

🔥 Let’s discuss about Chronic Kidney Disease - Mineral Bone disease (CKD- MBD)
🔥 This is what I thought it was as a student… I was wrong ❌
🔥Did you also think so ? #NephTwitter #MedTwitter #Medpearls
🔥 This is what I thought it was as a student… I was wrong ❌
🔥Did you also think so ? #NephTwitter #MedTwitter #Medpearls
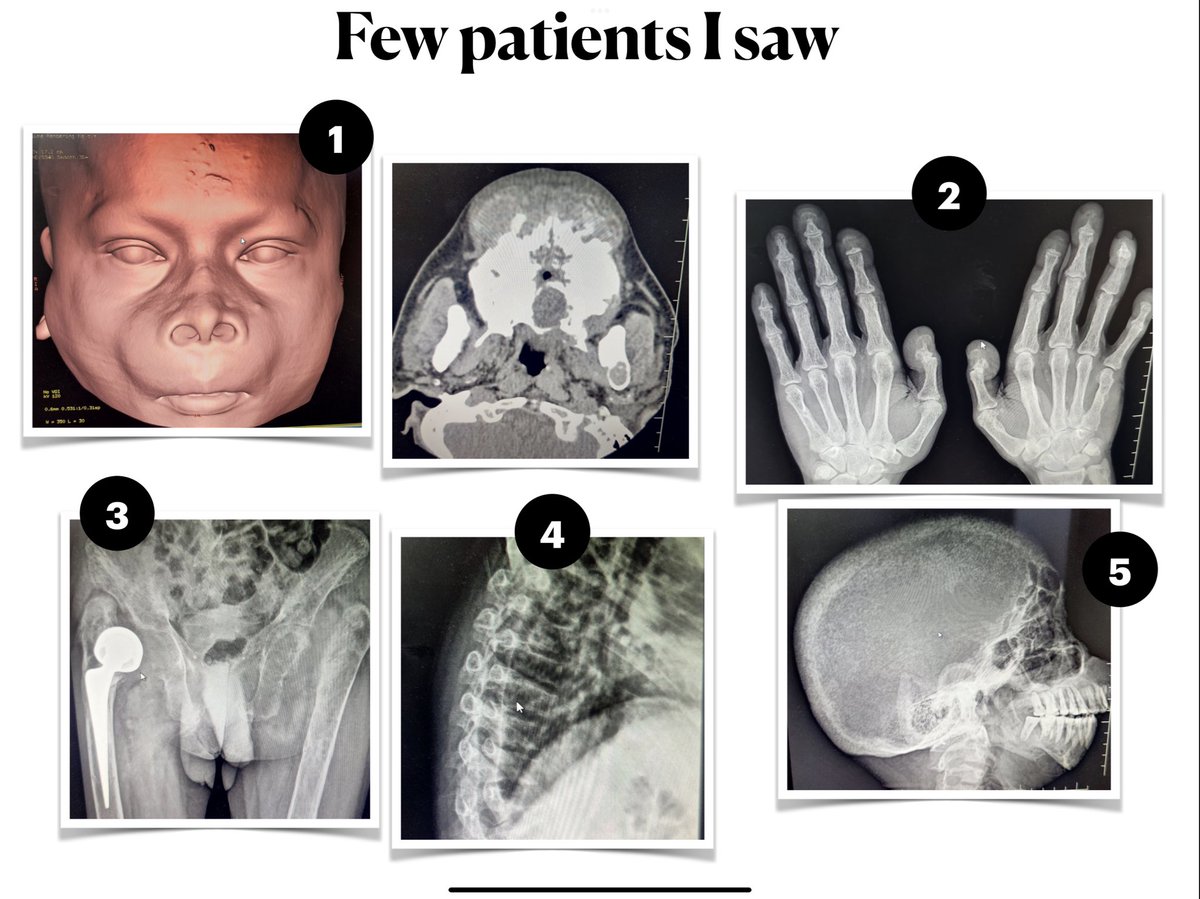
🔥 I saw the following CT and X rays and that changed my view
🔥 Can you identify the following X-rays and CT
🥇 the award winning question . What’s figure no. 1
🔥 Can you identify the following X-rays and CT
🥇 the award winning question . What’s figure no. 1
🔥 I realised this is a big game ⛳️ contrary to what I thought 🧠
