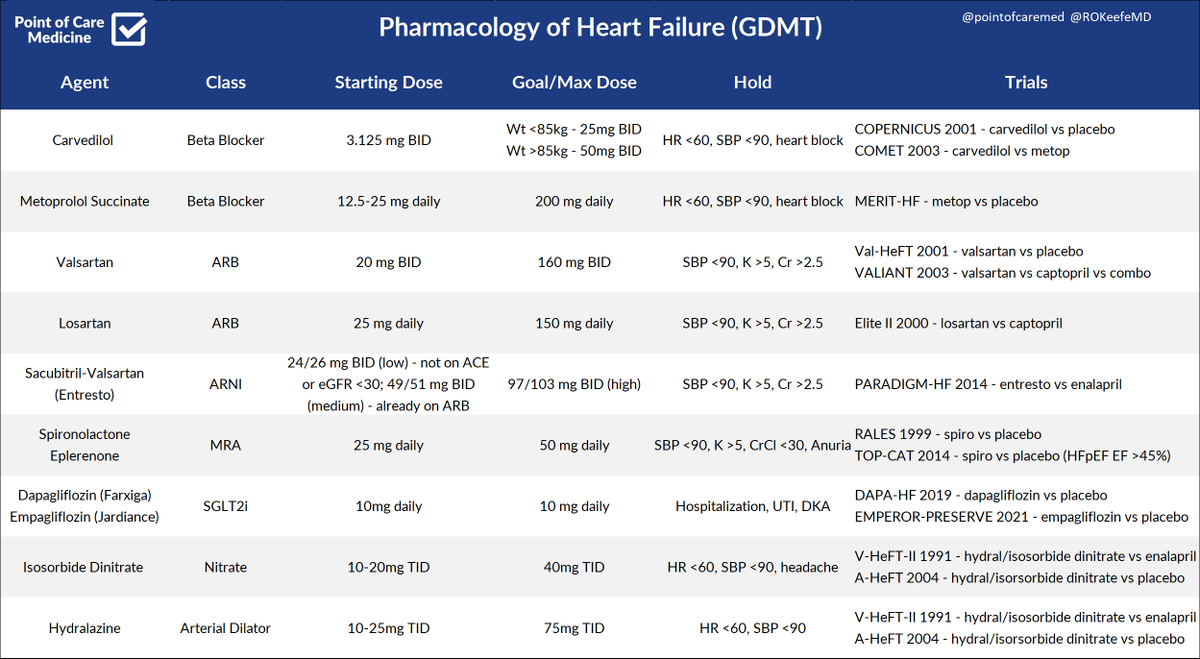
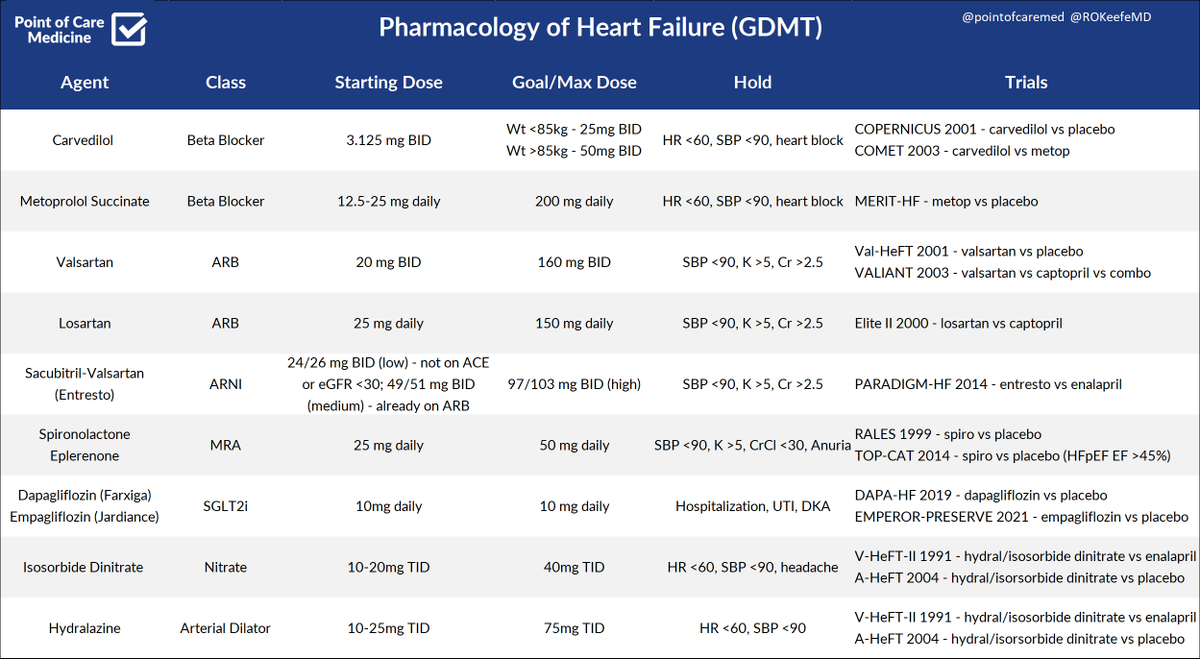
The Classes of Medications that Improve Mortality in HFrEF:
- Beta Blockers - carvedilol, metoprolol
- ACE/ARB/ARNI - lisinopril, losartan, valsartan, sacubitril/valsartan
- MRA - spironolactone, eplerenone
- SGLT2i - dapagliflozin, empagliflozin
5/20
- Beta Blockers - carvedilol, metoprolol
- ACE/ARB/ARNI - lisinopril, losartan, valsartan, sacubitril/valsartan
- MRA - spironolactone, eplerenone
- SGLT2i - dapagliflozin, empagliflozin
5/20
Beta Blockers
- Usually the first meds started in HFrEF
- Carvedilol is twice daily and non-selective - exerts more of a BP effect
- Metoprolol - daily, cardio-selective, more of a rate effect
- Hold HR <60 and SBP <90
6/20
- Usually the first meds started in HFrEF
- Carvedilol is twice daily and non-selective - exerts more of a BP effect
- Metoprolol - daily, cardio-selective, more of a rate effect
- Hold HR <60 and SBP <90
6/20

