

Here are some fallacies that I can see the usual suspects putting out on Long COVID
-"Most people recover from LC"
-"Most LC occurs in those hospitalised"
-"Vaccination has massively reduced the burden"
Thread addressing these:
-"Most people recover from LC"
-"Most LC occurs in those hospitalised"
-"Vaccination has massively reduced the burden"
Thread addressing these:
"Most people recover from LC"
Here's a study of patients recruited from an LC clinic where only 7.6% recovered over a 2 yr period, and their median duration of recovery was 1 year (not a quick recovery at all!)
thelancet.com
Here's a study of patients recruited from an LC clinic where only 7.6% recovered over a 2 yr period, and their median duration of recovery was 1 year (not a quick recovery at all!)
thelancet.com

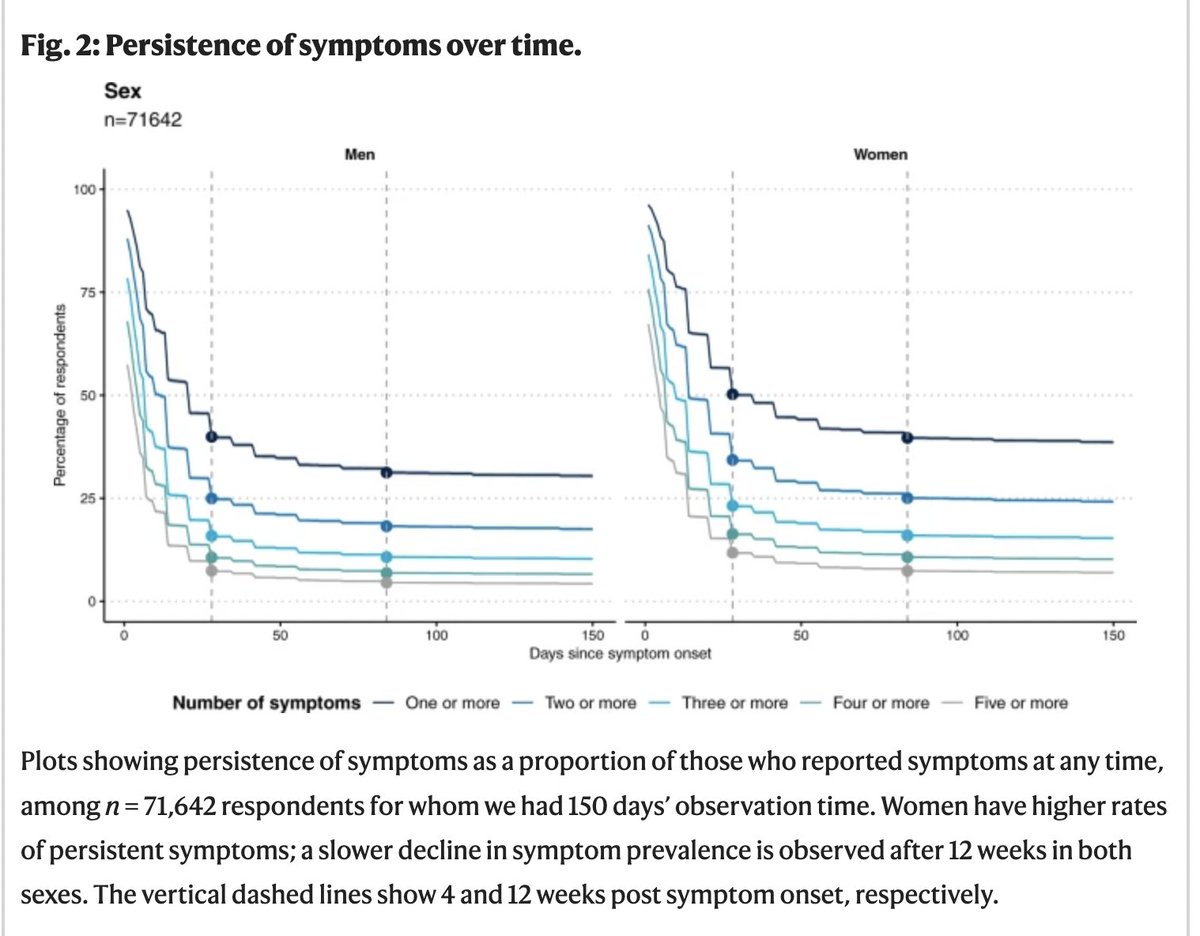
But that's a study from an outpatient clinic. What about the community? Here's the REACT study:
LC definition requires being 12 wks from infection (second dashed line)- as you can see not much recovery after this point up to 6 months at least.
nature.com
LC definition requires being 12 wks from infection (second dashed line)- as you can see not much recovery after this point up to 6 months at least.
nature.com

Another prospective cohort study showed that 85% still reported symptoms at 1 year.
ncbi.nlm.nih.gov
ncbi.nlm.nih.gov

"Most LC occurs in those hospitalised"
No. If you look at all the studies I've shown here, those who were hospitalised acutely are very much the minority- 70-80% of those with LC had not been hospitalised for acute illness.
No. If you look at all the studies I've shown here, those who were hospitalised acutely are very much the minority- 70-80% of those with LC had not been hospitalised for acute illness.
"Vaccination has massively reduced the burden"
In the pre-omicron era vaccination was shown to reduce the incidence of LC by ~50%. In the omicron era, this is expected to be less (as efficacy of vaccines is lower and waning faster) but the level of protection isn't known.
In the pre-omicron era vaccination was shown to reduce the incidence of LC by ~50%. In the omicron era, this is expected to be less (as efficacy of vaccines is lower and waning faster) but the level of protection isn't known.
I guess my question here is - what reduction from 10-20% would make this not problematic? Even if the incidence is 5%, given the mass exposure to infection, that is huge at population level.
So while the burden may have been 'substantially reduced', a substantial burden still exists. Also considering the huge numbers that have been infected since omicron and omicron subvariants took over. This is affecting millions across the world.
And we haven't even discussed post-acute-sequelae here- risk of cardiovascular disease, clotting, renal dysfunction, GI diseases, neurological disease- the limited studies on this show very little protection from long-term complications with vax.
Also, who bears this burden? Recent work shows that men are more likely to recover than women. Women are already at higher risk of LC, as are those with pre-existing conidtions. Those who are economically disadvantaged are also less likely to recover.
LC creates massive health inequities and the impact is not uniform. So when you speak about who the burden is reduced in, be cognisant of this. The burden is so huge for this disease, without a clear pathway of treatments, that the focus should be the huge numbers being affected.
And those affected in the last 4 years, many of whom have been suffering since- with no access to treatment or avenue of hope. Minimising LC really doesn't help anyone. And worsens the health inequities that exist.
LC prevalence is a combination of LC incidence (new cases occurring with infection) and recovery of prevalent LC. If recovery is slow, and infection rates are high, prevalence is going to continue to be high.
If you really want to reduce the burden of LC, the focus needs to be both prevention of new infections, and treatment of those who are suffering.
Loading suggestions...