

A🧵 on alkali therapy.
First a Question❓️
A patient of diabetic ketoacidosis presented in a stupourous state with hypotension.
ABG ➡️ pH -7, HCO3 - 9 mEq/L, K-5mmol/L.
Along with other measures a decision was made for alkali therapy with sodium bicarbonate.
#MedTwitter
First a Question❓️
A patient of diabetic ketoacidosis presented in a stupourous state with hypotension.
ABG ➡️ pH -7, HCO3 - 9 mEq/L, K-5mmol/L.
Along with other measures a decision was made for alkali therapy with sodium bicarbonate.
#MedTwitter
How to give?
A.50 mEq of NaHCO3 in 300 mL of saline over 45min with target blood levels of HCO3 to 12mEq/L & pH upto 7.2
B.Isotonic NaHCO3 drip at 100ml/hr till pH>7.35
C.IV bolus 2 mEq/kg every 5min to raise pH to 7.4
D.IV bolus 1mEq/kg every hour to raise HCO3 upto 16mEq/L
A.50 mEq of NaHCO3 in 300 mL of saline over 45min with target blood levels of HCO3 to 12mEq/L & pH upto 7.2
B.Isotonic NaHCO3 drip at 100ml/hr till pH>7.35
C.IV bolus 2 mEq/kg every 5min to raise pH to 7.4
D.IV bolus 1mEq/kg every hour to raise HCO3 upto 16mEq/L
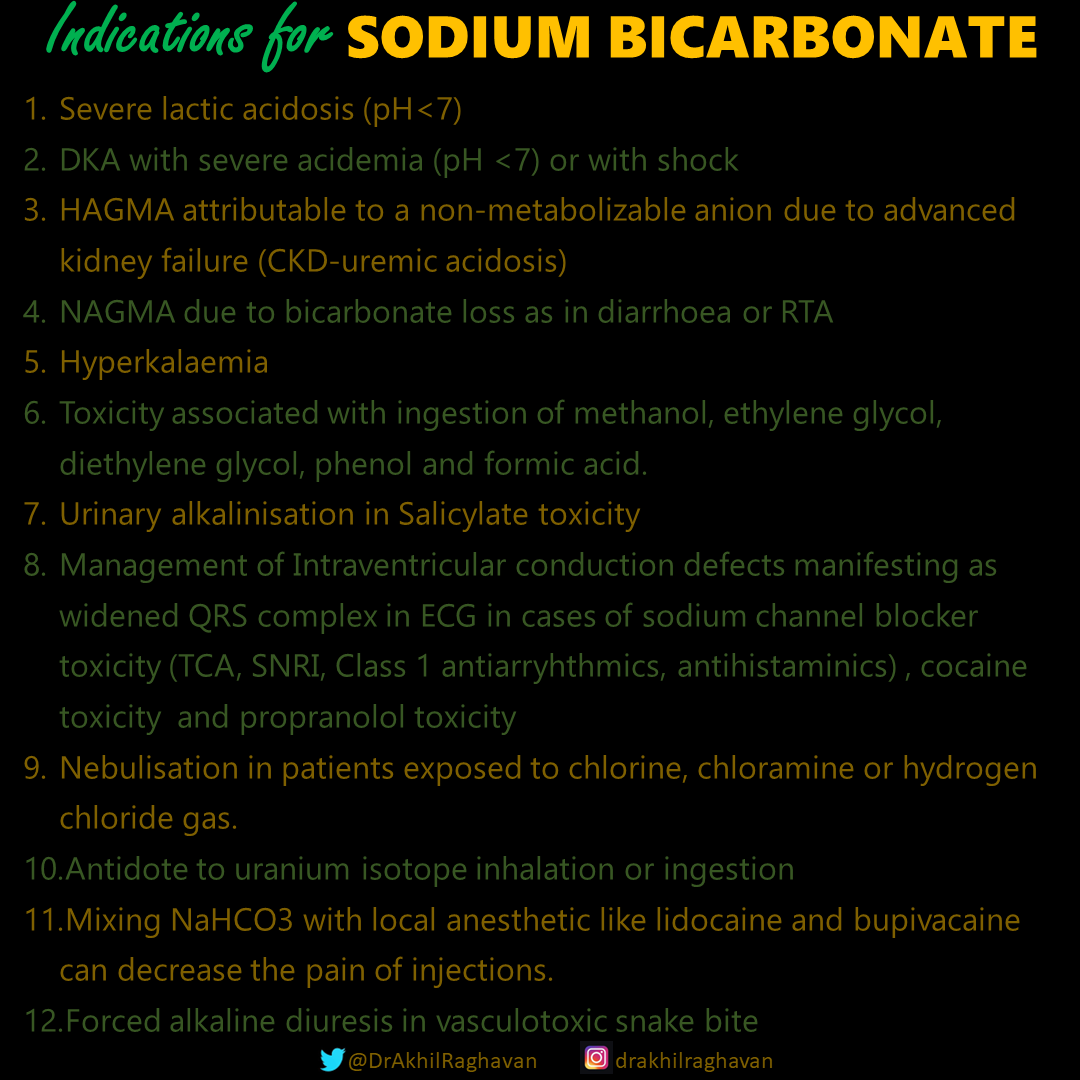
Intravenous sodium bicarbonate therapy can be lifesaving in a number of critical conditions.