ACE and ARBs
- inhibit RAAS, reduce afterload, prevent remodeling
- Watch renal fucntion and potassium
- ACE can lead to dry cough, angioedema
- Valsartan more robust effect on mortality and is dosed twice daily (shorter half-life); Losartan is less studied, dosed daily
7/20
- inhibit RAAS, reduce afterload, prevent remodeling
- Watch renal fucntion and potassium
- ACE can lead to dry cough, angioedema
- Valsartan more robust effect on mortality and is dosed twice daily (shorter half-life); Losartan is less studied, dosed daily
7/20

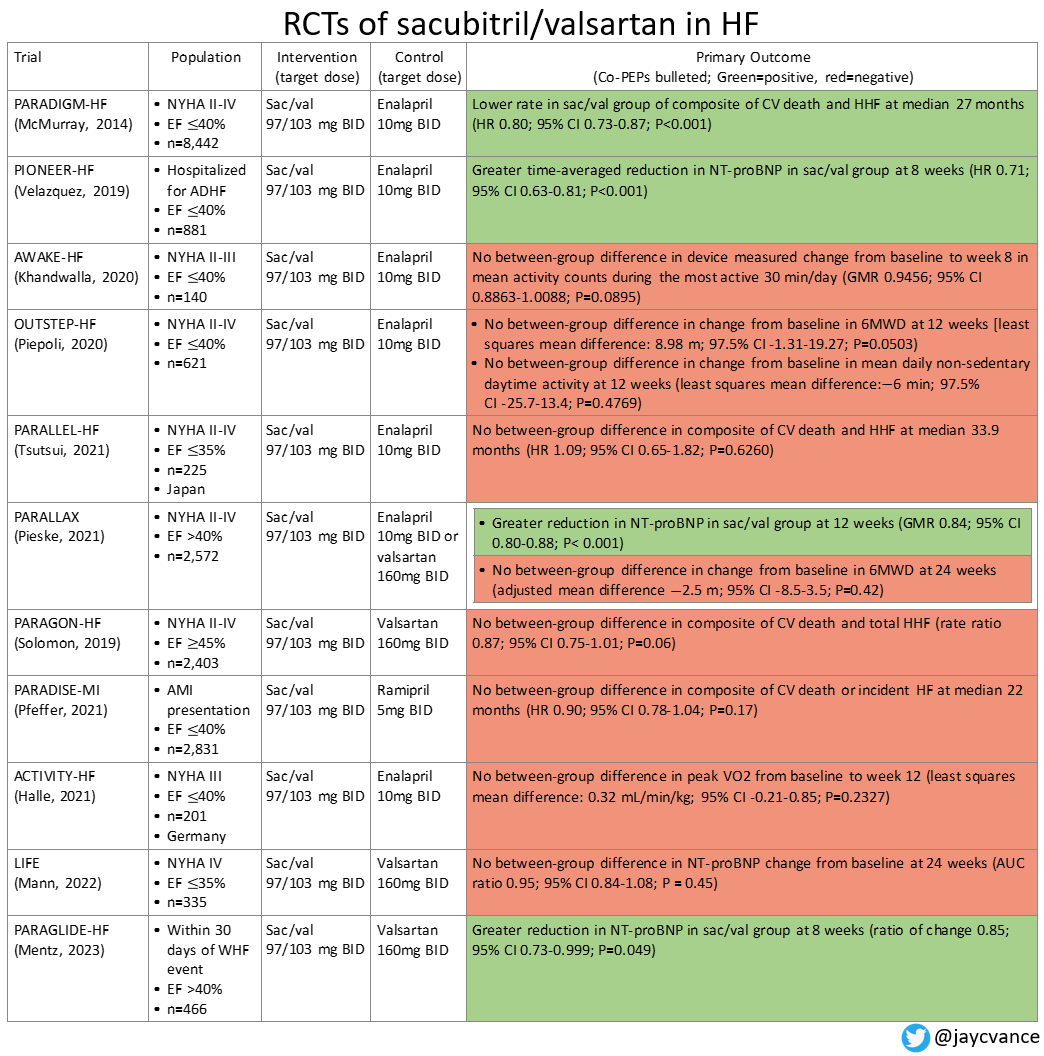
ARNI - sacubitril/valsartan (Entresto)
- inhibits neprilysin and blocks RAAS
- morality benefit over ACE, but only shown biomarker improvements over ARBs
- Go slow - titrating the dose up too fast can commonly lead to hypotension
8/20
- inhibits neprilysin and blocks RAAS
- morality benefit over ACE, but only shown biomarker improvements over ARBs
- Go slow - titrating the dose up too fast can commonly lead to hypotension
8/20

Awesome table from @javcvance on all of the trials (as of 2023) for ARNI's.
9/20
9/20
Mineralocorticoid Receptor Antagonists (MRAs)
- prevent hypokalemia associated with loop diuretics
- start if symptoms despite max tolerated BB and ACE/ARB/ARNI
- spironolactone antagonizes androgen receptor - gynecomastia
- eplerenone leads to fewer side effects
10/20
- prevent hypokalemia associated with loop diuretics
- start if symptoms despite max tolerated BB and ACE/ARB/ARNI
