

Few slides from the talk I gave for @GlomCon virtual fellowship program break out room #NephTwitter #MedTwitter @nephrologista @whattheneph @LaniShochet @hollylhutton @BrixSilke @JasmineNephro
🧵 tweetorial alert 🚨
🔥On Assays used to detect ANCA
🧵 tweetorial alert 🚨
🔥On Assays used to detect ANCA
📍 You test for ANCA serology ONLY in a patient with history, clinical features suspicious of vasculitis
📍 the tests can be divided into:
✅ Indirect Immunoflorescence (IIFT)
✅ Antigen specific assays ( ELISA is just one of it )
PANCA(IIF pattern) -> MPO(antigen specific assay) ->MPA
CANCA(IIF pattern) -> PR3(antigen specific assay) -> GPA
📍 the tests can be divided into:
✅ Indirect Immunoflorescence (IIFT)
✅ Antigen specific assays ( ELISA is just one of it )
PANCA(IIF pattern) -> MPO(antigen specific assay) ->MPA
CANCA(IIF pattern) -> PR3(antigen specific assay) -> GPA
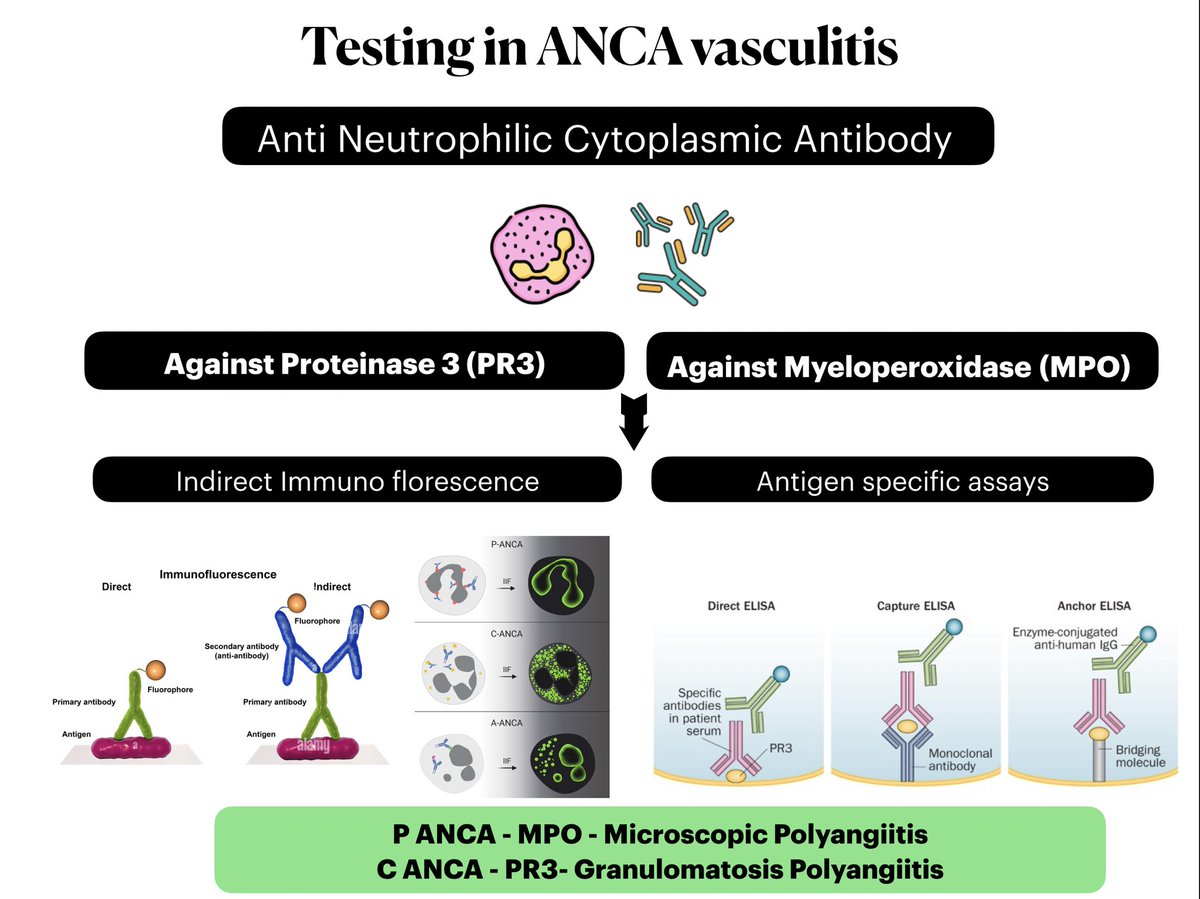
