

Venous variants and abnormalities are the most common causes of pulsatile tinnitus
Differential and learning points in 🧵
#ent #neurology #neurosurgery #meded #radres #futureradres @ASHNRSociety @AlbanyMedRadRes @TheENRS
Differential and learning points in 🧵
#ent #neurology #neurosurgery #meded #radres #futureradres @ASHNRSociety @AlbanyMedRadRes @TheENRS

Ddx for venous causes of PT:
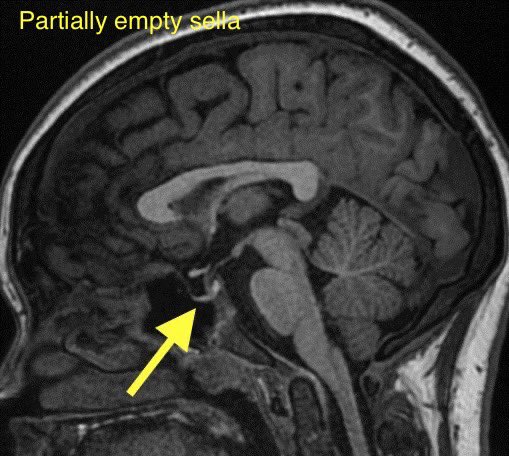
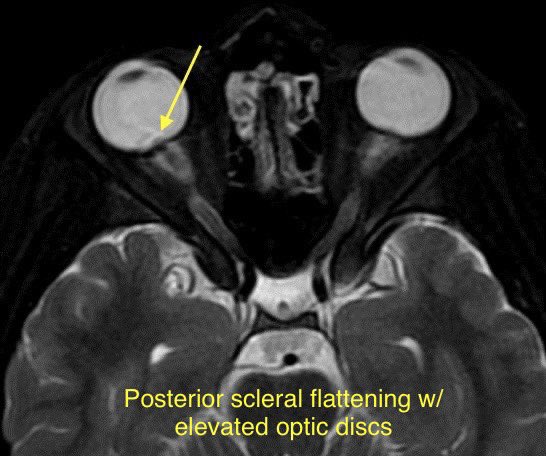
Idiopathic intracranial hypertension
Sigmoid plate dehiscence +/- diverticulum
Transverse sinus stenosis (w/ or w/o IIH)
Jugular bulb abnormalities
Dilated emissary veins
Extracranial IJ compression
Prominent occipital sinus
Occipital sinus stenosis
Idiopathic intracranial hypertension
Sigmoid plate dehiscence +/- diverticulum
Transverse sinus stenosis (w/ or w/o IIH)
Jugular bulb abnormalities
Dilated emissary veins
Extracranial IJ compression
Prominent occipital sinus
Occipital sinus stenosis
🔷Tinnitus occurs from turbulence within normally located veins and abnormally enlarged or located veins in close proximity to the conductive auditory pathways
🔷Concomitant venous findings may share the same pathophysiologic mechanism and may have additive effects causing PT
🔷Concomitant venous findings may share the same pathophysiologic mechanism and may have additive effects causing PT
🔷Many imaging findings associated with tinnitus may be seen incidentally in asymptomatic patients. If the finding is ipsilateral and there are no other findings to explain the PT then it is likely the cause.