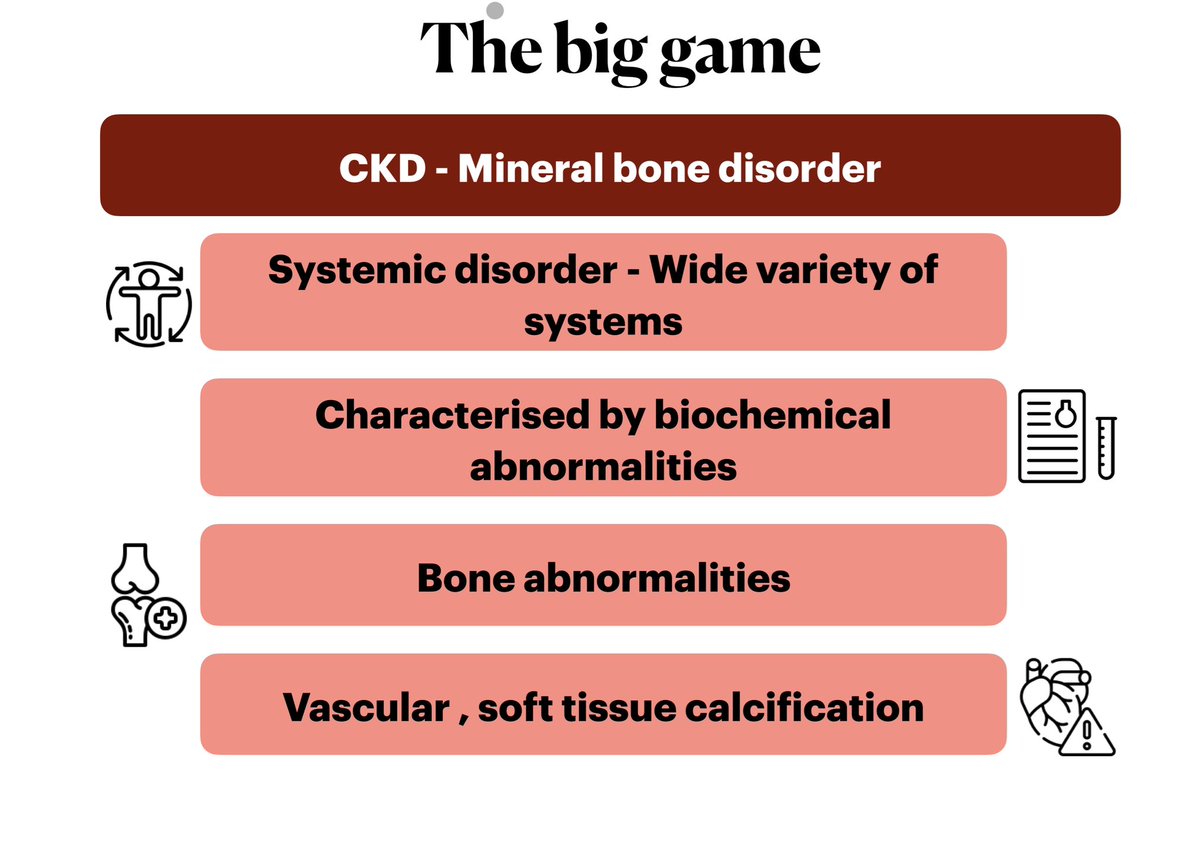

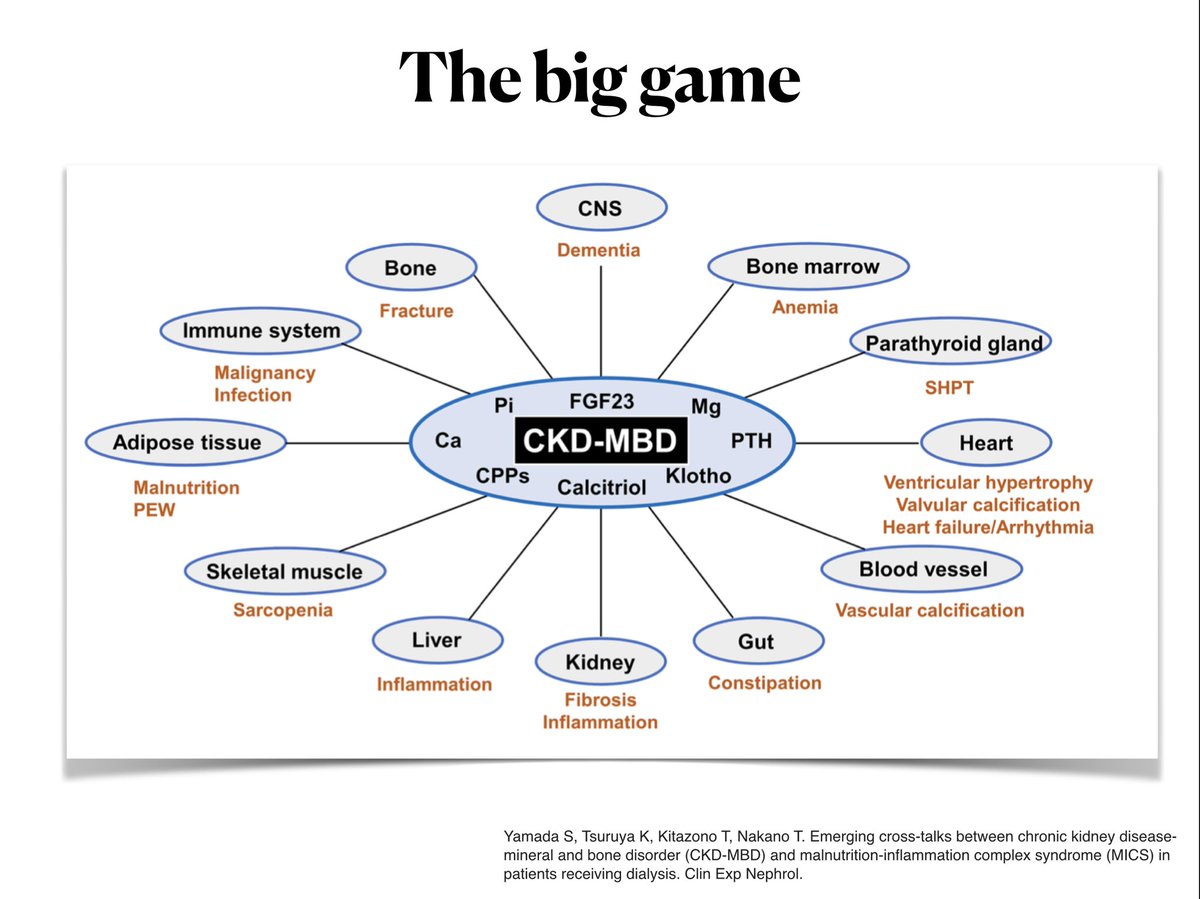
CKD MBD has far reaching effects 🌪️🌪️
🧠:CNS
🦴:Bone
❤️: Heart
🩸: Blood and vessels
🫘: Kidneys
💪: Muscle
What doesn’t it effect ? It does effects all 🔴
🧠:CNS
🦴:Bone
❤️: Heart
🩸: Blood and vessels
🫘: Kidneys
💪: Muscle
What doesn’t it effect ? It does effects all 🔴
🔥 The star players of the the Big game
🔥 Few players whom we still don’t know and yet to be named
🔥 Few players whom we still don’t know and yet to be named
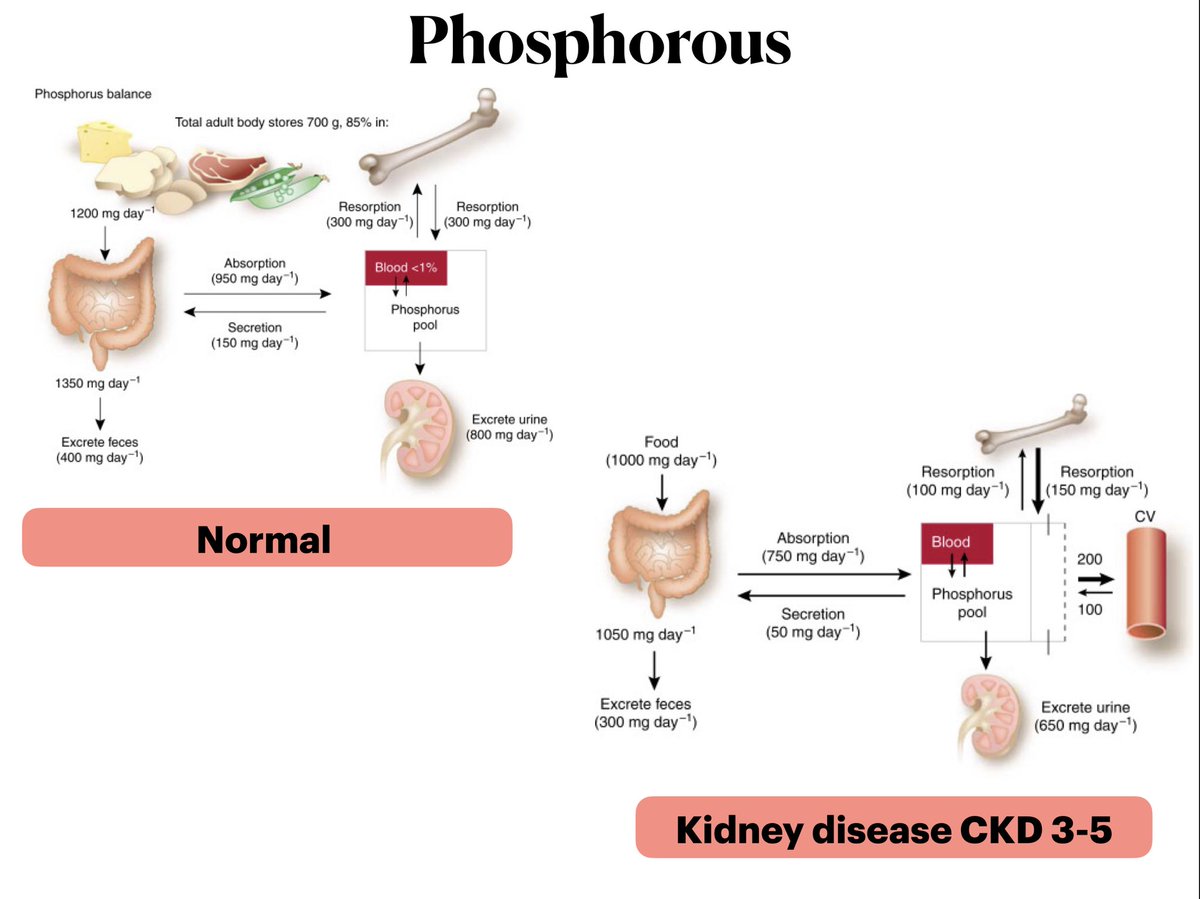
🔥Kidney : 🫘 key regulator of phosphate in health
🔥What happens to the phosphate in CKD ?
🔥Filtered load decreases ➡️ positive phosphorous balance