Indications for sodium bicarbonate use are:
Indications for sodium bicarbonate use are:
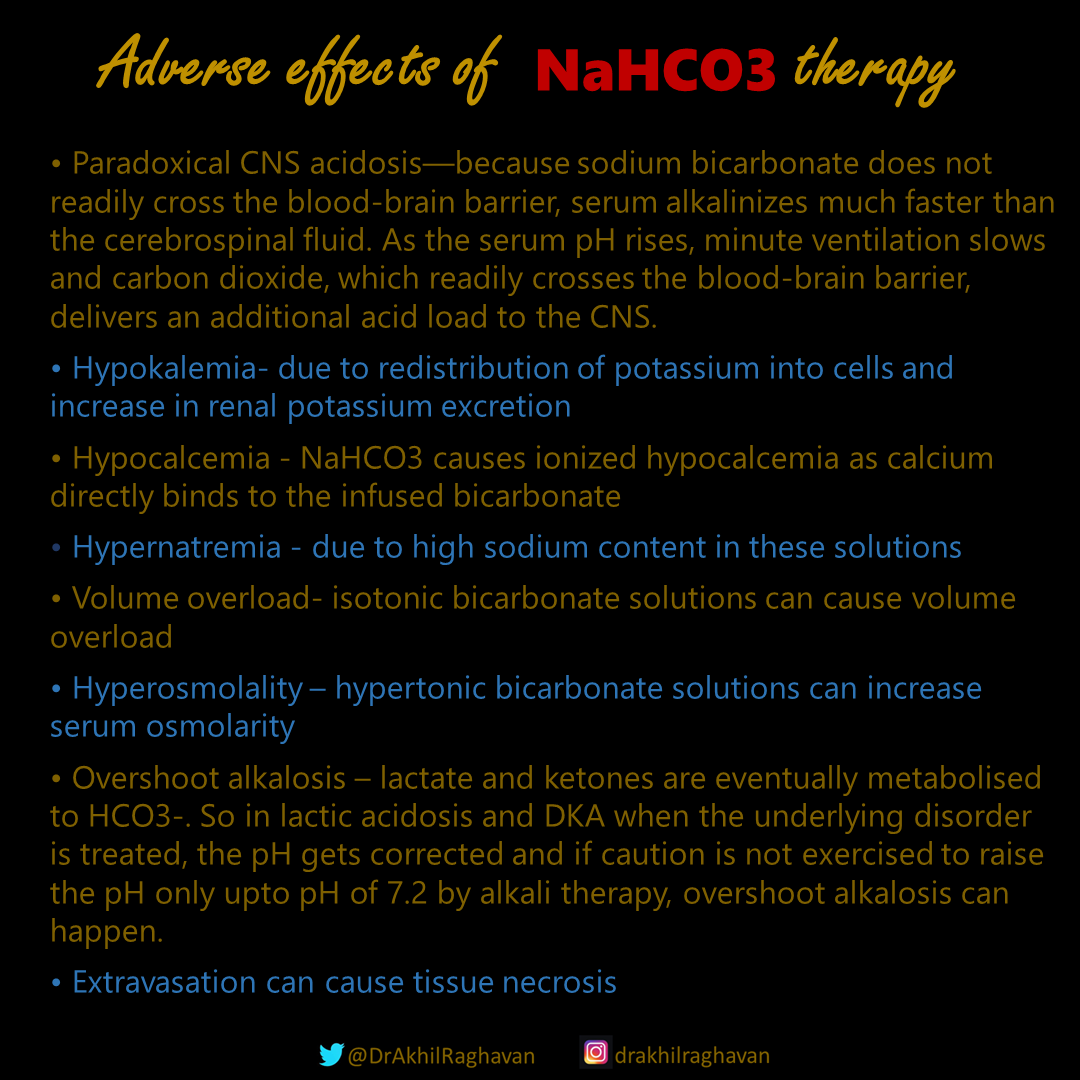
But it has to be administered in correct formulation and only if precisely indicated.