📍 Indirect Immunoflorescence : 🥢 antibodies in the serum of patient bind to the antigens in Neutrophil granules -> add another antibody which is bound to flourophore 🟢 FITC (Hence indirect )
📍 antigen specific assays : The antigen (PR3 or MPO ) is isolated and immobilised on a
✅ ELISA plate in ELISA
✅ Bead on bead assays
✅ depending on the particular assay
Patient sera is added to the Immobilised antigen
📍 antigen specific assays : The antigen (PR3 or MPO ) is isolated and immobilised on a
✅ ELISA plate in ELISA
✅ Bead on bead assays
✅ depending on the particular assay
Patient sera is added to the Immobilised antigen
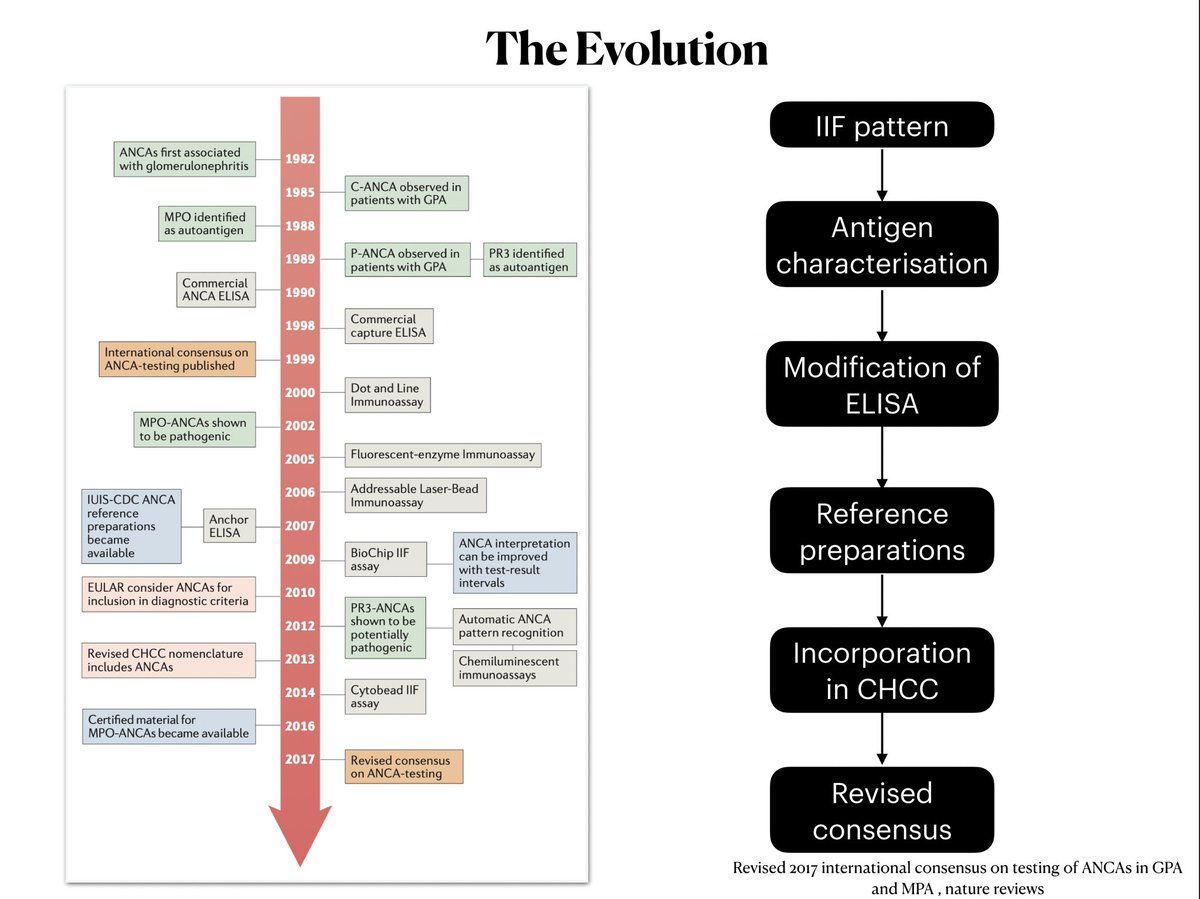
📍 How did the test to detect ANCA evolve over time ?
✅ First tests were Immunoflorescence
✅ Antigens were characterised
✅ Modification of ELISA (To make it more sensitive )
✅ Inclusion of ANCA in Chappel hill classification