🔥 Increase in phophorous ➡️ Body’s mechanisms to normalise it starts 🏎️
🔥What happens to the phosphate in CKD ?
🔥Filtered load decreases ➡️ positive phosphorous balance
🔥 Increase in phophorous ➡️ Body’s mechanisms to normalise it starts 🏎️
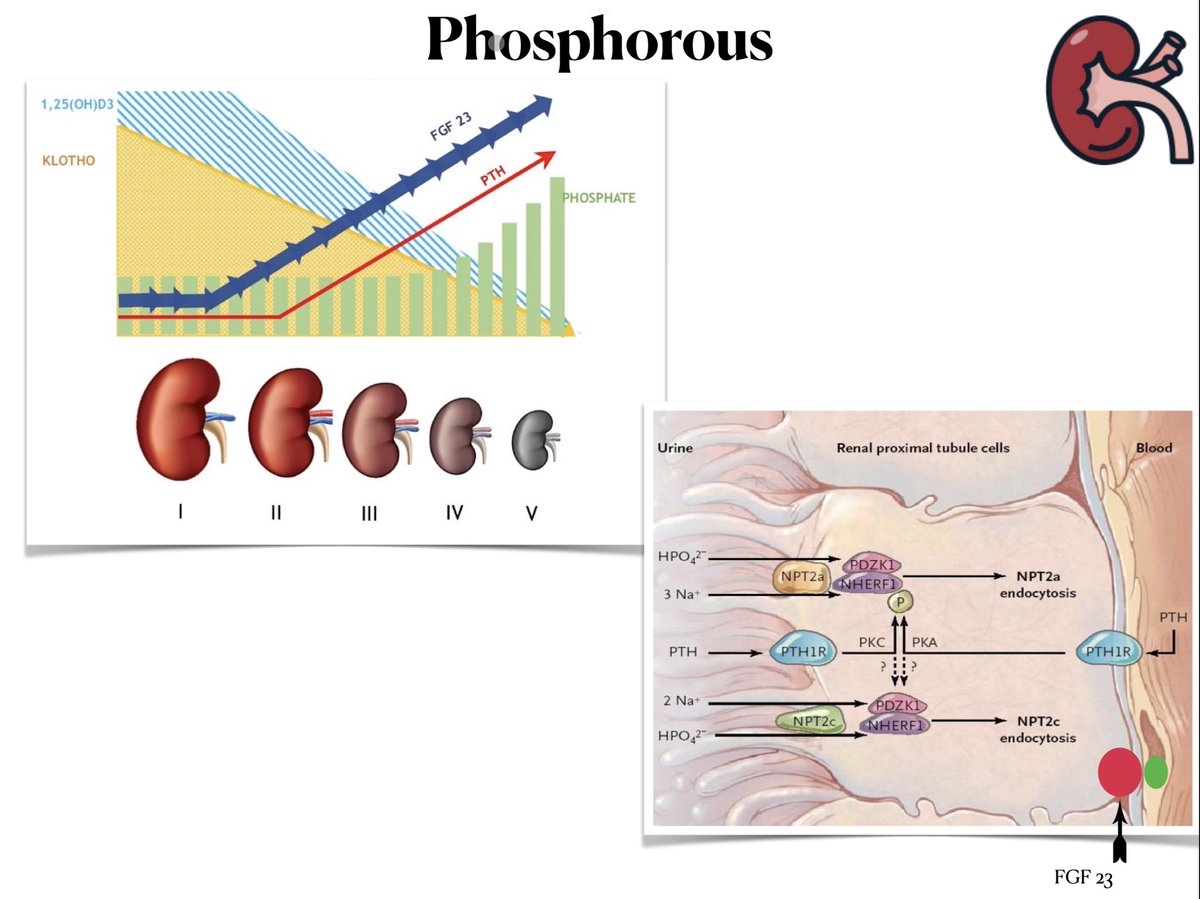
🔥 Mechanisms of decreasing phosphate
⏫ increase in PTH ➡️ 🔻🔻 decreases phosphate
⏫ PTH ➡️ 🔻🔻 sodium phosphate transporter in tubules ➡️ Phosphaturia
⏫ FGF 23 ➡️ Phosphaturia
🚨🚨 By the time you see an abnormal phosphate ➡️ all compensations surpassed
⏫ increase in PTH ➡️ 🔻🔻 decreases phosphate
⏫ PTH ➡️ 🔻🔻 sodium phosphate transporter in tubules ➡️ Phosphaturia
⏫ FGF 23 ➡️ Phosphaturia
🚨🚨 By the time you see an abnormal phosphate ➡️ all compensations surpassed
