

Today I’m going to cover some basics of asthma. 🫁
Most of this content comes from this year’s GINA report.
Most of this content comes from this year’s GINA report.

Asthma is characterized by chronic airway inflammation, VARIABLE symptoms, and VARIABLE airflow limitation/airway hyperresponsiveness.
It is a clinical diagnosis, not a spirometric one as spiro findings are “not necessary or sufficient to make the diagnosis.”
It is a clinical diagnosis, not a spirometric one as spiro findings are “not necessary or sufficient to make the diagnosis.”
For a primer on obstruction (airflow limitation), start here with the beginning of this thread on COPD.
Now this emphasis on VARIABLE symptoms and VARIABLE airflow limitation can make asthma tricky to diagnose.
Whereas an initial COPD history can sometimes feel straightforward, an asthma history requires a lot of digging: family history, childhood history, environmental allergies, eczema, GERD, nasal polyps, sinus history, NSAIDs, triggers, etc.
Because asthma can be difficult to diagnose and there are many mimics, you should always aim to TEST BEFORE YOU TREAT.
Trying to sort out the diagnosis once someone is on therapy can be exceptionally difficult.
Trying to sort out the diagnosis once someone is on therapy can be exceptionally difficult.
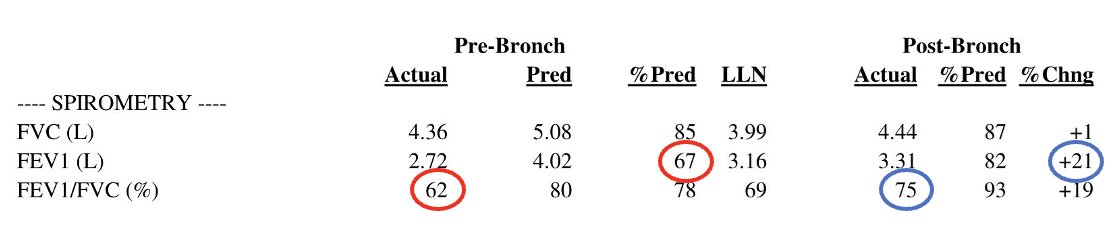
Initial testing with PFTs can show the classic obstruction with complete reversibility of the defect after administration of an inhaled bronchodilator. This makes your life easy, diagnostically speaking.
If your PFTs are unrevealing though (as MANY will be), your next stop is a bronchoprovocation test.
I have only ever used methacholine, which is a muscarinic agonist (opposite of a LAMA).
Higher and higher doses are given, and a drop of 20% from baseline FEV1 is significant.
I have only ever used methacholine, which is a muscarinic agonist (opposite of a LAMA).
Higher and higher doses are given, and a drop of 20% from baseline FEV1 is significant.
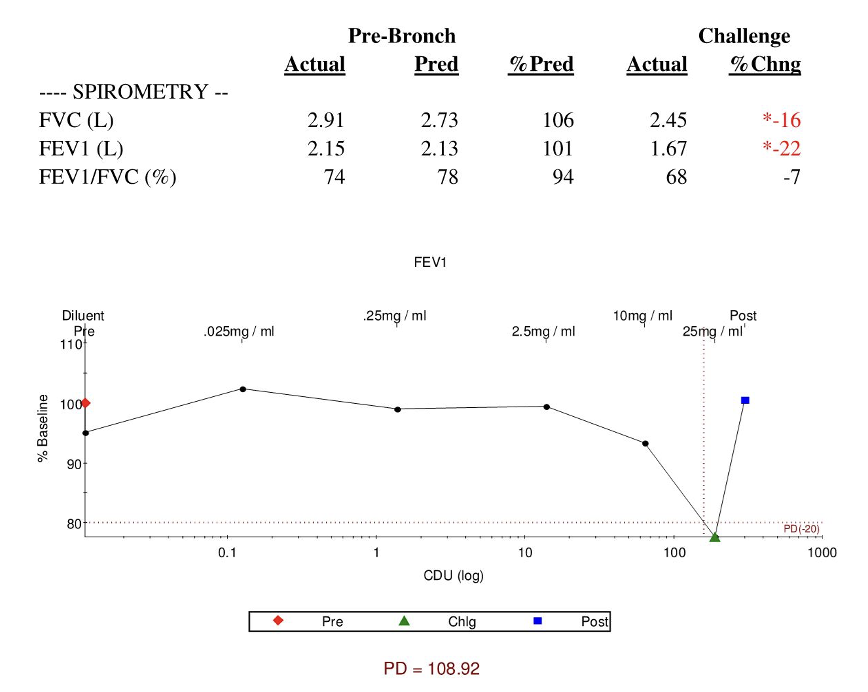
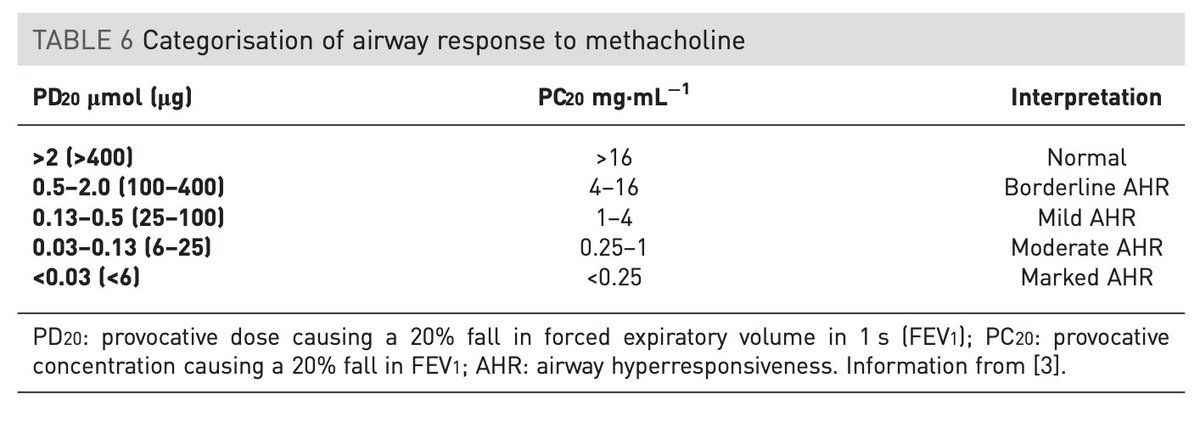
The PD20 can be used to grade the hyperresponsiveness. (ATS/ERS 2017)
Methacholine challenges have moderate sensitivity, but limited specificity.
Methacholine challenges have moderate sensitivity, but limited specificity.
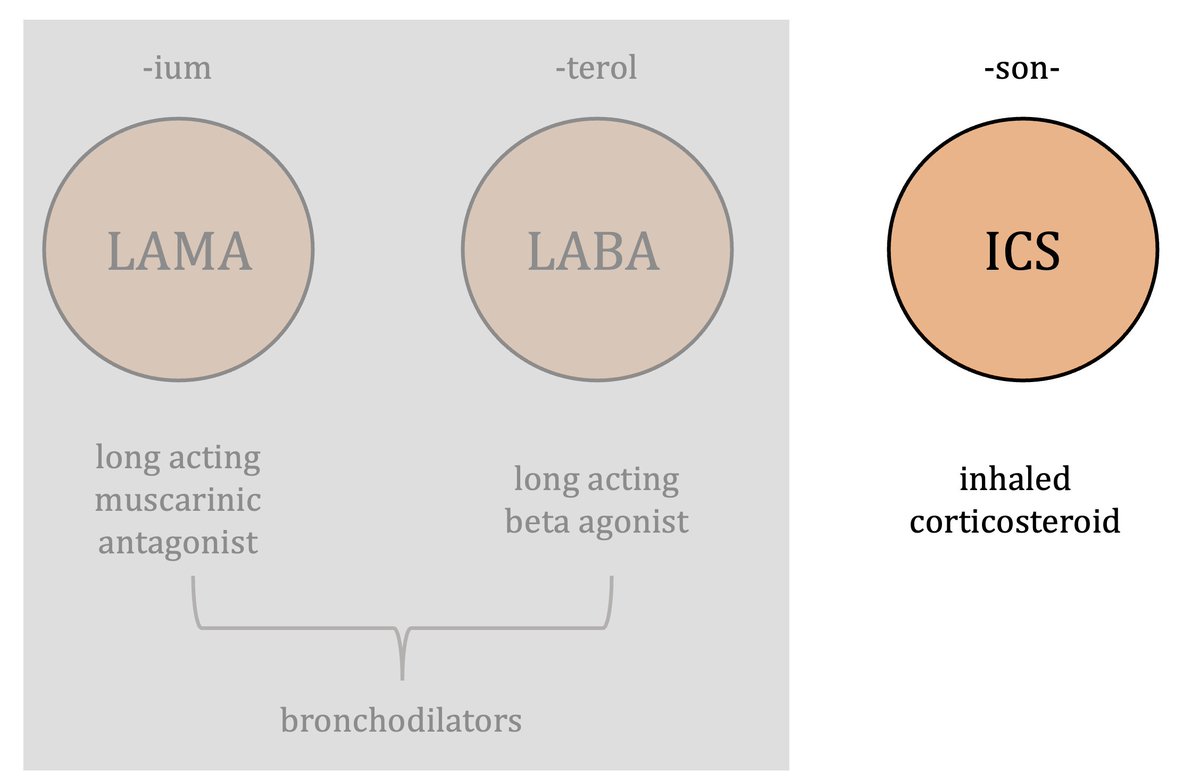
Once you have diagnosed asthma, you have the same inhaled meds that you have in COPD but ICS is the star here and bronchodilators (particularly LAMAs) really take a back seat.