✅ Modification of consensus (1999 —> 2017 )
✅ First tests were Immunoflorescence
✅ Antigens were characterised
✅ Modification of ELISA (To make it more sensitive )
✅ Inclusion of ANCA in Chappel hill classification
✅ Modification of consensus (1999 —> 2017 )
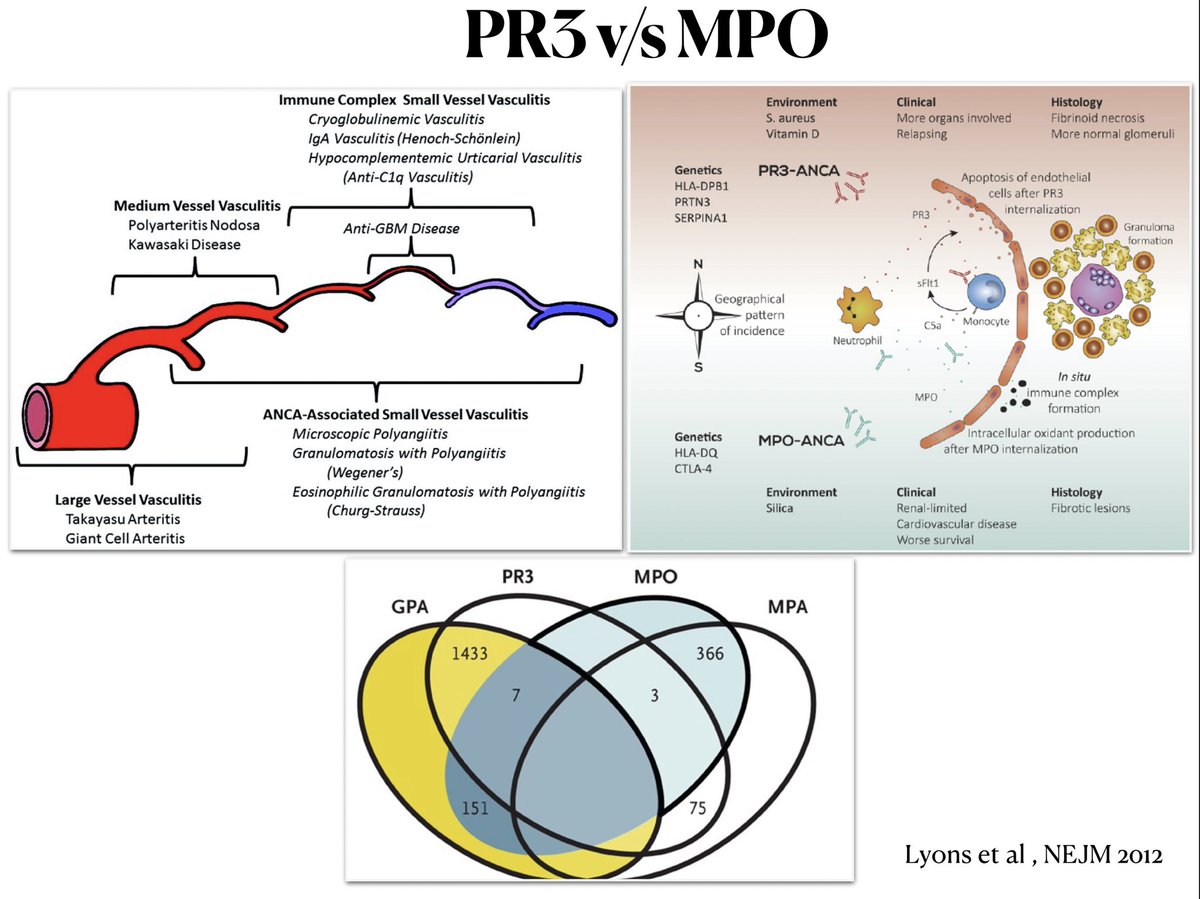
📍 should we classify the vasculitis based on serological pattern(MPO V/S PR3) OR the clinico pathological classification (GPA V/S MPO)
✅ genetic studies (GWAS) shows there is a clear
Genetic basis for such a serological classification
✅ PR 3 associated disease : Multisystemic relapsing and necrotising
✅ MPO : Mostly renal limited and fibrosing
🔥 LOTS OF OVERLAP AND CROSS OVER
✅ genetic studies (GWAS) shows there is a clear
Genetic basis for such a serological classification
✅ PR 3 associated disease : Multisystemic relapsing and necrotising
✅ MPO : Mostly renal limited and fibrosing