- spironolactone antagonizes androgen receptor - gynecomastia
- eplerenone leads to fewer side effects
10/20

SGLT2 Inhibitors
- inhibit glucose re-absorption in kidney
- unclear why they work in heart failure patients without diabetes
- monitor for dehydration, UTIs, Fournier's gangrene, and euglycemic DKA
- hold while inpatient
11/20
- inhibit glucose re-absorption in kidney
- unclear why they work in heart failure patients without diabetes
- monitor for dehydration, UTIs, Fournier's gangrene, and euglycemic DKA
- hold while inpatient
11/20

Isosorbide Dinitrate and Hydralazine
- usually second-line after other GDMT
- nitrates dilate the venous system, hydralazine the arterial system
- nitrates can lead to headaches, flushing, reflex tachy
- hydral can lead to BP lability and is dosed 3-4 times daily
12/20
- usually second-line after other GDMT
- nitrates dilate the venous system, hydralazine the arterial system
- nitrates can lead to headaches, flushing, reflex tachy
- hydral can lead to BP lability and is dosed 3-4 times daily
12/20
Initiating and Titrating GDMT
- goal to achieve the target or maximally tolerated doses within 3-6 months
- ideally titrated every 1-2 weeks via telehealth visit with monitoring of vitals and labs
13/20
- goal to achieve the target or maximally tolerated doses within 3-6 months
- ideally titrated every 1-2 weeks via telehealth visit with monitoring of vitals and labs
13/20