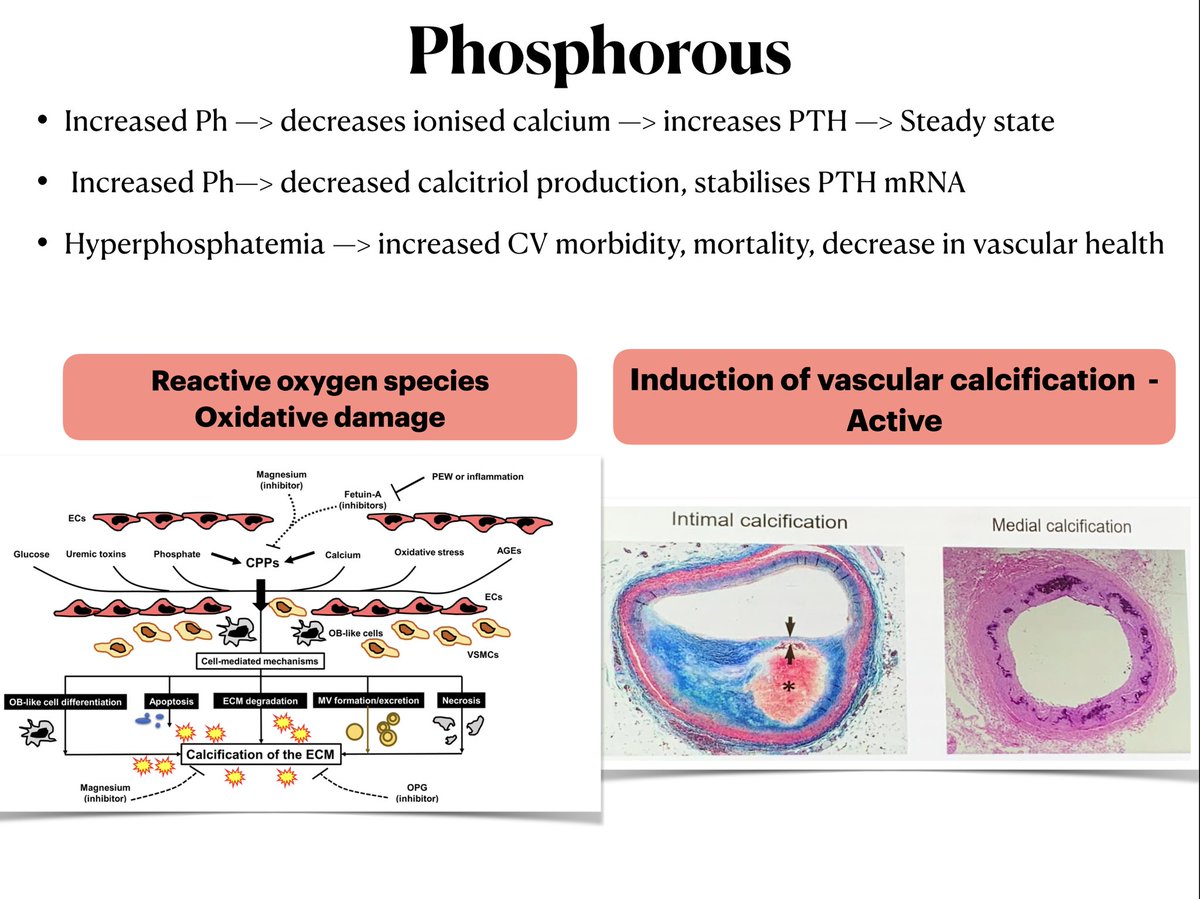
🔥⏫ Phosphates ➡️ 🔻🔻 calcium ➡️ 🔺🔺 PTH
🔥⏫ Phosphates ➡️ 🔻🔻 calcitriol and stabilises PTH mRNA
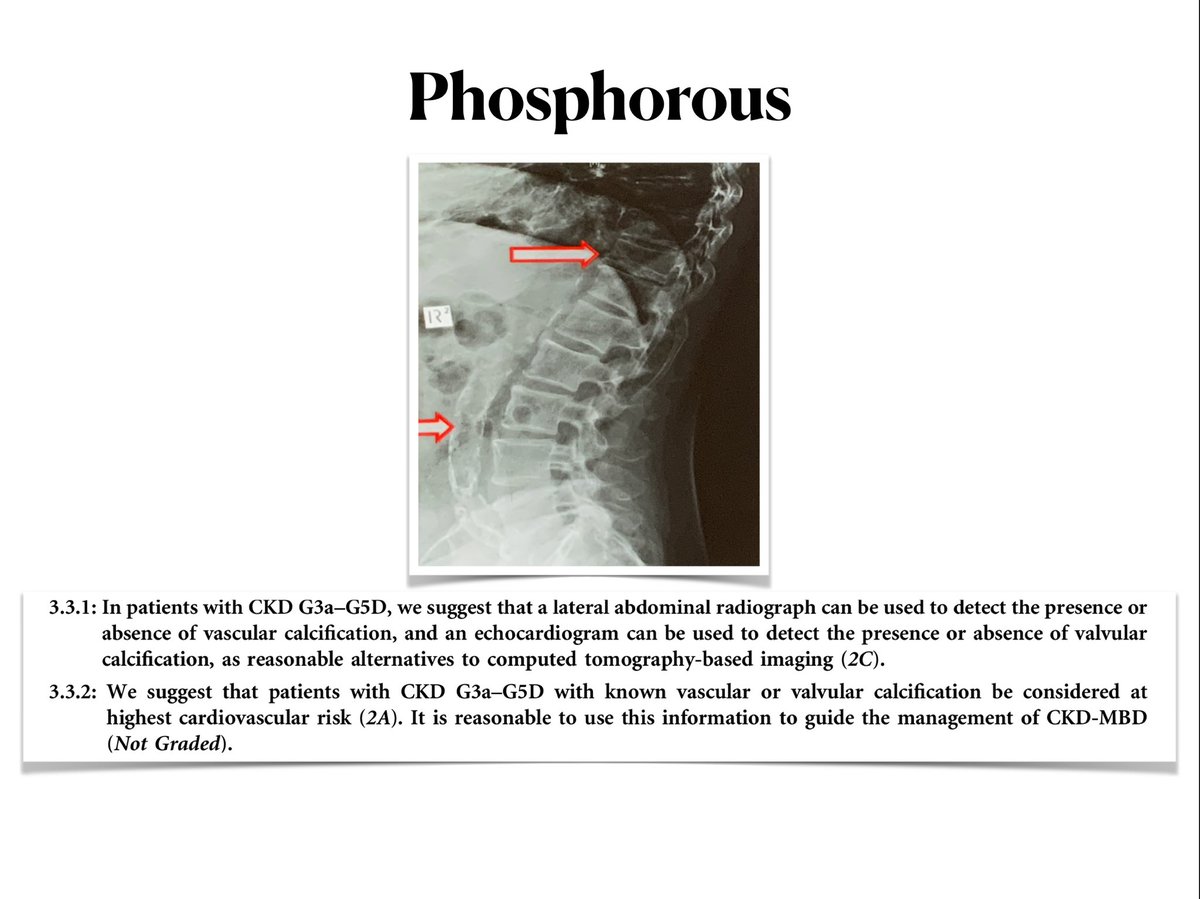
🔥⏫ phosphate level cause vascular calcification
🔥KDIGO suggest to do X ray for vascular and ECHO for valvular calcification
🔥⏫ Phosphates ➡️ 🔻🔻 calcitriol and stabilises PTH mRNA
🔥⏫ phosphate level cause vascular calcification
🔥KDIGO suggest to do X ray for vascular and ECHO for valvular calcification
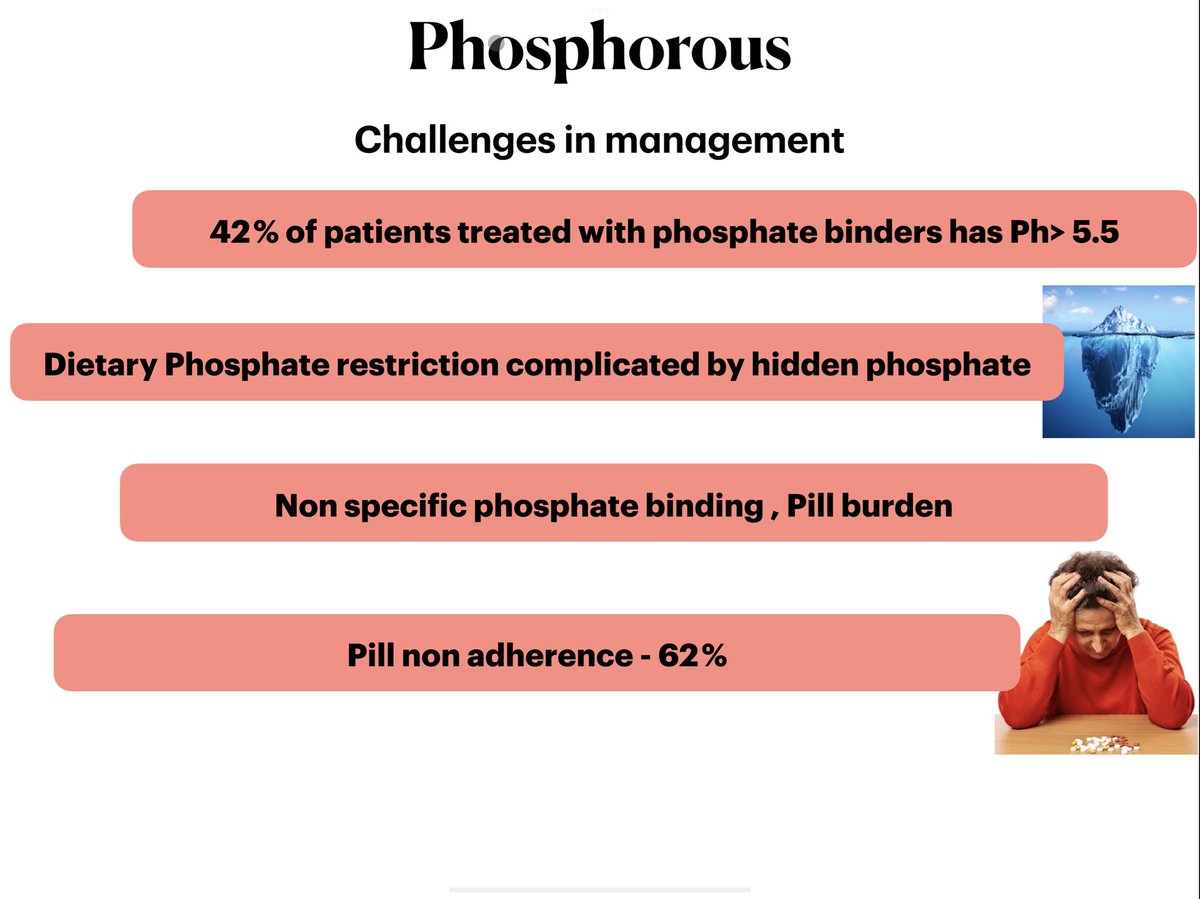
🔥 Challenges in phosphate management
🔥Most patients are not in the range inspite of best efforts
🔥Most patients are not in the range inspite of best efforts