🔥 LOTS OF OVERLAP AND CROSS OVER
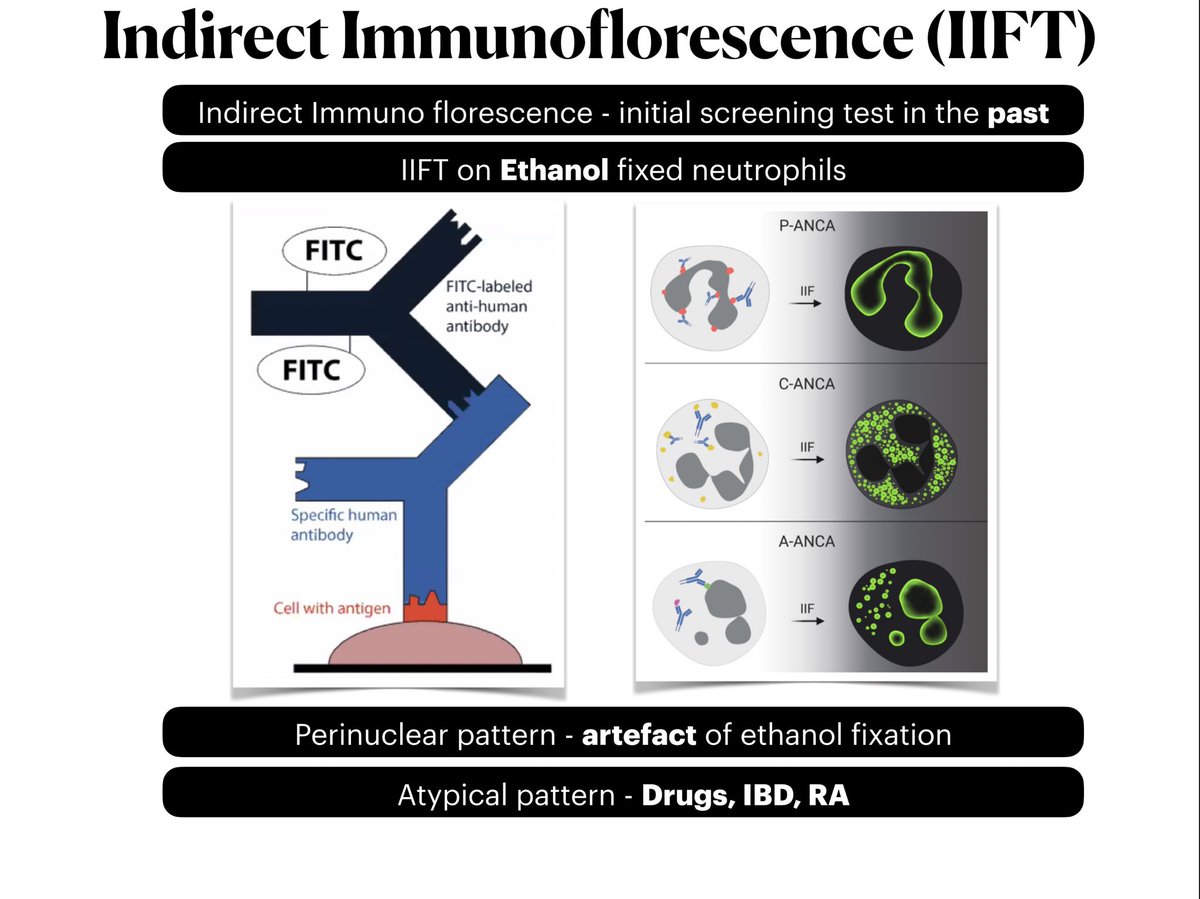
📍Indirect immunofluorescence : USED to be the initial screening test
✅ IIFT done on ethanol fixed neutrophils
✅ P ANCA pattern -> artefact of ethanol fixation
Ethanol solubilises the neutrophilic MPO granules to cationic which go bind to negative nuclei
✅ atypical ANCA : in non vasculitic conditions
✅ IIFT done on ethanol fixed neutrophils
✅ P ANCA pattern -> artefact of ethanol fixation
Ethanol solubilises the neutrophilic MPO granules to cationic which go bind to negative nuclei
✅ atypical ANCA : in non vasculitic conditions
📍 P ANCA can be confused with Nuclear staining
✅ IIF on formalin fixed neutrophils versus ethanol fixed neutrophils can give a clue
✅ Computer generated image analysis of IIF : as good as conventional method
✅ IIF on formalin fixed neutrophils versus ethanol fixed neutrophils can give a clue