- start with a BB if not decompensated
- can add ACE/ARB/ARNI at the same time if there is BP room
- add MRA if still symptoms and not hyperkalemic - will not lower BP
- SGLT2i can be added before or after MRA
- repeat echo 3-6 months after doses are optimized
14/20
- can add ACE/ARB/ARNI at the same time if there is BP room
- add MRA if still symptoms and not hyperkalemic - will not lower BP
- SGLT2i can be added before or after MRA
- repeat echo 3-6 months after doses are optimized
14/20
Barriers to Optimal GDMT
- polypharmacy and difficulty with adherence
- complexity of care coordination
- discontinuation with decompensations
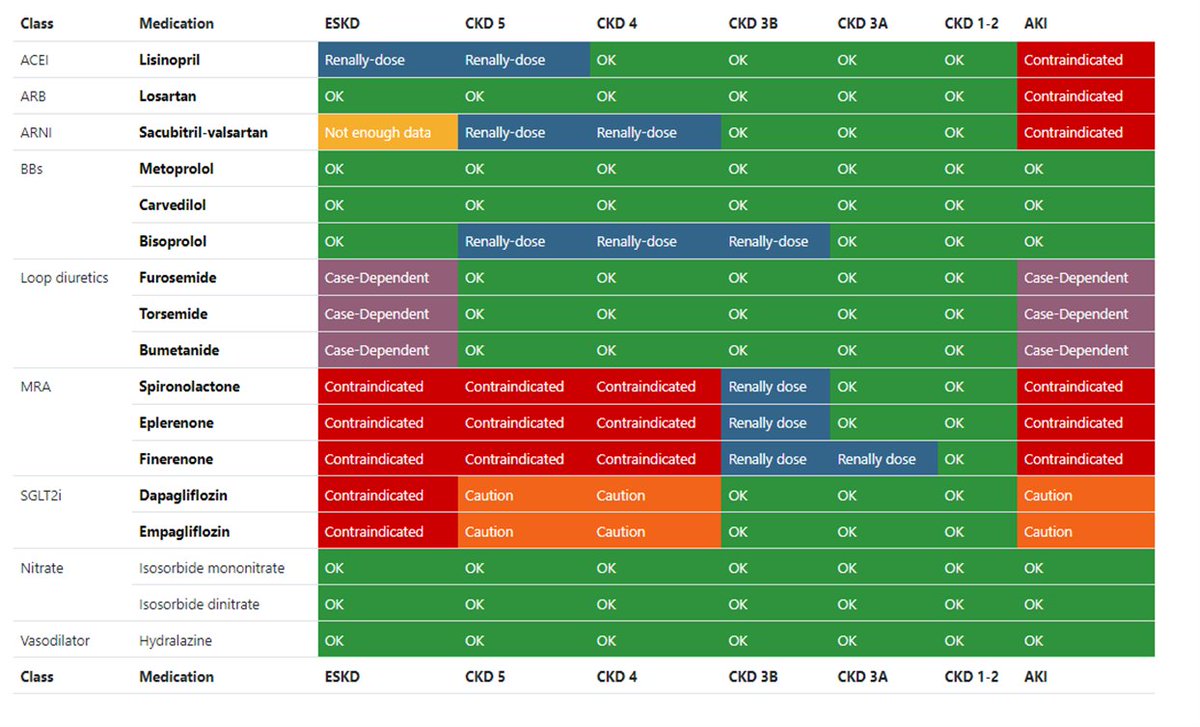
- uncertainty with CKD
- cost and access
- geriatric patient and those with frailty have different risk/benefit ratios
15/20
- polypharmacy and difficulty with adherence
- complexity of care coordination
- discontinuation with decompensations
- uncertainty with CKD
- cost and access
- geriatric patient and those with frailty have different risk/benefit ratios
15/20


GDMT For Everyone
- graphics on whether agents can be used at different CKD levels
- links to key literature
- interactive consultant tool
gdmt.org
Thanks to Dr. Jiawei Tan and Dr. Jiun-Ruey Hu for this amazing resource!
17/20
- graphics on whether agents can be used at different CKD levels
- links to key literature
- interactive consultant tool
gdmt.org
Thanks to Dr. Jiawei Tan and Dr. Jiun-Ruey Hu for this amazing resource!
17/20