Inadvertent use can have deleterious effect.
Harmful effects of intravenous NaHCO3 are:
Inadvertent use can have deleterious effect.
Harmful effects of intravenous NaHCO3 are:
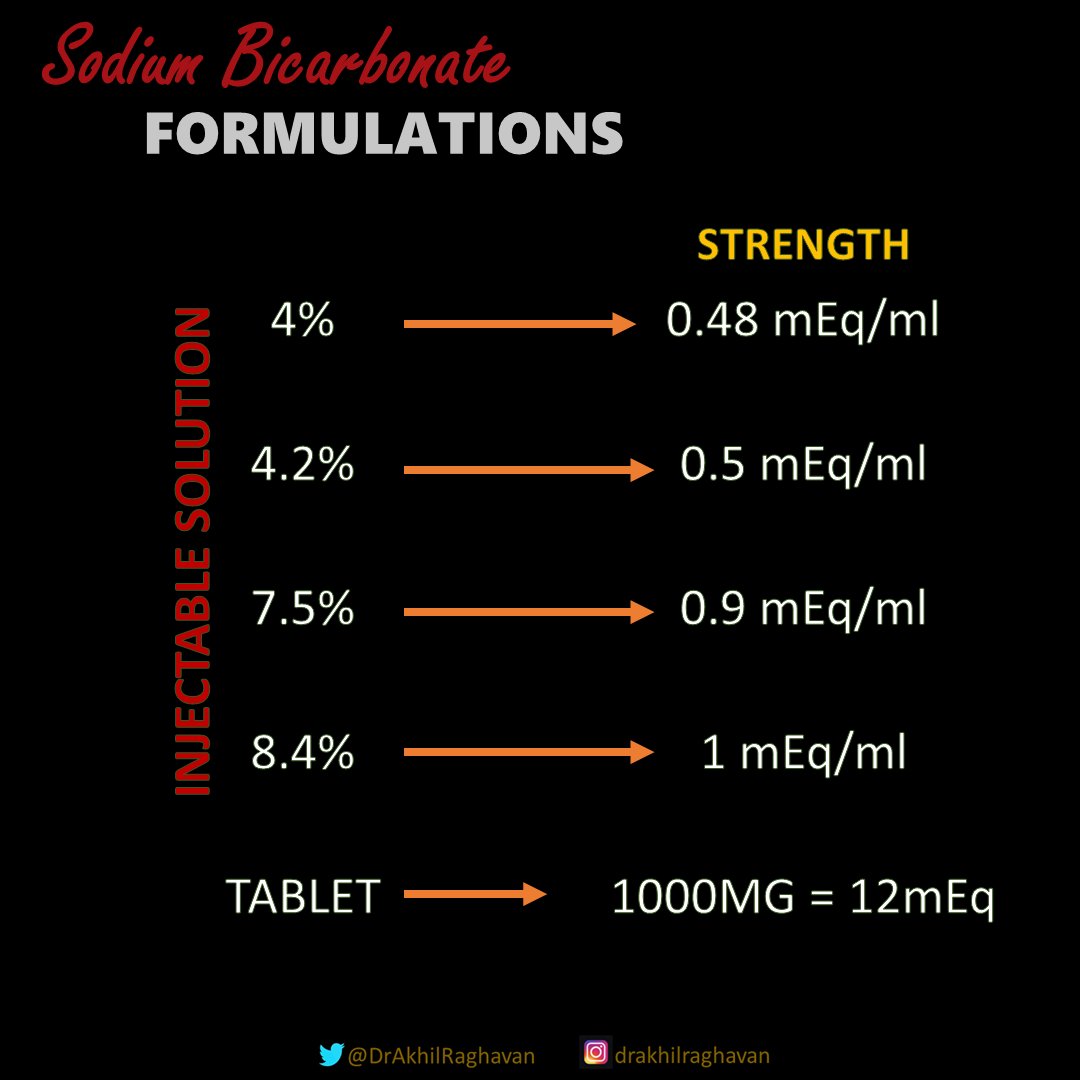
Formulations:
Various formulations in various strength and volume are available.