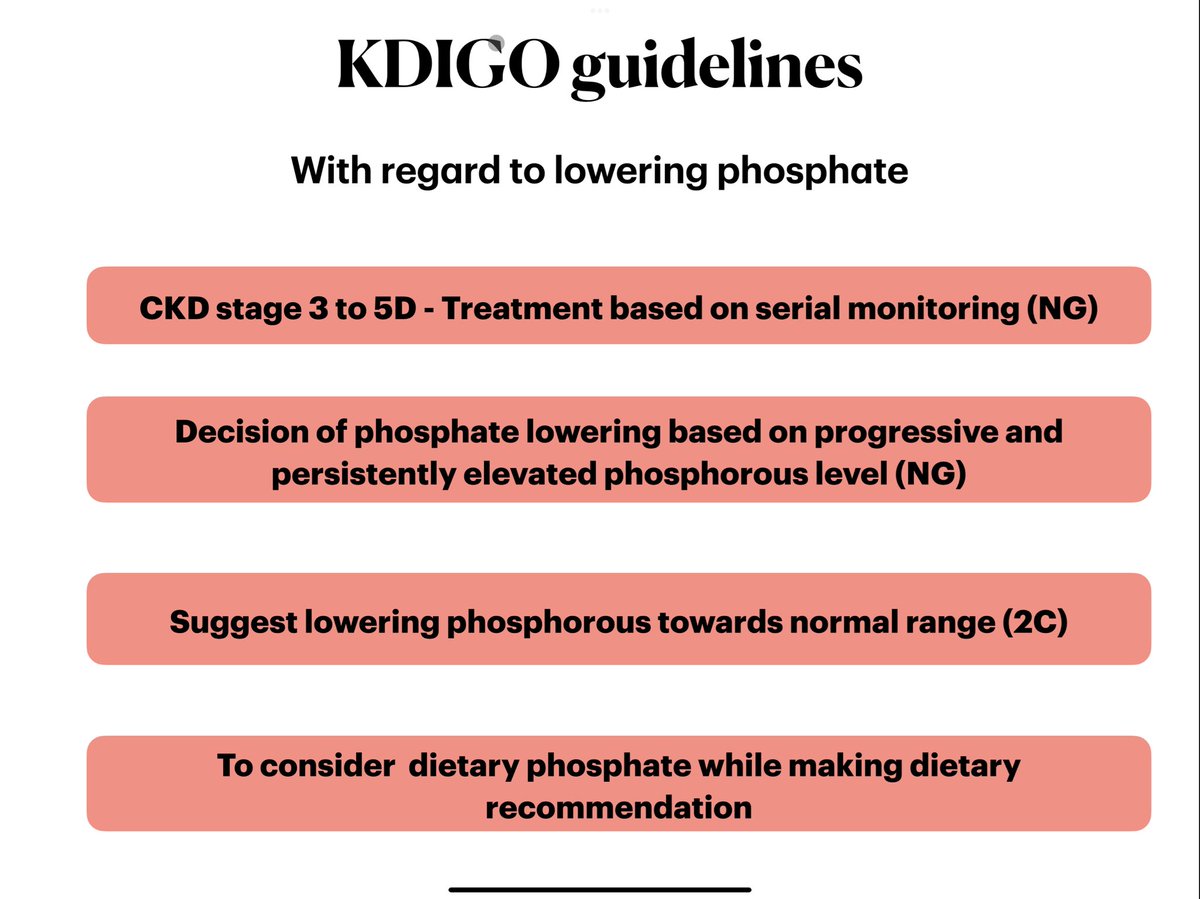
🔥 what does KDIGO tell about Phosphate lowering therapy ?
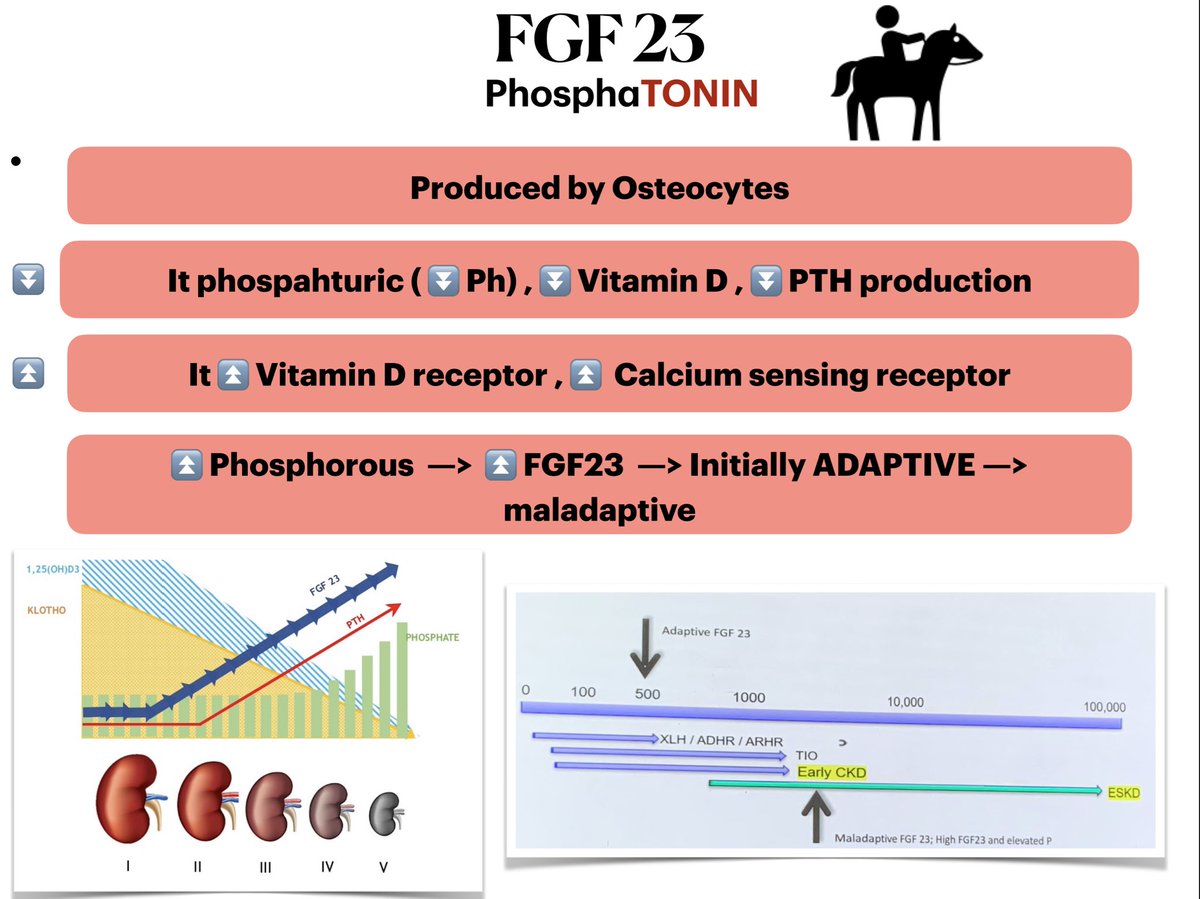
🔥 FGF23 - Remember FGF23 is like a TONIN( remember it like the reins of a horse 🎠 )
🔥Brings down Vitamin D , PTH , Phosphorous
🔥Brings down Vitamin D , PTH , Phosphorous
🔥 Klotho - the supporting player
🔥 Decrease in Klotho is the first change in CKD -MBD
🥇
🔥 Converts FGF receptor into a high affinity one 👩❤️💋👨
🔥 Decrease in Klotho is the first change in CKD -MBD
🥇
🔥 Converts FGF receptor into a high affinity one 👩❤️💋👨
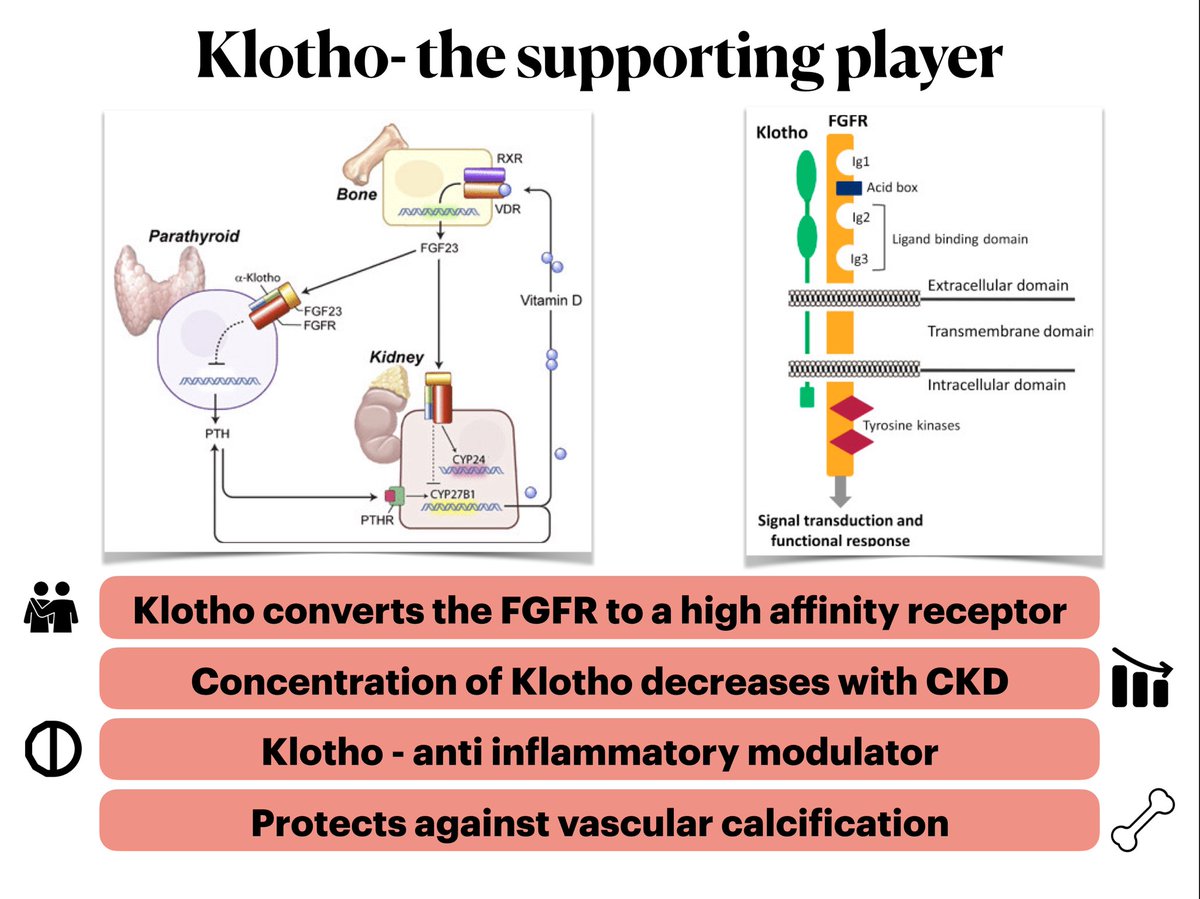
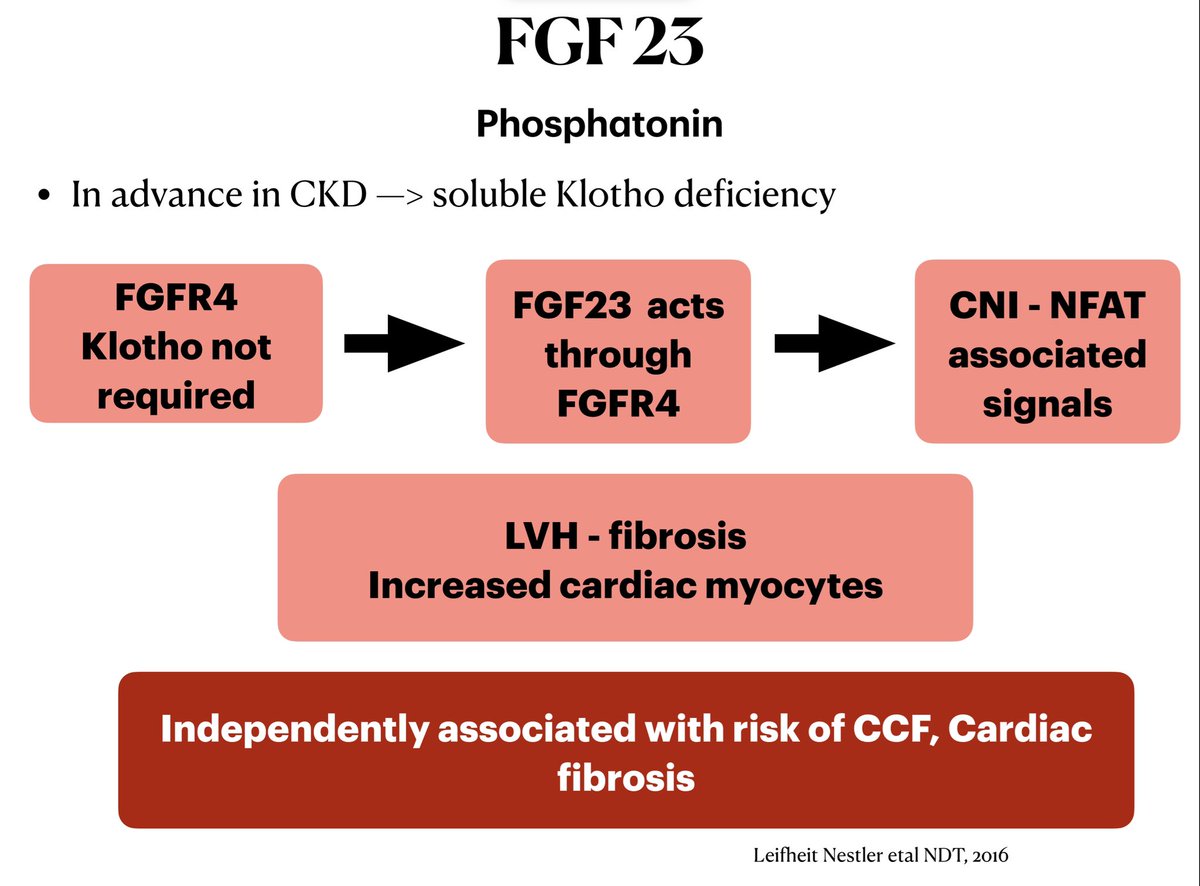
🔥Does all FGF23 receptors require Klotho ?