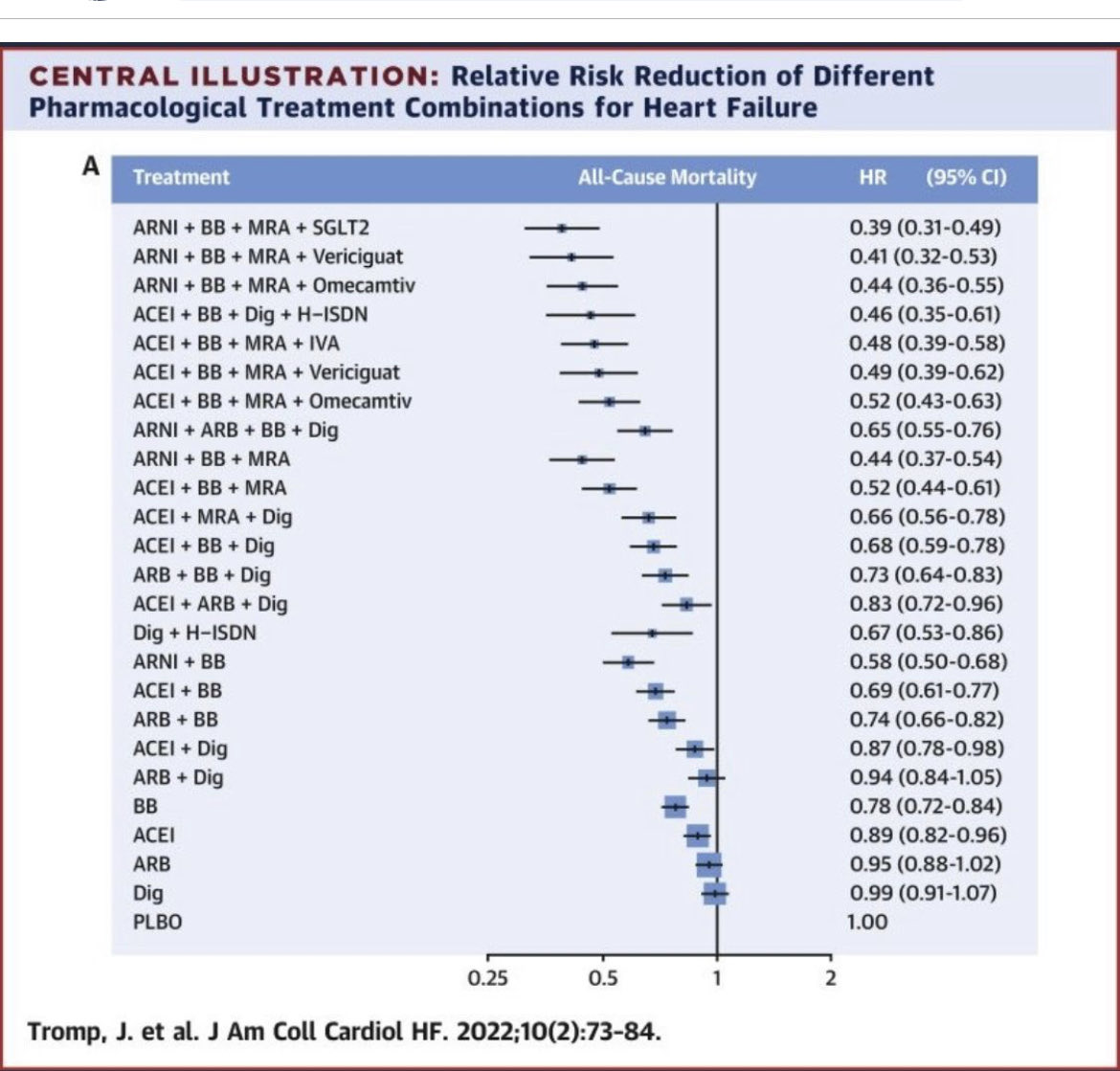
An elegant graphic showing how the HR's for all-cause mortality improve based on adding each extra GDMT medication.
Thanks to @2scottish for bringing it to my attention
18/20
Thanks to @2scottish for bringing it to my attention
18/20
I hope you've found this thread helpful.
Follow me @ROKeefeMD for more.
Like/Retweet the first tweet below if you can:
19/20
Follow me @ROKeefeMD for more.
Like/Retweet the first tweet below if you can:
19/20
You can read the unrolled version of this thread here: typefully.com
20/20
20/20

Loading suggestions...