10ml ampoules of 7.5% NaHCO3 are commonly available in india.
50ml ampoules of 8.4% NaHCO3 are common in the west.
Various formulations in various strength and volume are available.
10ml ampoules of 7.5% NaHCO3 are commonly available in india.
50ml ampoules of 8.4% NaHCO3 are common in the west.
It can be administered as boluses or drip.
Protocol of administration differs according to indication.
Protocol of administration differs according to indication.
Drip/infusion can be administered in concentrations ranging from 1.3% bicarbonate isotonic drip (prepared by adding 150 mEq in 1000ml 5% Dextrose) or if fluid overload is a concern, in various concentrations upto maximum concentration being undiluted 1 mEq/ml solution.
The rate of administration ranges from 2mEq/kg IV boluses (in Na channel blocker toxicity) to infusions as slow as 10-12 mEq/hr (in hyperk).
Unless indicated to use specific rate of infusion it is advisable to give NaHCO3 at a ratenot more than 1.5mEq/kg/hr to⬇️ adverse effects
Unless indicated to use specific rate of infusion it is advisable to give NaHCO3 at a ratenot more than 1.5mEq/kg/hr to⬇️ adverse effects
SEVERE LACTIC ACIDOSIS can impair myocardial contractility. Alkali therapy is generally advocated for acute, severe acidemia (pH <7.00) to improve cardiovascular function.
It is not indicated as empirical therapy in treatment of lactic acodosis as it can be harmful.
It is not indicated as empirical therapy in treatment of lactic acodosis as it can be harmful.
The goal of Rx in lactic acidosis is to correct the underlying metabolic abnormality.
Alkali therapy aimed at correcting the pH is a desperate last attempt.
Hemodialysis solely for the Rx of metabolic acidosis other than that associated with renal failure is rarely beneficial
Alkali therapy aimed at correcting the pH is a desperate last attempt.
Hemodialysis solely for the Rx of metabolic acidosis other than that associated with renal failure is rarely beneficial
SEVERE ACIDEMIA (pH<7) OR SHOCK are the only two indications for bicarbonate therapy in DKA.
NaHCO3 is administered IV, as a slow infusion of 50 meq diluted in 300 mL of a saline solution, over 30-45 min, during the initial 1-2 h of therapy.
Avoid bolus administration.
NaHCO3 is administered IV, as a slow infusion of 50 meq diluted in 300 mL of a saline solution, over 30-45 min, during the initial 1-2 h of therapy.
Avoid bolus administration.
A reasonable initial goal in DKA is to increase the [HCO3 -] to 10-12 mmol/L and the pH to approximately 7.20, but clearly not to increase these values to normal.
Limited amounts of NaHCO3 should be administered to avoid cerebral edema. NaHCO3 can also precipitate hypokalemia.
Limited amounts of NaHCO3 should be administered to avoid cerebral edema. NaHCO3 can also precipitate hypokalemia.
CKD WITH ACIDOSIS
High anion gap metabolic acidosis attributable to a nonmetabolizable anion due to advanced kidney failure ("uremic" acidosis) should receive alkali therapy as it can be lifesaving in a setting of delayed dialysis.