🔥One of the postulated mechanism of cardiac fibrosis in CKD
🔥One of the postulated mechanism of cardiac fibrosis in CKD
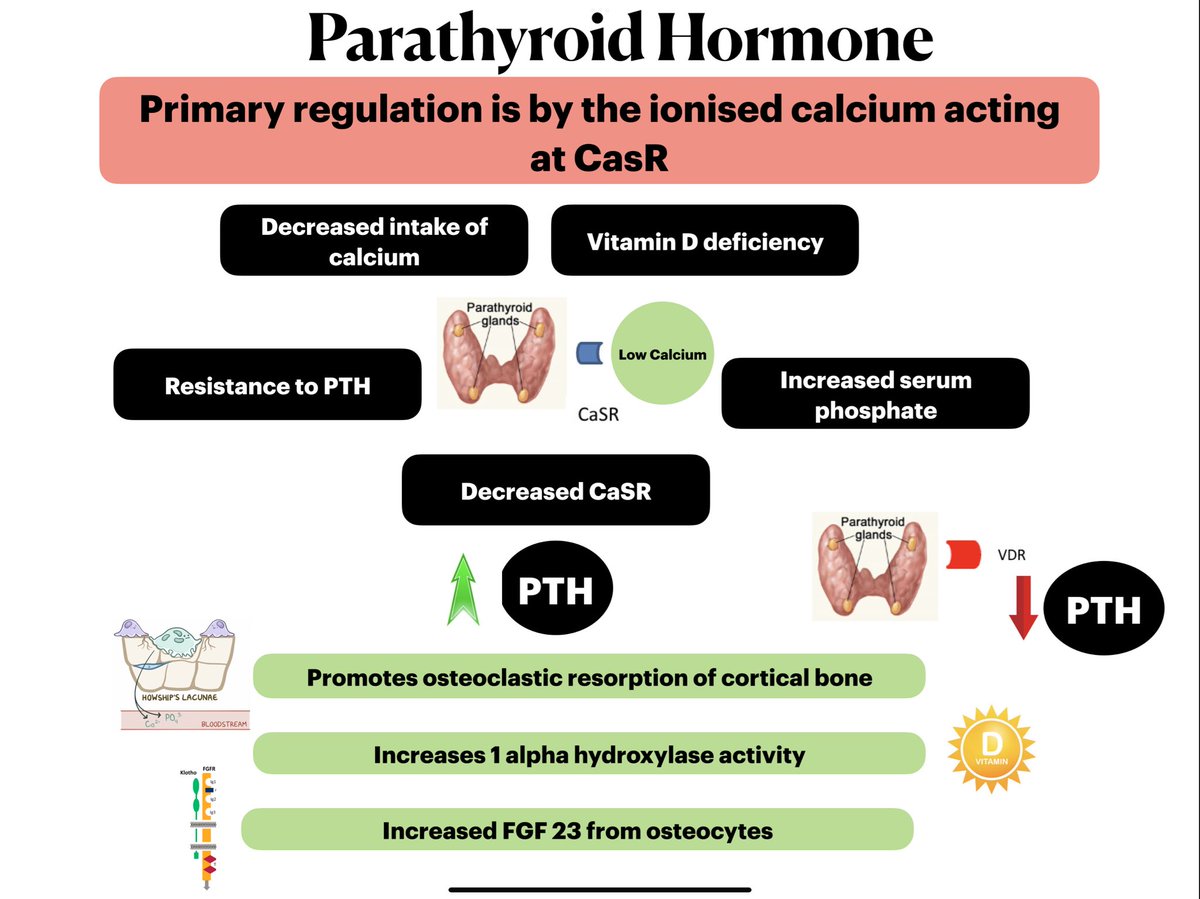
🔥 Parathyroid hormone : primary regulated by ionised calcium at the CaSR
🔥⏬ calcium at CaSR ➡️ tells the parathyroid gland to ⏫ PTH
🔥Parathyroid gland also has Vitamin D receptor which when activated cause ⏬ PTH
🔥⏬ calcium at CaSR ➡️ tells the parathyroid gland to ⏫ PTH
🔥Parathyroid gland also has Vitamin D receptor which when activated cause ⏬ PTH
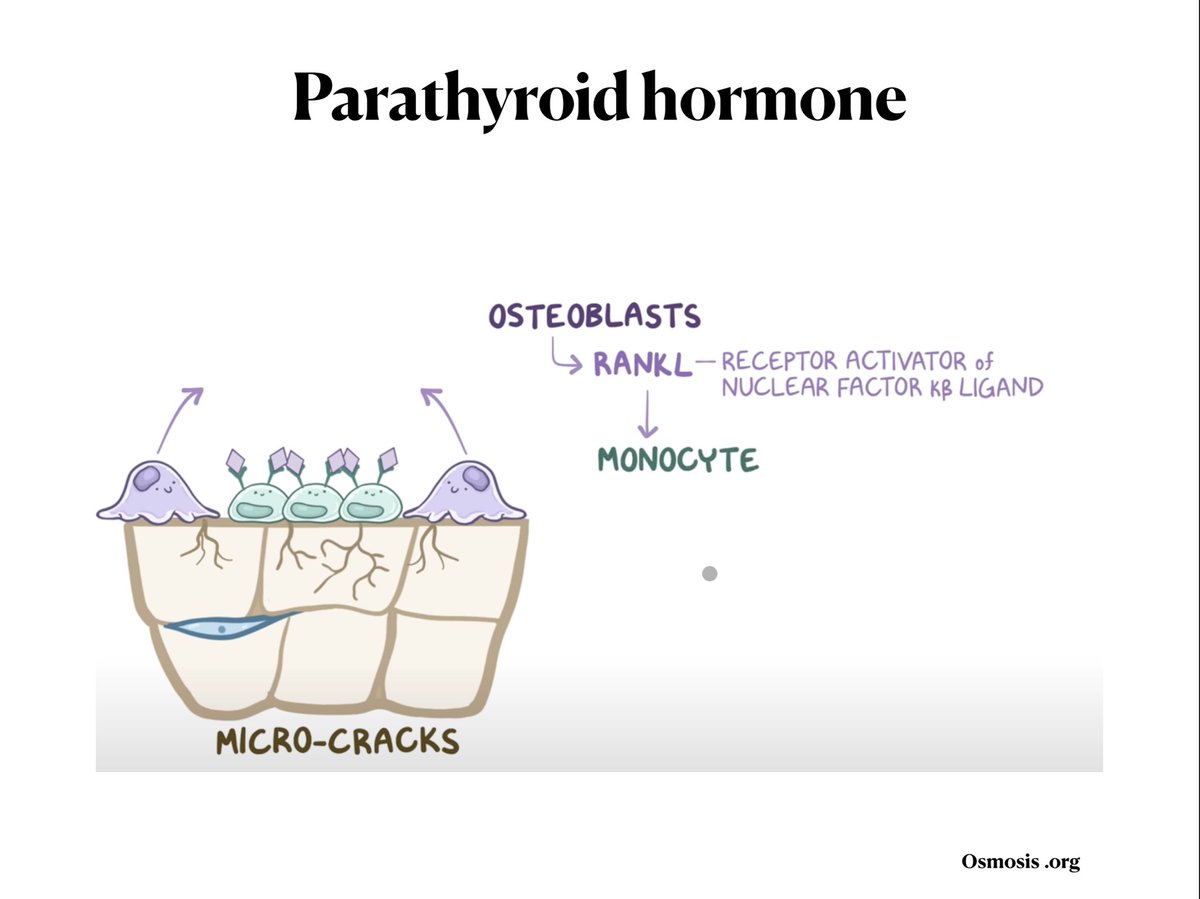
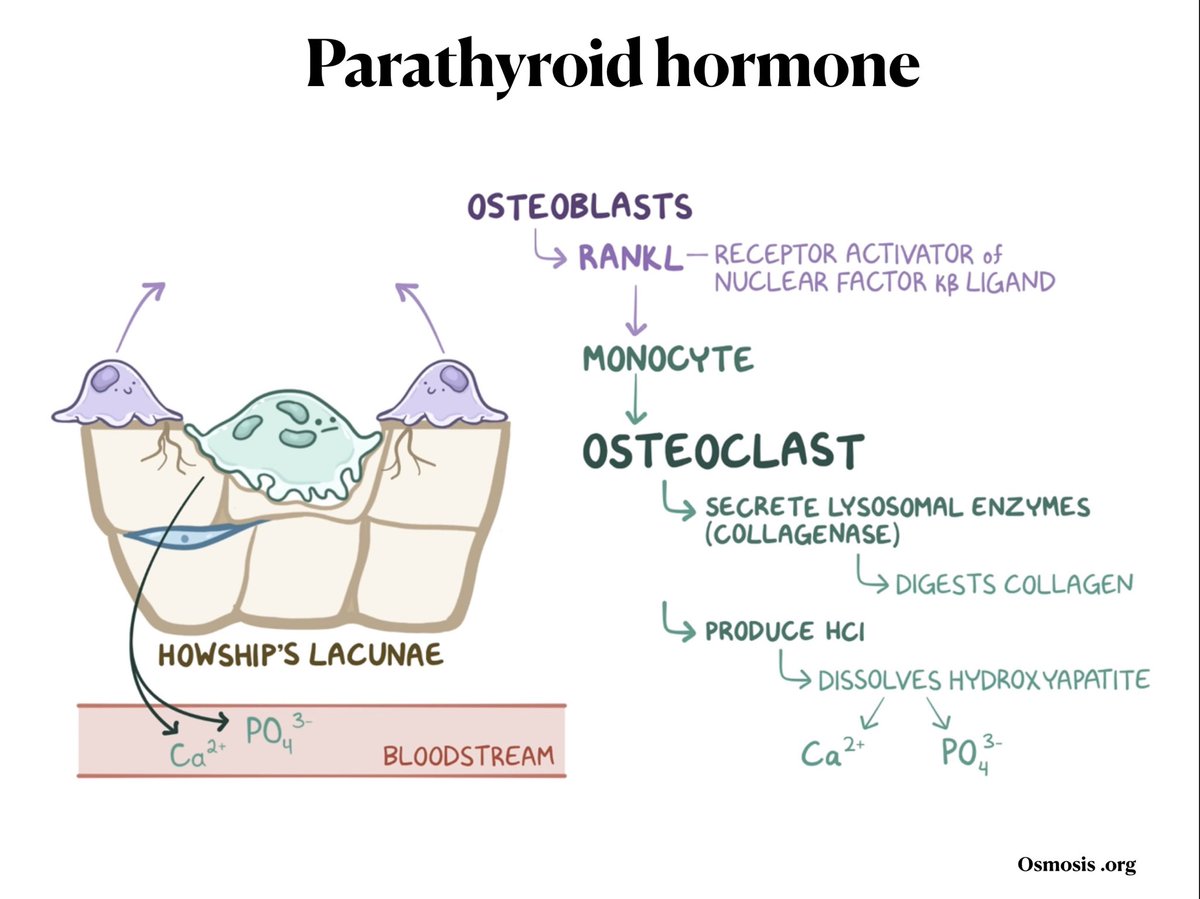
🔥 PTH ⏫ the RANK receptors on osteoblasts
🔥 RANK receptors activated by RANKL Osteoclasts are formed
🔥 Osteoclasts ➡️ ⏫ calcium and phosphorous in blood
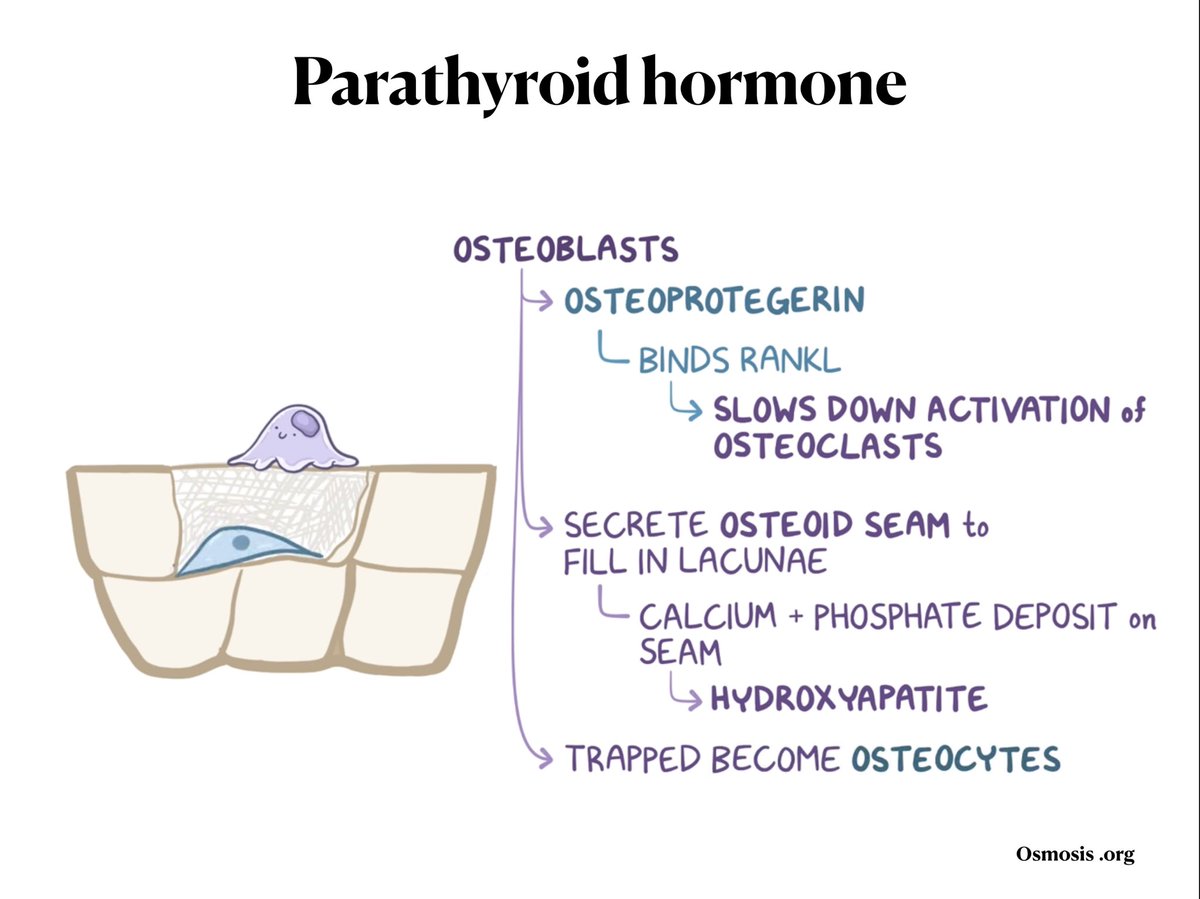