✅ Computer generated image analysis of IIF : as good as conventional method

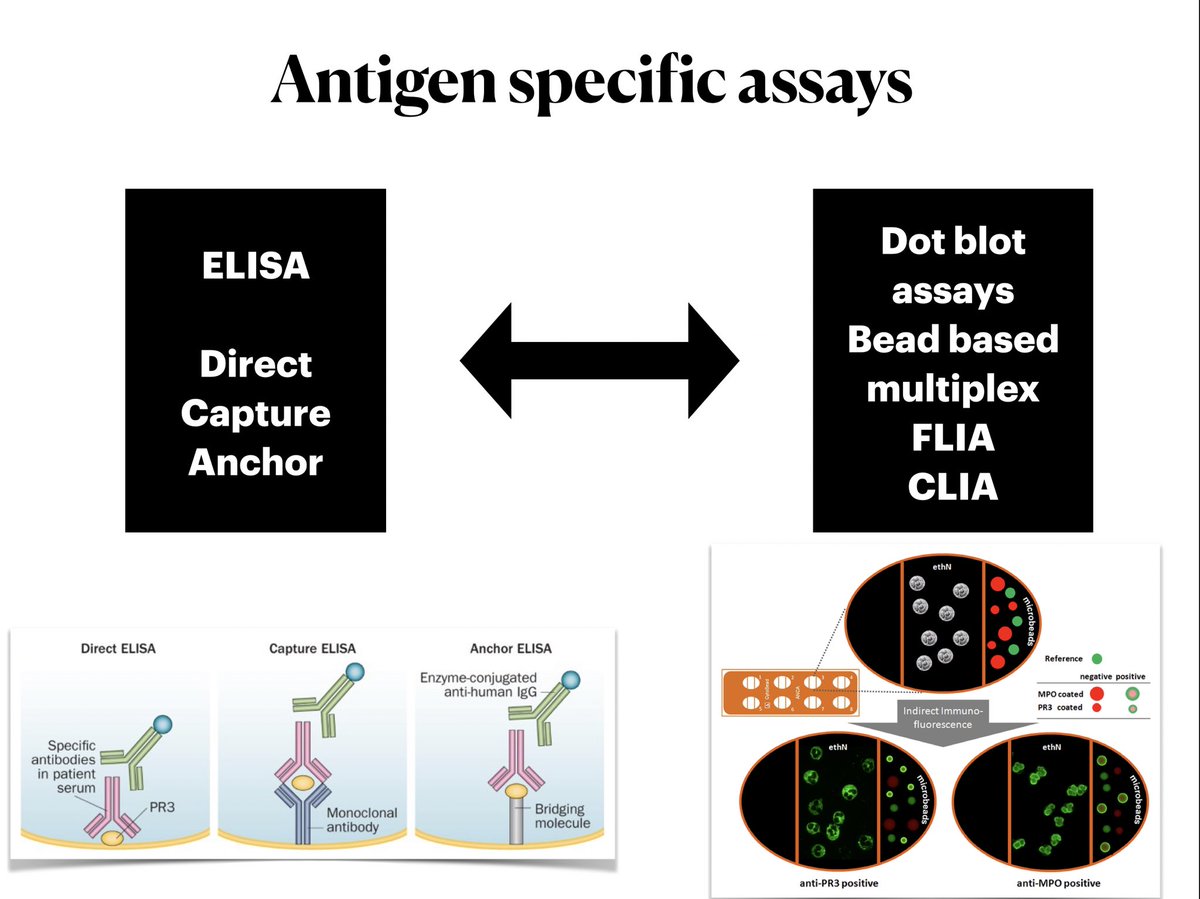
📍 Antigen specific assays
✅ ELISA is one among the many antigen specific assays
✅ ELISA is one among the many antigen specific assays
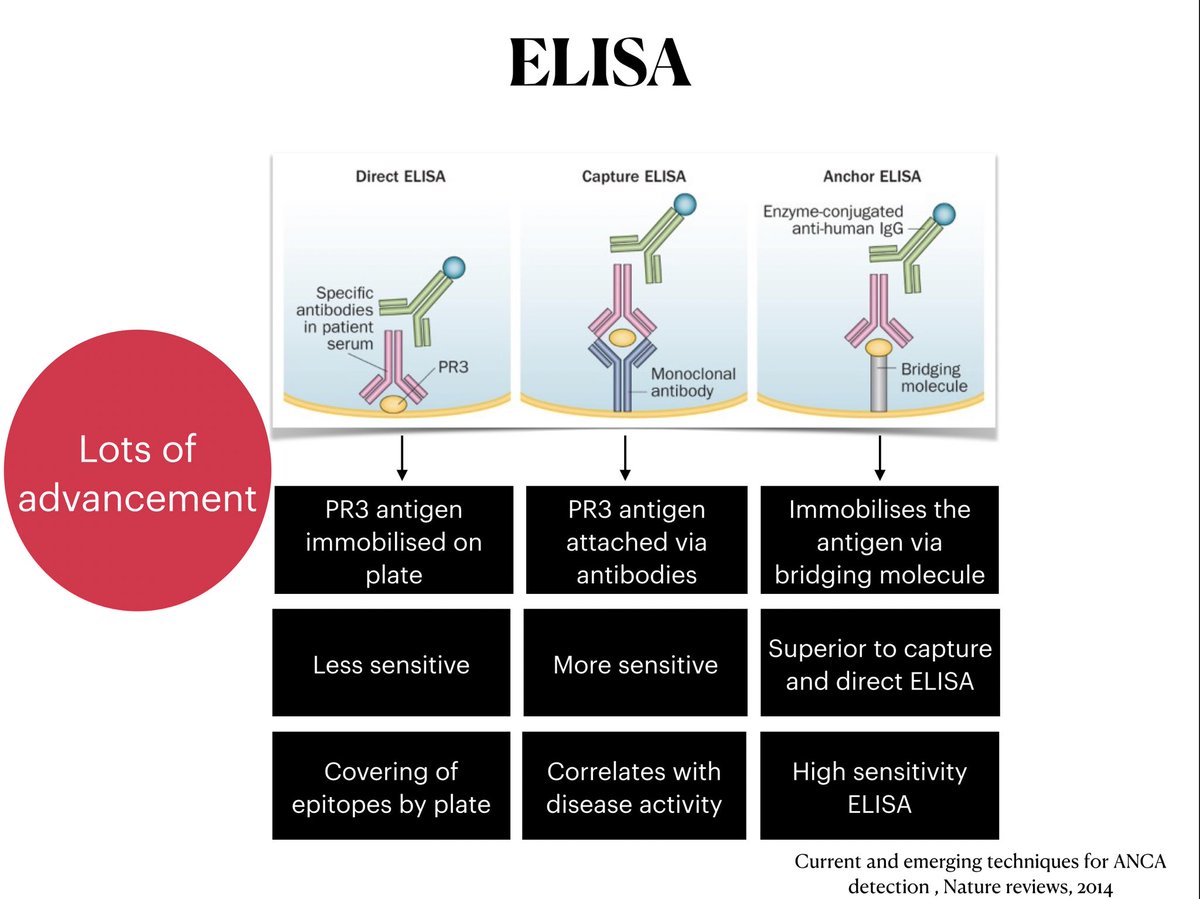
📍 The modifications of ELISA
✅ the epitopes of antigen are buried away by the plate
Making it less sensitive
✅ capture and Anchor ELISA exposes more epitope of the antigen for the paratope of antibody to bind
✅ the ELISA evolved to give better sensitivity and specificity
✅ the epitopes of antigen are buried away by the plate
Making it less sensitive
✅ capture and Anchor ELISA exposes more epitope of the antigen for the paratope of antibody to bind
✅ the ELISA evolved to give better sensitivity and specificity
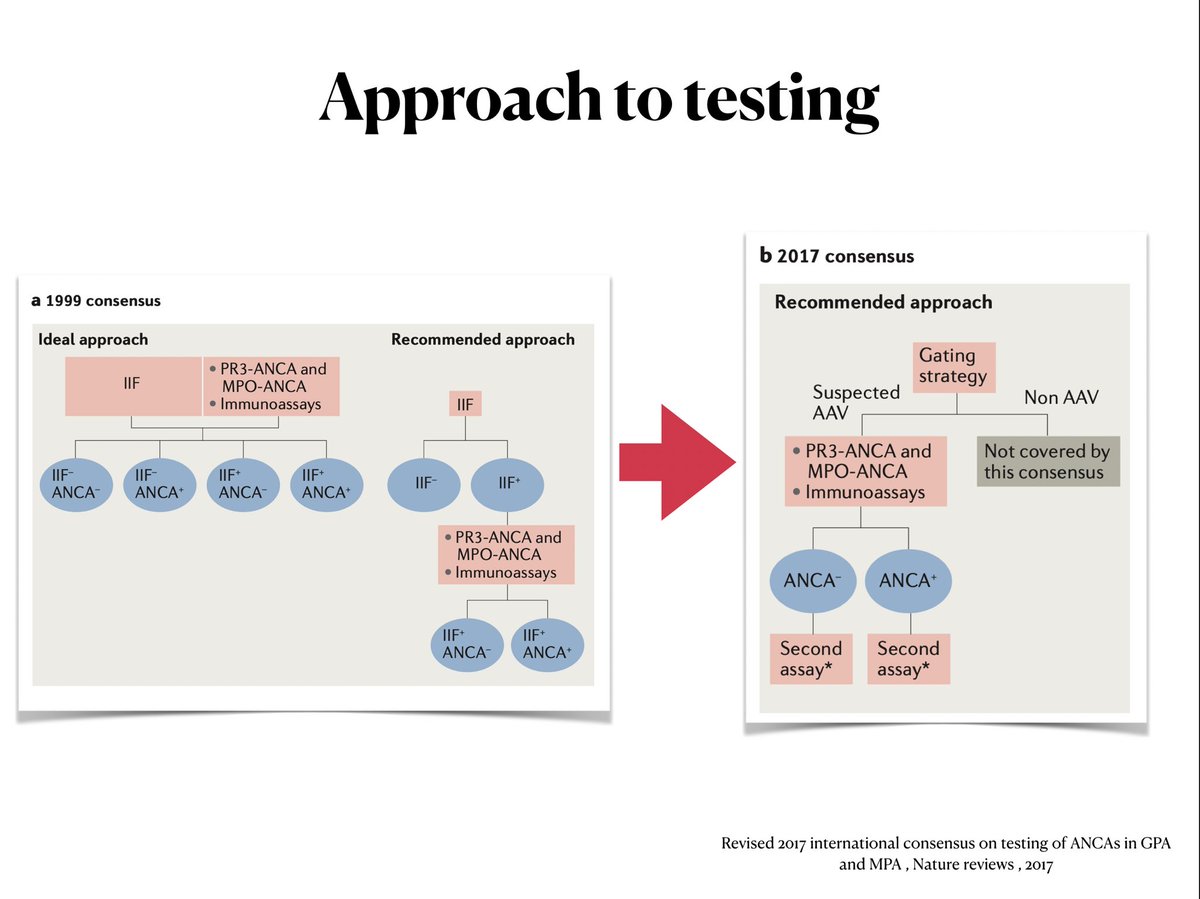