High anion gap metabolic acidosis attributable to a nonmetabolizable anion due to advanced kidney failure ("uremic" acidosis) should receive alkali therapy as it can be lifesaving in a setting of delayed dialysis.
In CKD bicarbonate deficit should be calculated and NaHCO3 can be infused to increase the plasma [HCO3-] upto 22mmol/L.
IV NaHCO3 can be infused in various concentrations upto maximum concentration being undiluted 1 mEq/ml solution and at a rate not exceeding of 1.5mEq/kg/hr.
IV NaHCO3 can be infused in various concentrations upto maximum concentration being undiluted 1 mEq/ml solution and at a rate not exceeding of 1.5mEq/kg/hr.
METABOLIC ACIDOSIS IN DIARRHOEA
Diarrhea usually produces a hyperchloremic metabolic acidosis (NAGMA) from bicarbonate losses in stool.
Bicarbonate therapy should be given slowly to increase the plasma [HCO3-] to a target value of 22 mmol/L.
Diarrhea usually produces a hyperchloremic metabolic acidosis (NAGMA) from bicarbonate losses in stool.
Bicarbonate therapy should be given slowly to increase the plasma [HCO3-] to a target value of 22 mmol/L.
In diarrhea, sodium bicarbonate can be infused as an isotonic 1.3% bicarbonate drip (made by adding 150 mEq NaHCO3 in 1000ml 5% Dextrose) at a rate of 250ml/hr.
20 - 40 mEq of potassium should be added to this drip as hypokalemia is a concern.
20 - 40 mEq of potassium should be added to this drip as hypokalemia is a concern.
HYPERKALEMIA
Intravenous bicarbonate has no role in the acute treatment of hyperkalemia, but may slowly attenuate hyperkalemia with sustained administration over several hours.
Hypertonic intravenous bolus of undiluted ampules of NaHCO3 has little effect on potassium levels.
Intravenous bicarbonate has no role in the acute treatment of hyperkalemia, but may slowly attenuate hyperkalemia with sustained administration over several hours.
Hypertonic intravenous bolus of undiluted ampules of NaHCO3 has little effect on potassium levels.
Toxicity associated with ingestion of methanol, ethylene glycol, diethylene glycol, phenol and formic acid should be treated with specific therapeutic measures as indicated.
NaHCO3 should be given if pH falls below 7.3 and correction should be done till pH normalises(7.35-7.45)
NaHCO3 should be given if pH falls below 7.3 and correction should be done till pH normalises(7.35-7.45)

SALICYLATE TOXICITY:
Urine alkalinization is advisable in patients with salicylate levels greater than 30 mg/dL, significant acid-base disturbance, or increasing salicylate levels.
This is most often achieved via administration of a isotonic bicarbonate drip.
Urine alkalinization is advisable in patients with salicylate levels greater than 30 mg/dL, significant acid-base disturbance, or increasing salicylate levels.
This is most often achieved via administration of a isotonic bicarbonate drip.