🔥Osteoblasts secrete osteoprotegerin and ➡️ binds RANK L and slows Osteoclasts
Pics from osmosis.org
🔥 RANK receptors activated by RANKL Osteoclasts are formed
🔥 Osteoclasts ➡️ ⏫ calcium and phosphorous in blood
🔥Osteoblasts secrete osteoprotegerin and ➡️ binds RANK L and slows Osteoclasts
Pics from osmosis.org

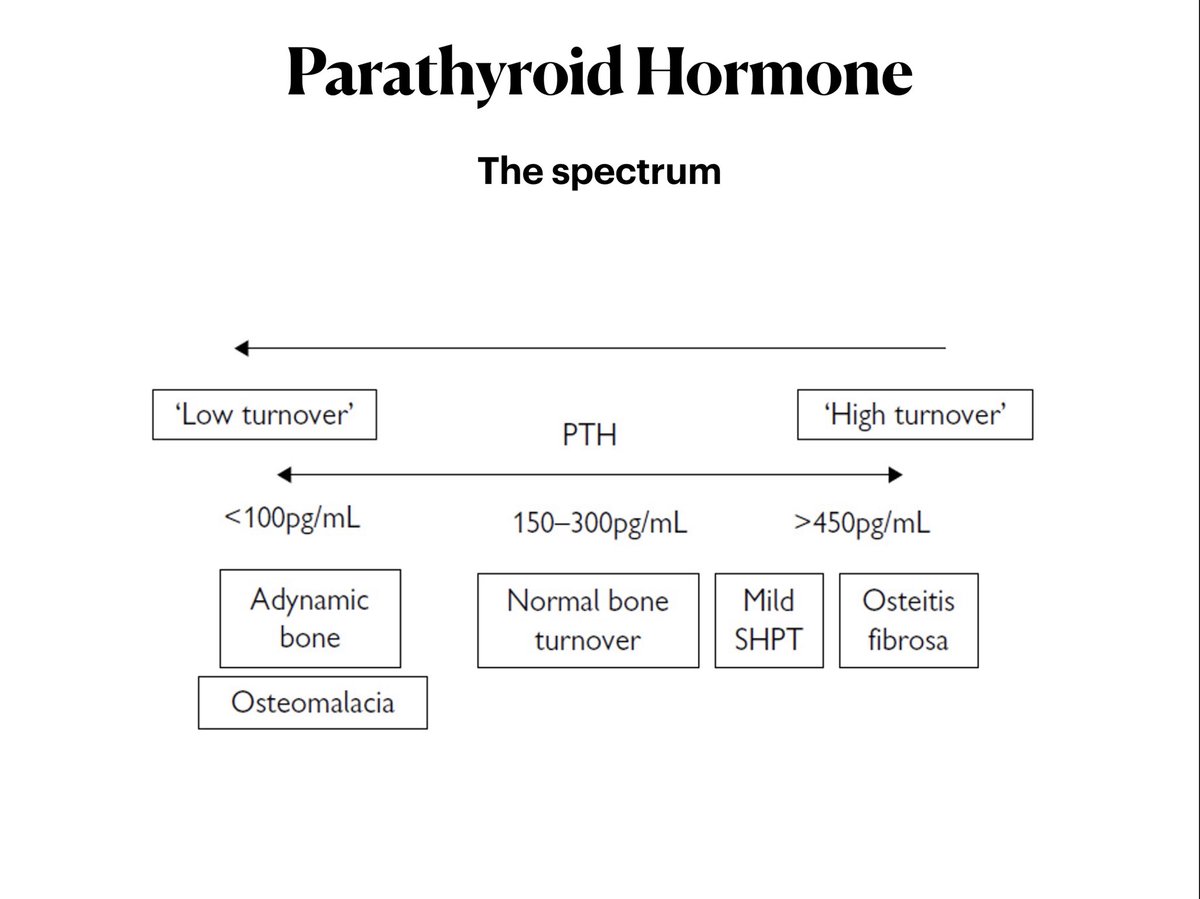
🔥 The spectrum of parathyroid abnormalities
🔥we are seeing more of low turn over disease now a days
🔥 ⏫⏫ High turn over bone ➡️ weak bones due to demineralisation
🔥⏬⏬ low turn over ➡️ no dynamicity ➡️ bones are brittle and ( easy to break )
🔥we are seeing more of low turn over disease now a days
🔥 ⏫⏫ High turn over bone ➡️ weak bones due to demineralisation
🔥⏬⏬ low turn over ➡️ no dynamicity ➡️ bones are brittle and ( easy to break )
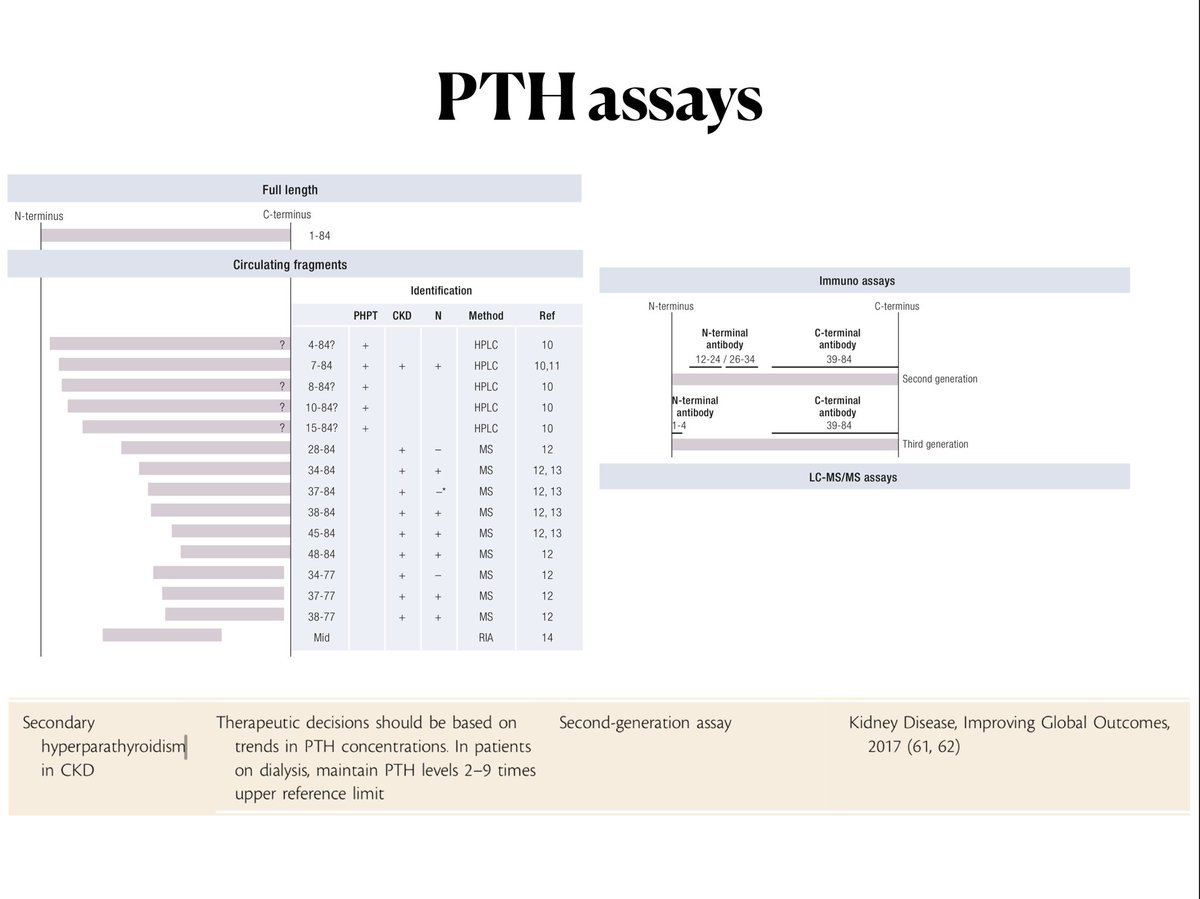
🔥 How do you check PTH levels ?