📍 With better ELISA test , the testing strategy moved from IIF based screening to antigen specific assay screening
✅ major change in 1999 consensus —> 2017 consensus
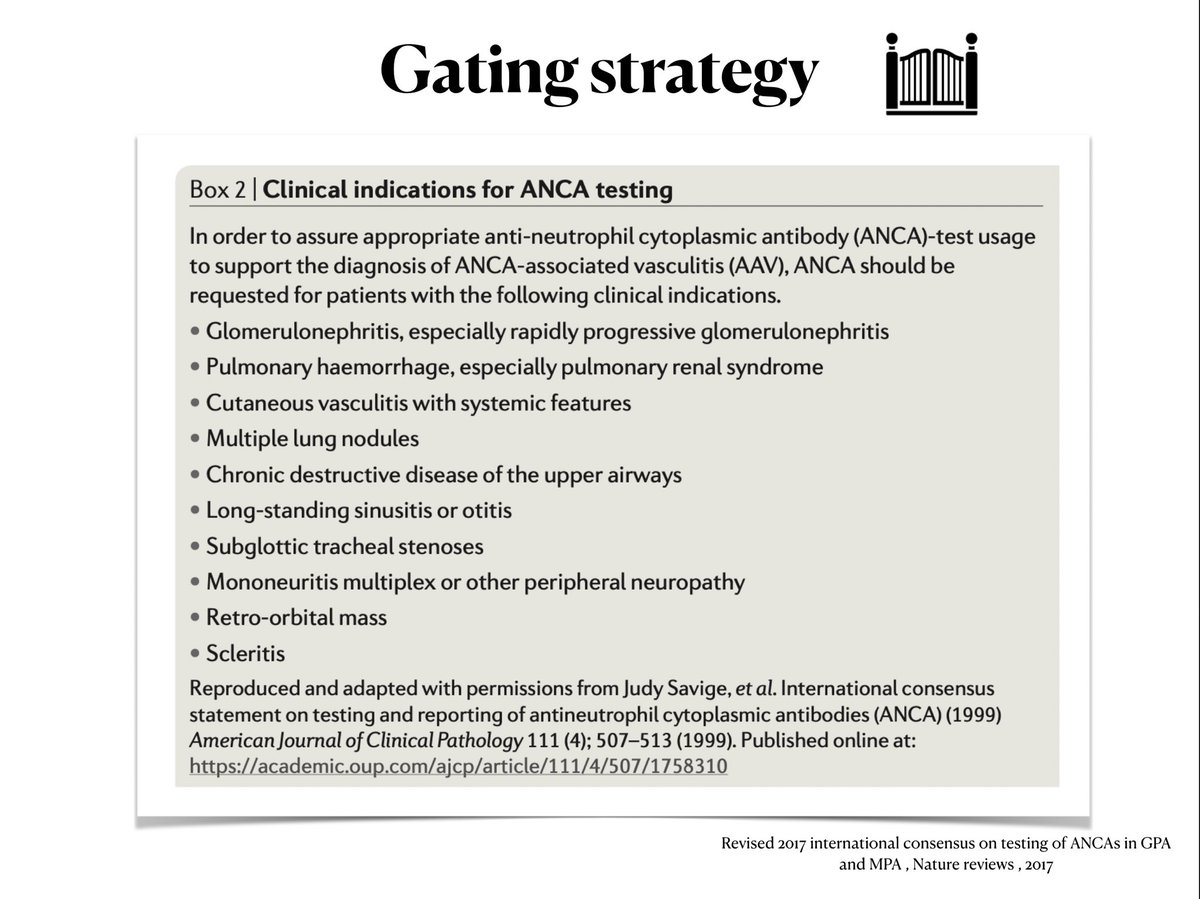
✅ Gating strategy: to do the ANCA testing in only those patients with high index of suspicion 🕵️♀️
✅ major change in 1999 consensus —> 2017 consensus
✅ Gating strategy: to do the ANCA testing in only those patients with high index of suspicion 🕵️♀️
📍 🚪 whats gating strategy ?
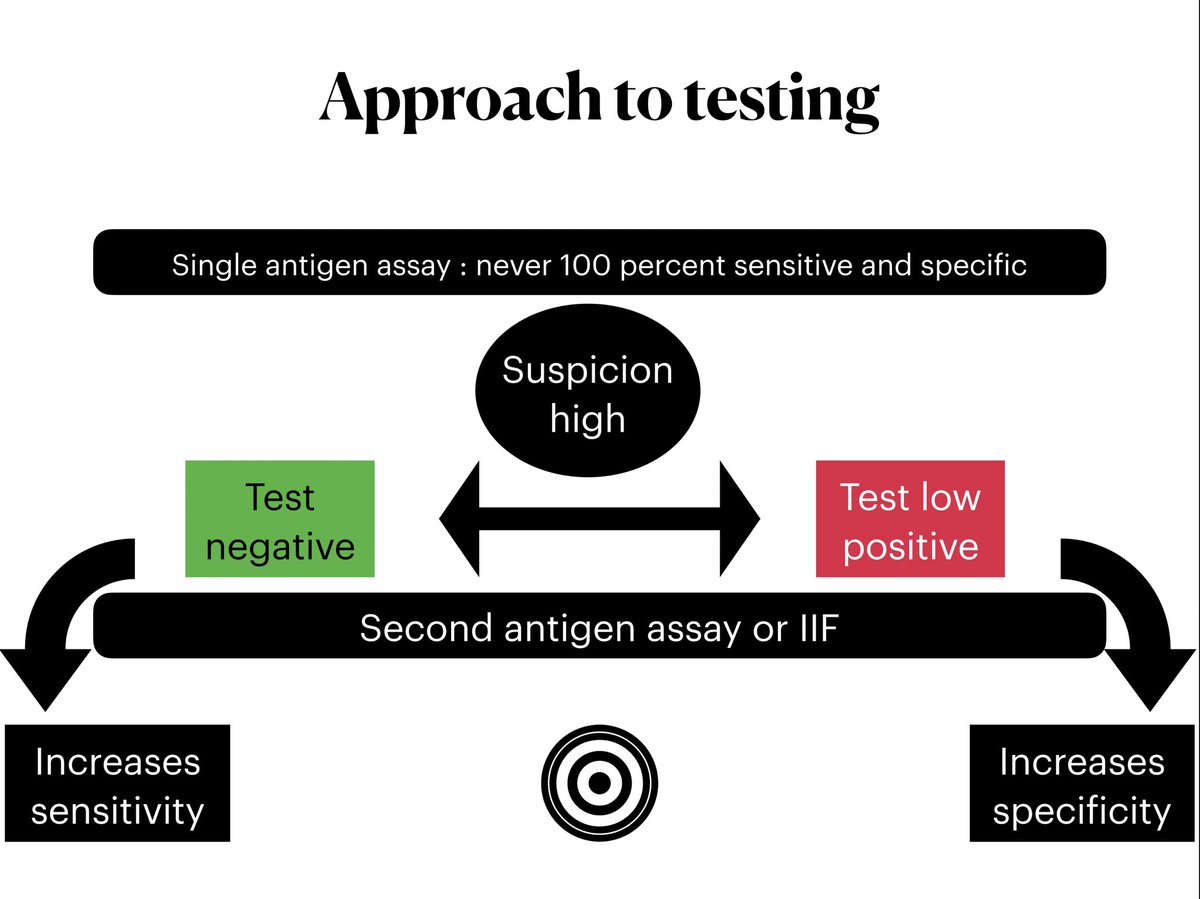
📍 what if the first ANCA testing was negative
✅ Do a second antigen specific assay
✅ or an Indirect Immunofluorescence
✅ Do a second antigen specific assay
✅ or an Indirect Immunofluorescence
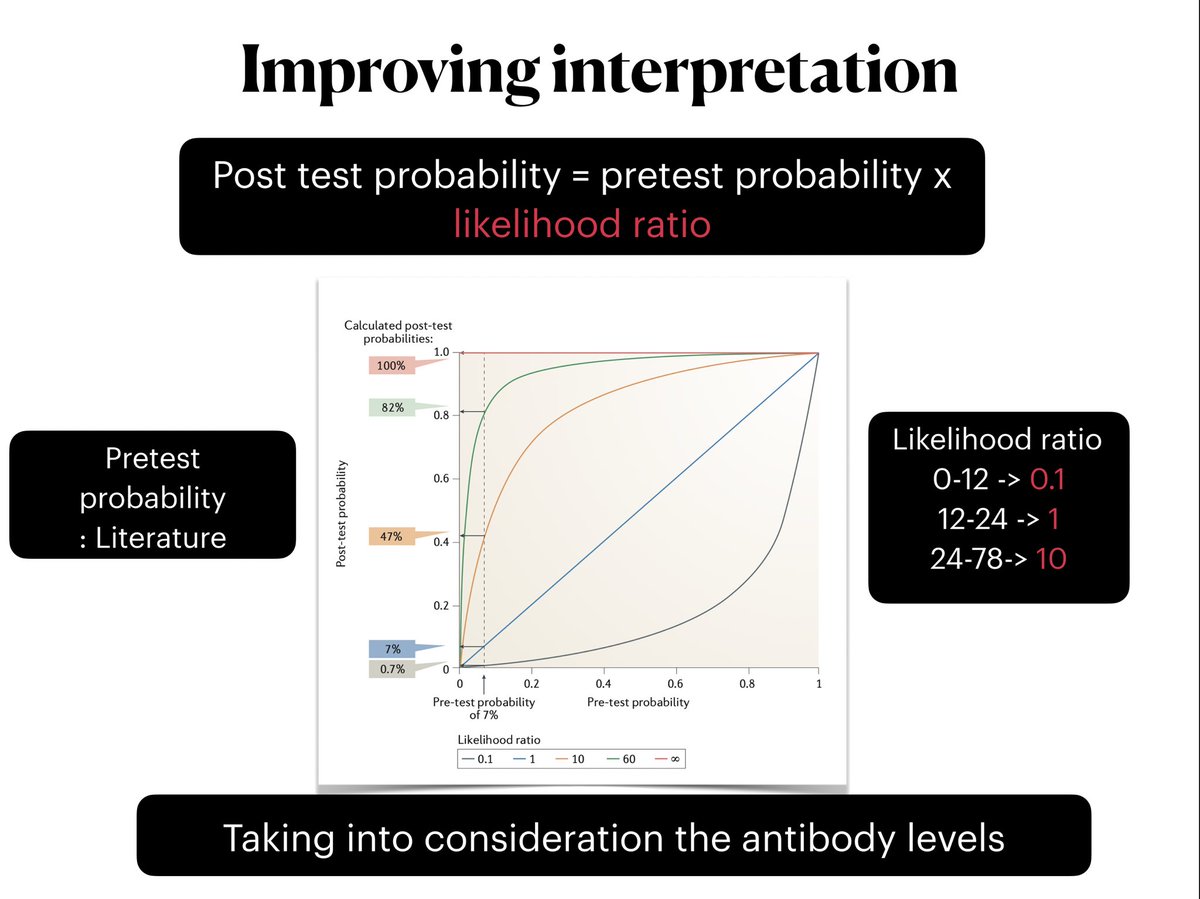
📍 Does the quantity of antibody matter ?
✅ pretest probability : got from literature for a particular symptom / presentation
✅ likelihood ratio: from the value of antibody level for that particular test