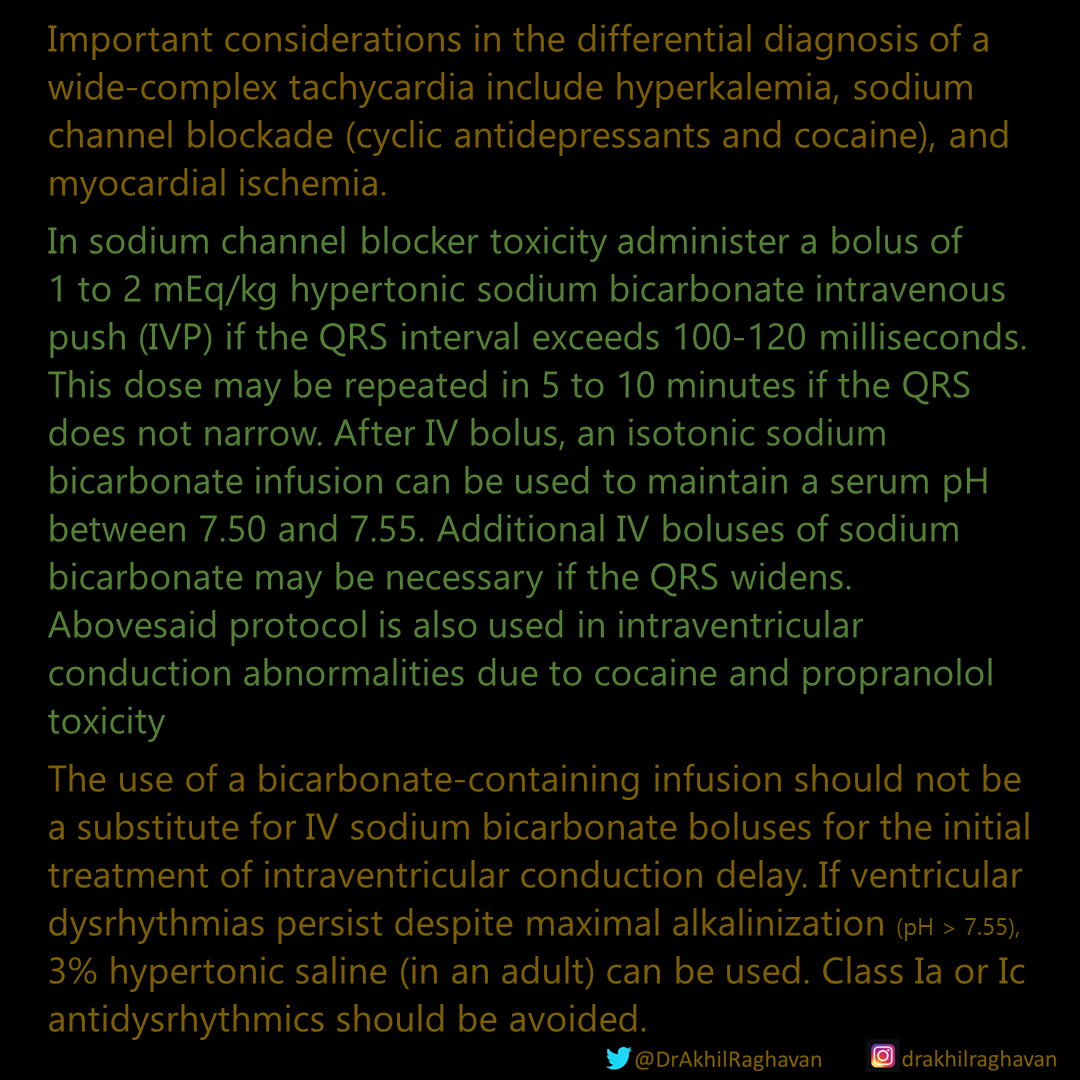
Management of Intraventricular conduction defects manifesting as widened QRS complex in ECG in cases of sodium channel blocker toxicity (TCA, SNRI, Class 1 antiarryhthmics, antihistaminics), cocaine toxicity and propranolol toxicity
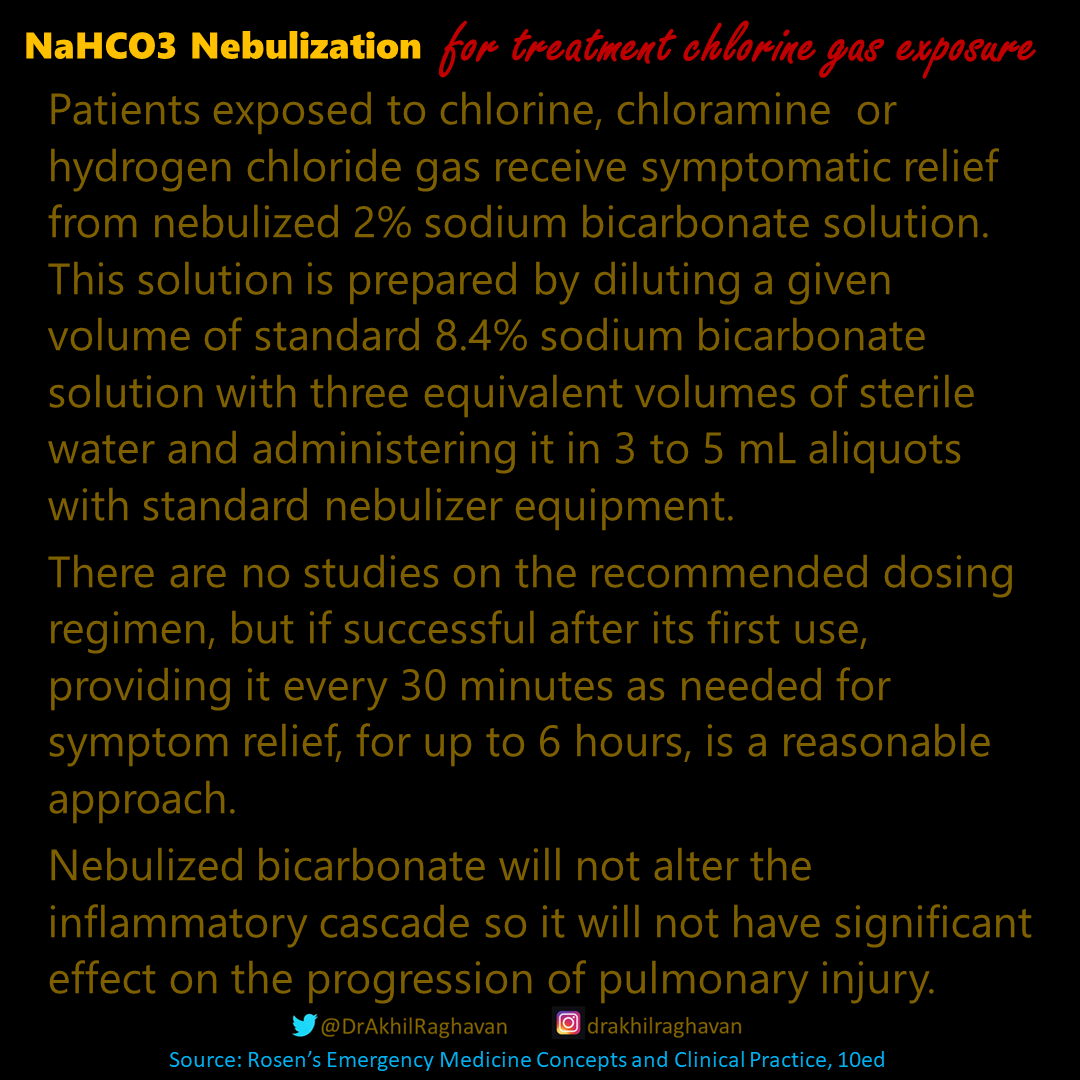
Nebulisation of NaHCO3 can be used in patients exposed to chlorine, chloramine or hydrogen chloride gas.
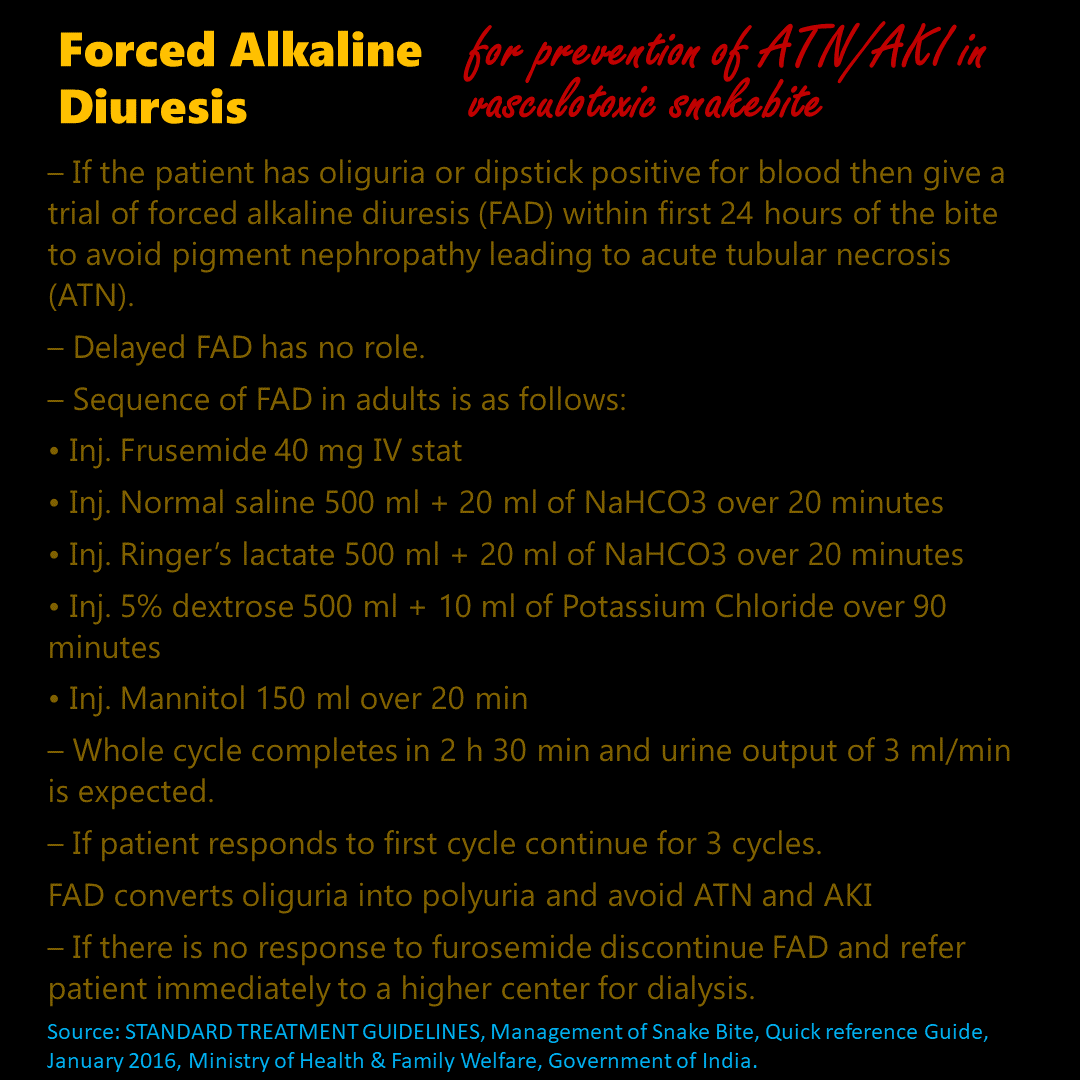
Forced Alkaline Diuresis (FAD) is mentioned in standard treatment guidelines on management of snake bite by ministry of health & family welfare, Government of India and can help in prevention of ATN/AKI in vasculotoxic snake bite.