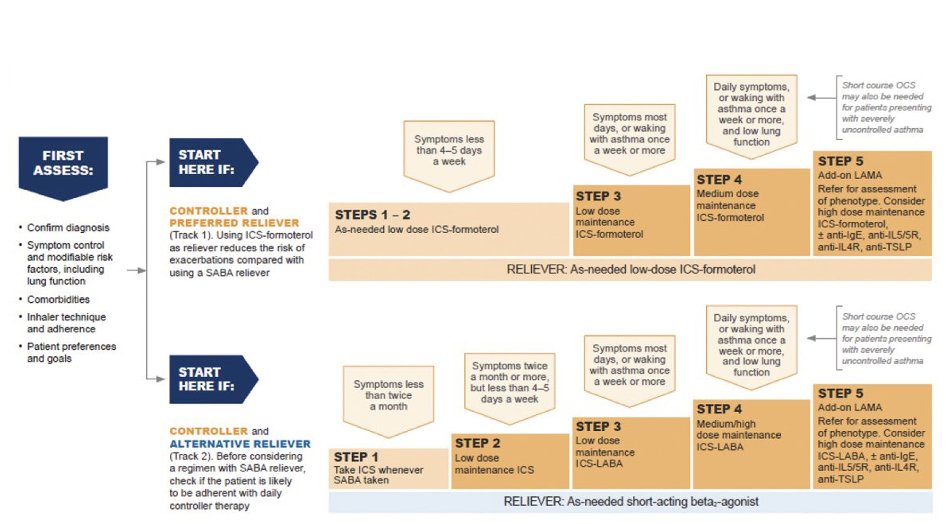
GINA does a really great job of summarizing asthma management here.
You can look along the top and based on how often your patient is having symptoms, it tells you what therapy to start. You can then step therapy up or down depending on their control.
You can look along the top and based on how often your patient is having symptoms, it tells you what therapy to start. You can then step therapy up or down depending on their control.
🚨KEY POINT: NO ONE with asthma should be on just a bronchodilator!
Every patient with a diagnosis of asthma should be getting an inhaled steroid, whether daily or just PRN (steps 1-2).
SABA alone increases risk of severe exacerbation/hospitalization compared with LABA/ICS.
Every patient with a diagnosis of asthma should be getting an inhaled steroid, whether daily or just PRN (steps 1-2).
SABA alone increases risk of severe exacerbation/hospitalization compared with LABA/ICS.
Notice that the different steps involve different doses of ICS. This means you have to know which ICS and how much you’re using. The # of puffs for these inhalers matter.
This chart from @pyrlsapp is a thing of beauty. Use it to ensure you're RXing what you say you're RXing.
This chart from @pyrlsapp is a thing of beauty. Use it to ensure you're RXing what you say you're RXing.