✅ This is more valuable than a binary result of positive and negative
✅ pretest probability : got from literature for a particular symptom / presentation
✅ likelihood ratio: from the value of antibody level for that particular test
✅ This is more valuable than a binary result of positive and negative
📍 few important points :
✅ Negative serology doesn’t rule out ANCA vasculitis: its a clinicopathological diagnosis supported by serology 🔴
✅ positive ANCA only contributes to but NOT DIAGNOSTIC by itself 🟢
✅ non vasculitic condition associated with ANCA positivity : GI disorders , SLE, RA, infections (endocarditis, Hep C)
✅ Drug induced ANCA - Double positivity
✅ Negative serology doesn’t rule out ANCA vasculitis: its a clinicopathological diagnosis supported by serology 🔴
✅ positive ANCA only contributes to but NOT DIAGNOSTIC by itself 🟢
✅ non vasculitic condition associated with ANCA positivity : GI disorders , SLE, RA, infections (endocarditis, Hep C)
✅ Drug induced ANCA - Double positivity
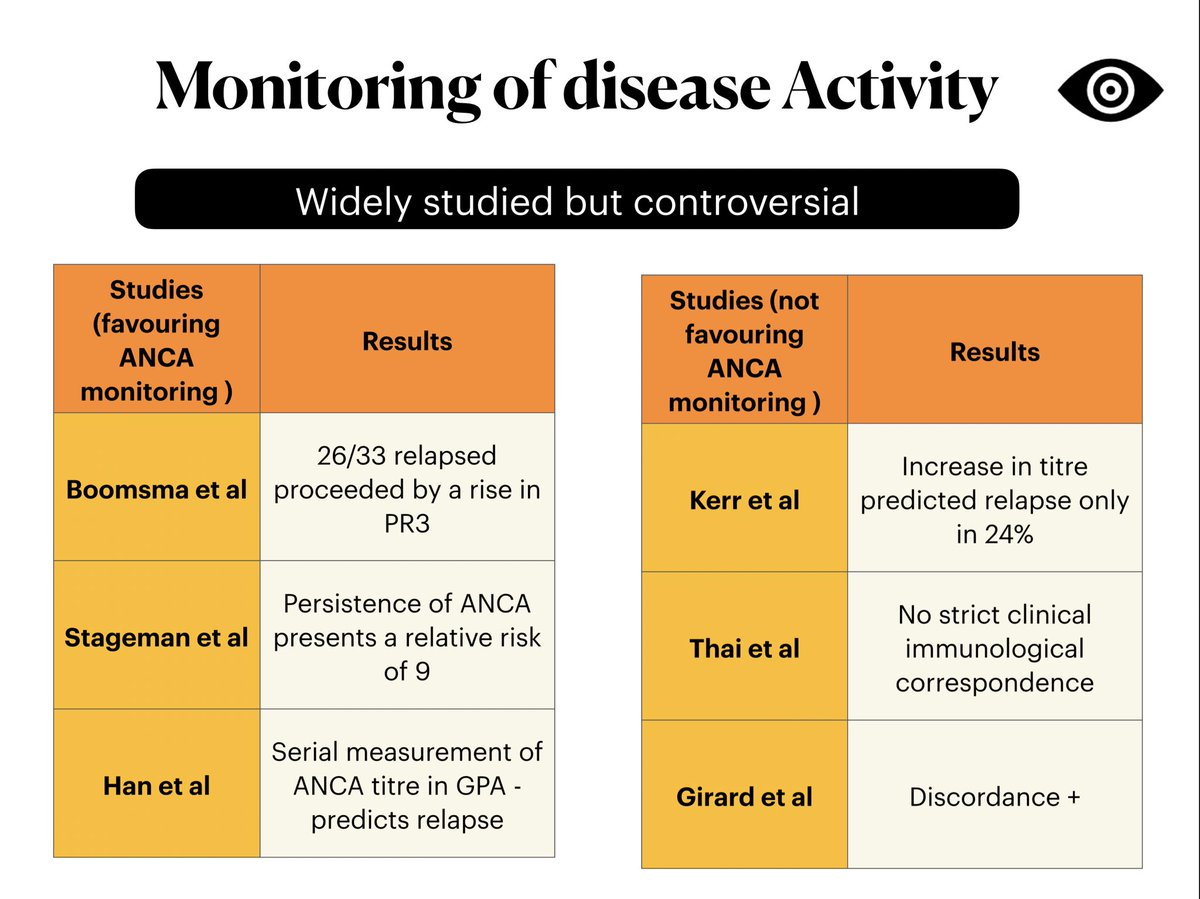
📍 once you have treated a patient and in remission , What’s the role in ANCA titre monitoring ? ⚖️
✅ 🤺 controversial evidence
✅ 🤺 controversial evidence
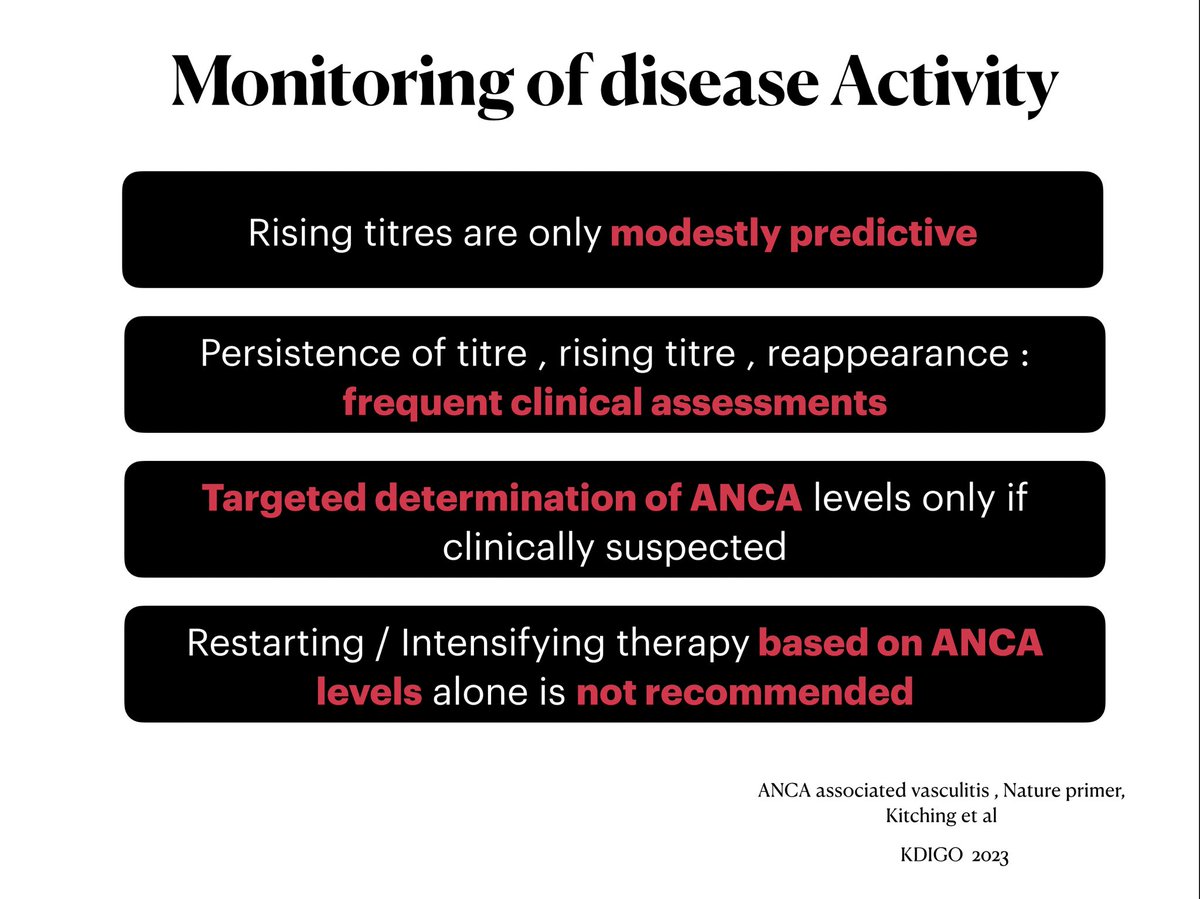
📍 Rising , reappearance of antibody should be always looked in the background of the patients clinical picture
✅ rising titres modestly predictive of relapse (KDIGO practice guidlines)
✅ If rising titres -> follow the patient closely
✅ Never restart or intensify therapy only based on rising titres ❌
✅ rising titres modestly predictive of relapse (KDIGO practice guidlines)
✅ If rising titres -> follow the patient closely
✅ Never restart or intensify therapy only based on rising titres ❌
📍 🏡 Take home messages
Loading suggestions...