URANIUM ISOTOPE INHALATION/INGESTION
Isotonic 1.3% bicarbonate infusion to maintain a urinary pH of 8-9 is given which will prevent nephrotoxic effects of uranium.
Treatment is given for 3 days.
Isotonic 1.3% bicarbonate infusion to maintain a urinary pH of 8-9 is given which will prevent nephrotoxic effects of uranium.
Treatment is given for 3 days.
Bicarbonate therapy is of questionable value in the following
💥Tumour Lysis Syndrome
💥Rhabdomyolysis
💥Prevention of contrast induced nephropathy
💥Lithium overdose
💥Barbiturate poisoning
💥Cardiac arrest (except if caused by Na channel blocker overdose where it has a role).
💥Tumour Lysis Syndrome
💥Rhabdomyolysis
💥Prevention of contrast induced nephropathy
💥Lithium overdose
💥Barbiturate poisoning
💥Cardiac arrest (except if caused by Na channel blocker overdose where it has a role).
References
I couldn’t get a standard textbook reference regarding the maximum rate of infusion of NaHCO3. It is mentioned to be not more than 1.5mEq/kg/hr in package inserts
I couldn’t get a standard textbook reference regarding the maximum rate of infusion of NaHCO3. It is mentioned to be not more than 1.5mEq/kg/hr in package inserts

Loading suggestions...