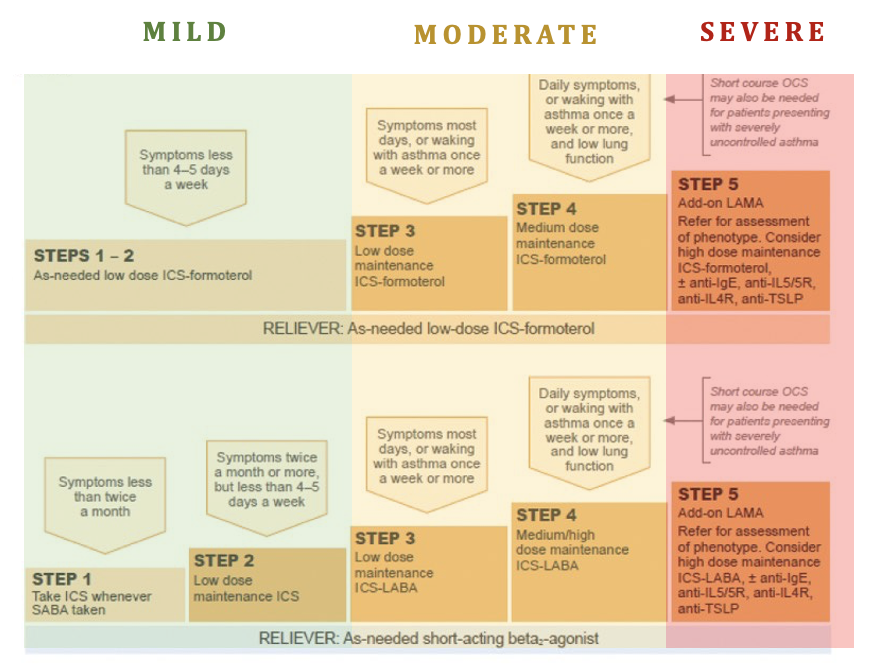
Assessing asthma should be done retrospectively based on how difficult they’ve been to treat. GINA breaks it down like this.
And the thing with asthma is it can be a moving target. So you start therapy, see them back to assess control, adjust as needed, then start again.
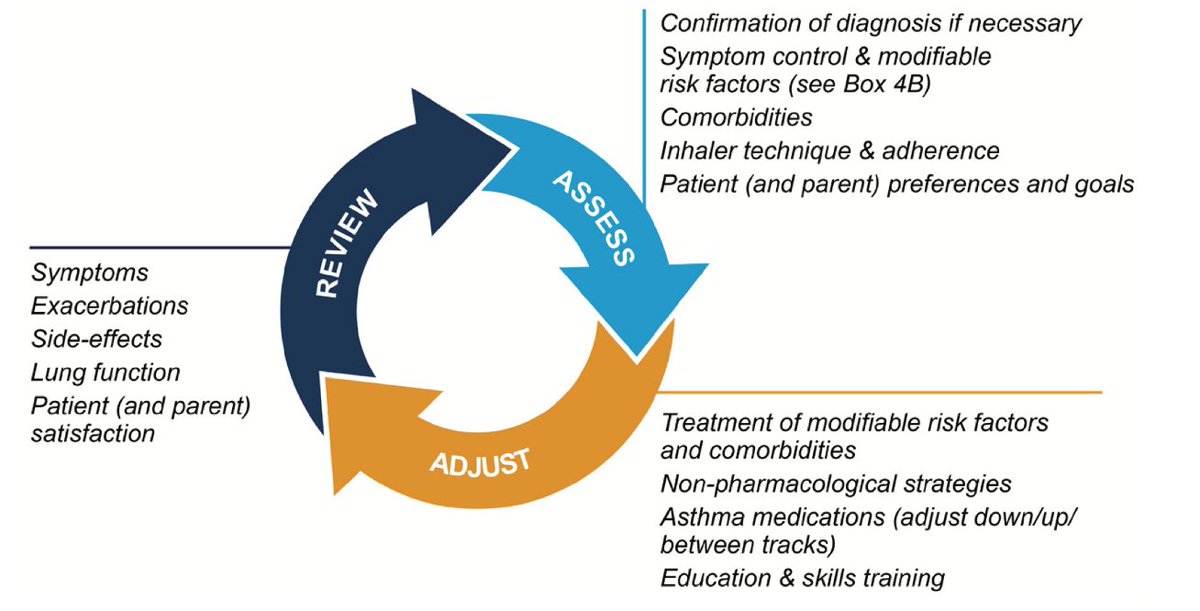
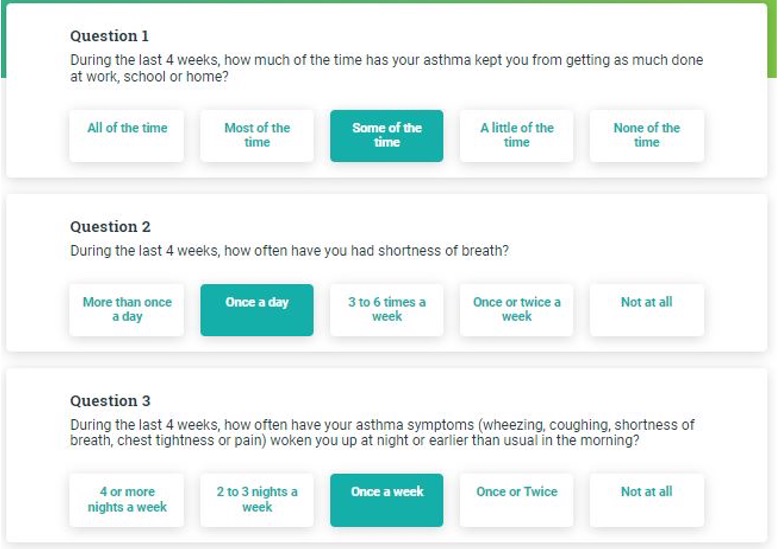
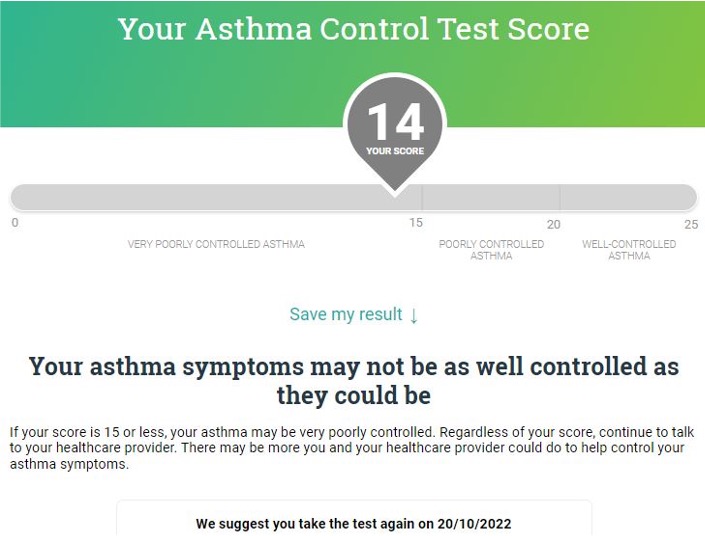
My favorite way to reassess asthma is by using the asthma control test. It’s a 5 question test that I just pull up