🔥 PTH - 84 amino acids
🔥 Assays may pick up the whole molecule 🌝or fragments 🌓
🔥Assays - designed to pick up the whole molecule instead of fragments by its modification - Subsequent generation of assays getting better at it.
🔥 PTH - 84 amino acids
🔥 Assays may pick up the whole molecule 🌝or fragments 🌓
🔥Assays - designed to pick up the whole molecule instead of fragments by its modification - Subsequent generation of assays getting better at it.
🔥 Busy slide : But important 🥇
🔥 🧐Evaluate for low calcium, Low vitamin D, Increased phosphate(ALL WHICH CAN INCREASE PTH ) - TRY CORRECTING IT before jumping to PTH
🔥 Treat based on a trend 📈 than a single value
🔥 🧐Evaluate for low calcium, Low vitamin D, Increased phosphate(ALL WHICH CAN INCREASE PTH ) - TRY CORRECTING IT before jumping to PTH
🔥 Treat based on a trend 📈 than a single value
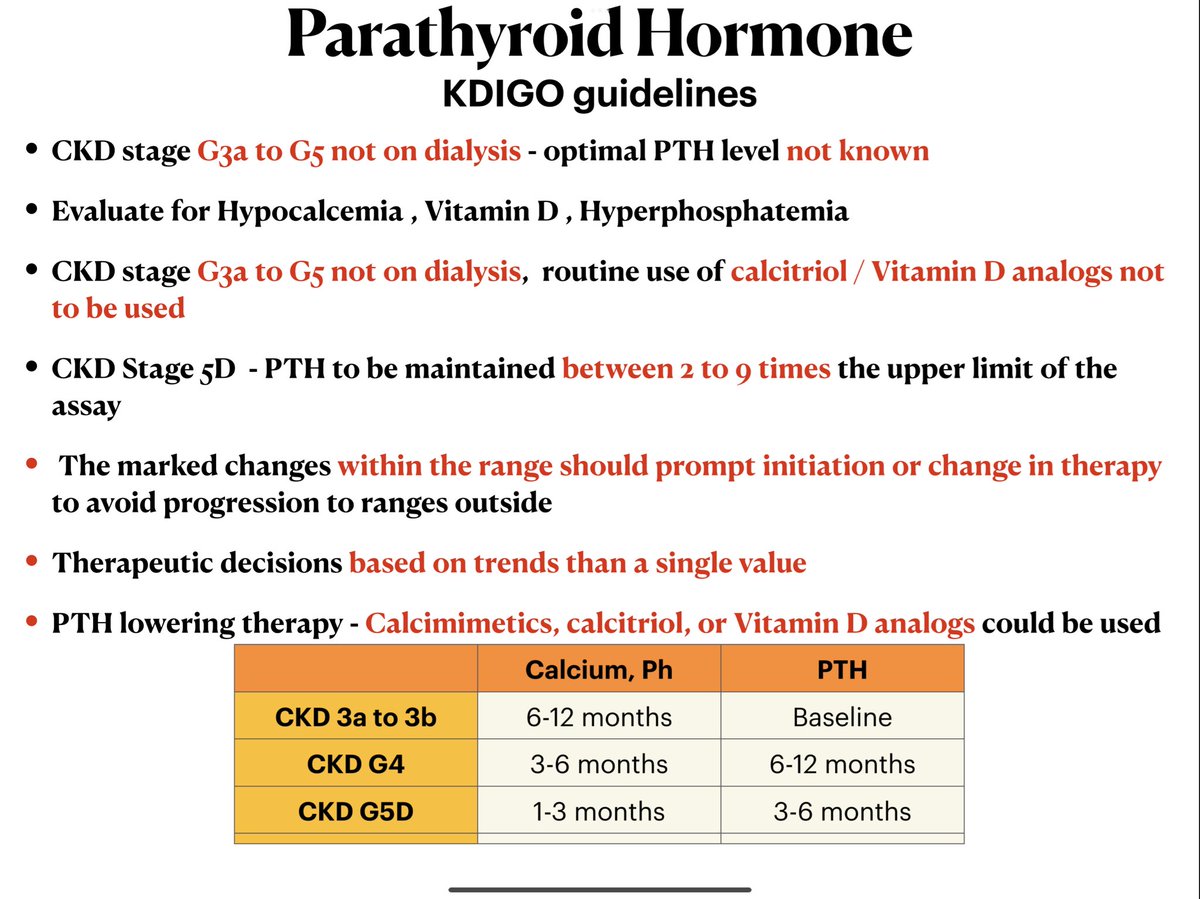
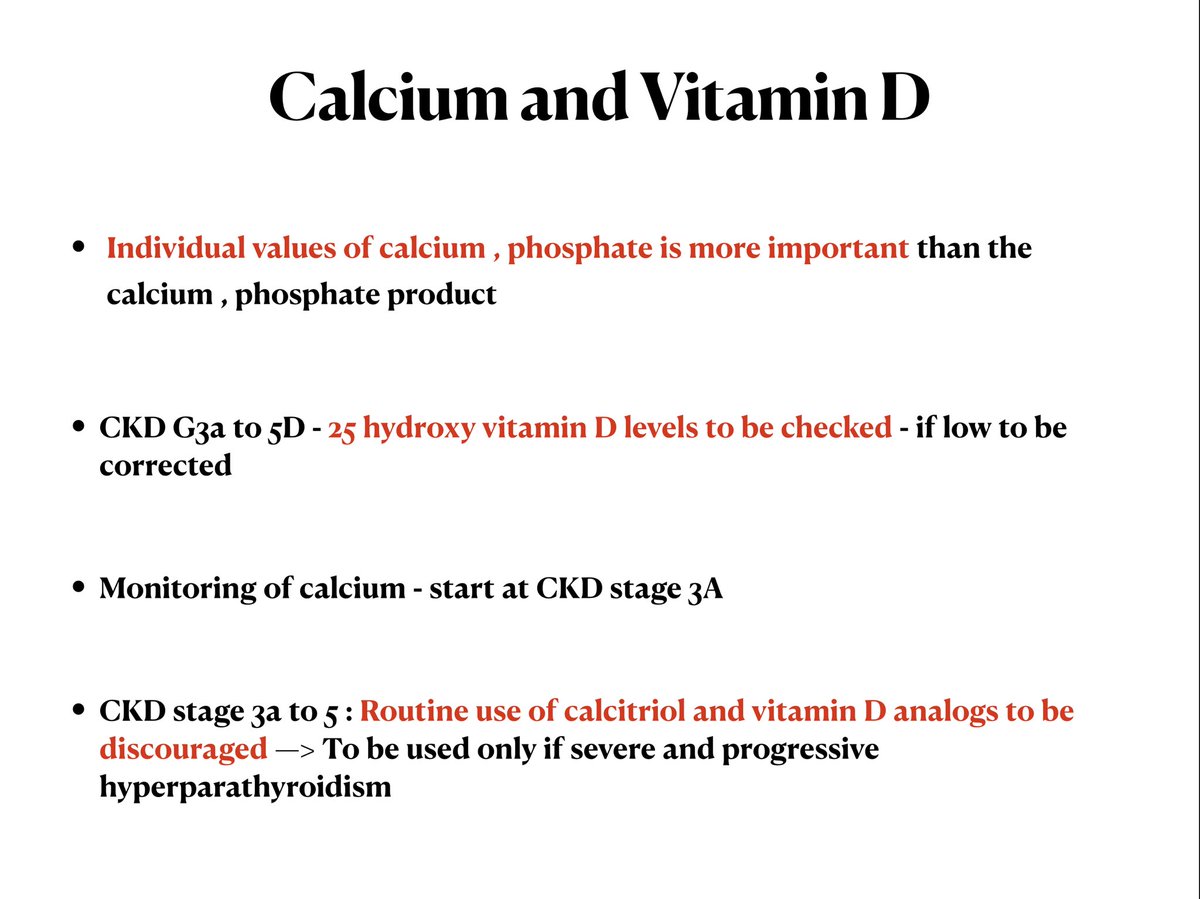
🔥What about calcium and Vitamin D?
🚨🚨 Routine use of calcitriol and Vitamin D analogues to be discouraged in CKD stage 3A to 5
🚨🚨 Routine use of calcitriol and Vitamin D analogues to be discouraged in CKD stage 3A to 5
🔥 The diagnosis of our patient was Leontiasis Ossea (like a lion)
🔥 Rare presentation of severe hyperparathyroidism
🔥affects craniofacial bones
🔥D/D - Paget’s disease , fibrous dysplasia , ossifying and non ossifying tumours
🔥 Rare presentation of severe hyperparathyroidism
🔥affects craniofacial bones
🔥D/D - Paget’s disease , fibrous dysplasia , ossifying and non ossifying tumours

🔥will cover osteoporosis, DEXA scan and bone biopsy in the next tweetorial
Loading suggestions...