on my phone and do with them in the room and then document. It gives a number that is sort of an objective way to follow the patient’s symptoms visit to visit.
A few words on severe asthma (patients on step 5 of the GINA step up guidelines).
We are finding that there are different types/phenotypes of asthma. In severe asthma, it’s helpful to look for signs of T2-High asthma. I always send a CBC w/ diff + eos.
We are finding that there are different types/phenotypes of asthma. In severe asthma, it’s helpful to look for signs of T2-High asthma. I always send a CBC w/ diff + eos.
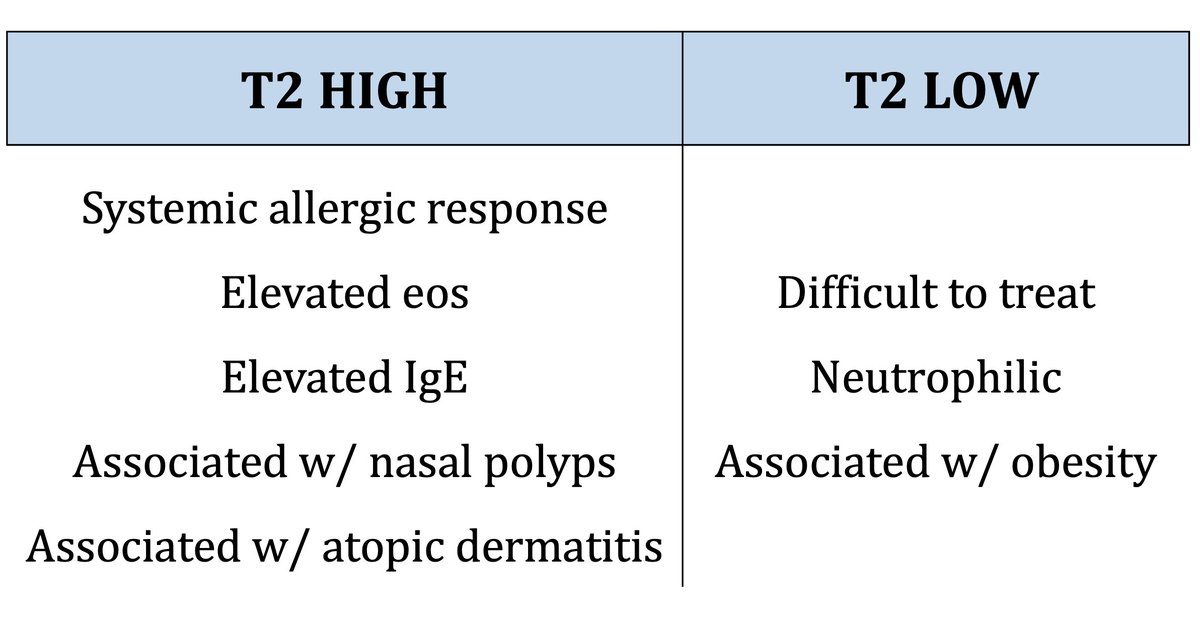
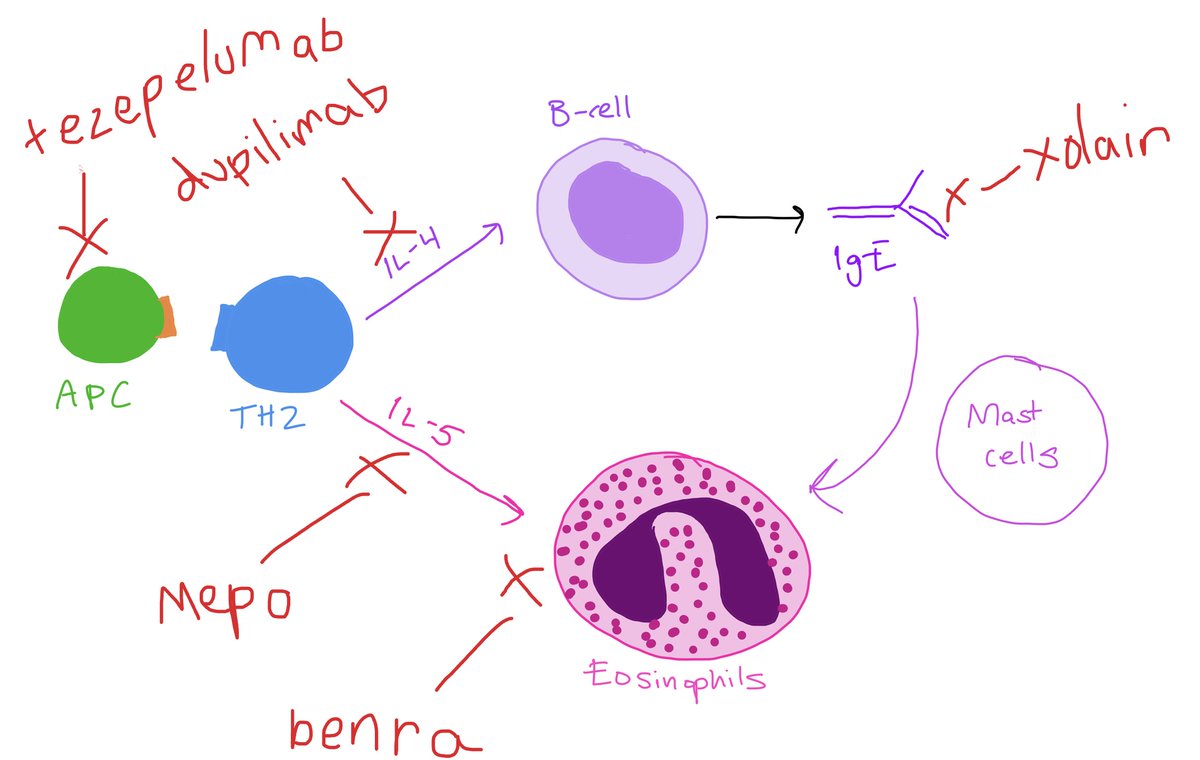
T2-high patients often have targets for biologics. These meds can be really life changing for severe asthma and allergy patients, and I’m happy to see them being used earlier and earlier.
Asthma can be tricky to diagnose and tricky to manage, but if you are attentive and thorough (and you make sure they’re on an ICS) you can make a big difference in quality of life for your asthma patients (26 million in the US)!
Loading suggestions...