Diagnostic algorithm 👇
Source: pubs.rsna.org
Diagnostic algorithm 👇
Source: pubs.rsna.org
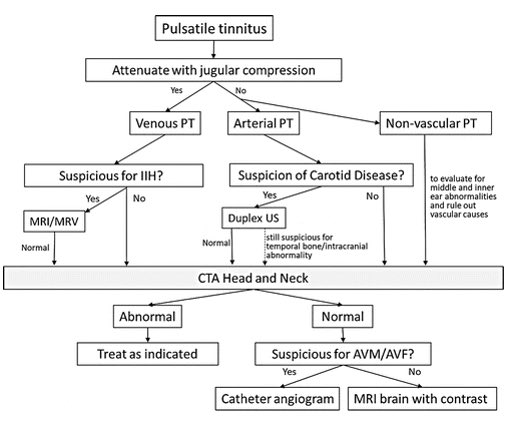
🔷Maneuvers that should alleviate venous causes of PT:
1️⃣Gentle compression of the ipsilateral IJ
2️⃣Valsalva maneuver
3️⃣Turning the patient's head toward the side lateralizing with PT
4️⃣Compression in contralateral IJ may result in temporary increase in tinnitus
1️⃣Gentle compression of the ipsilateral IJ
2️⃣Valsalva maneuver
3️⃣Turning the patient's head toward the side lateralizing with PT
4️⃣Compression in contralateral IJ may result in temporary increase in tinnitus
🔷Successful test occlusion can eradicate the tinnitus and confirm the utility of treatment while also ensuring adequate collateral drainage if considering a venous vessel sacrifice.
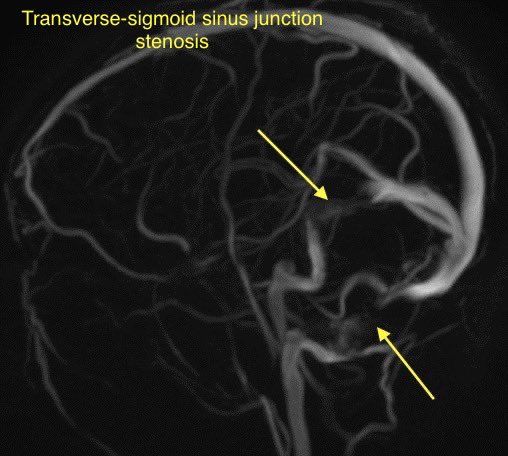
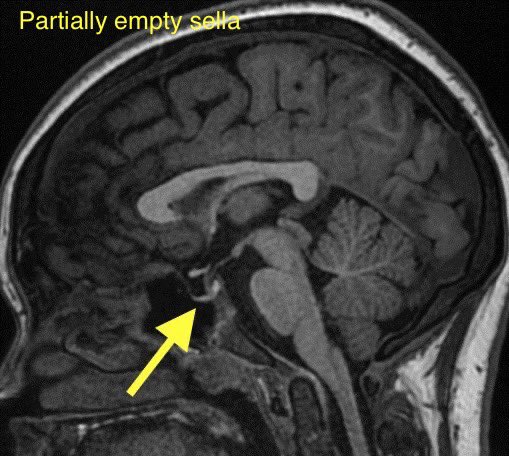
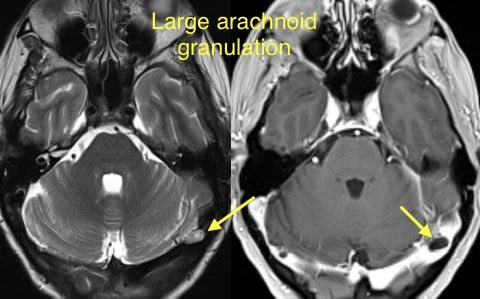
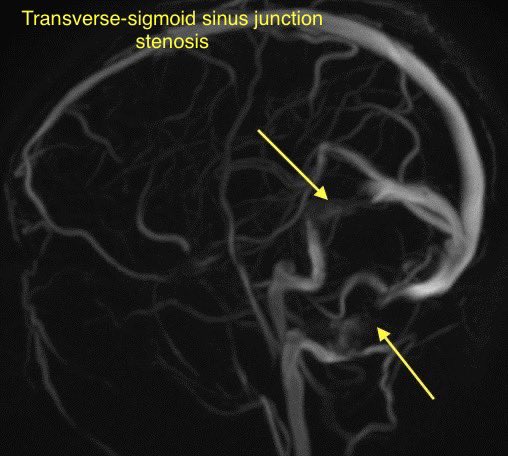
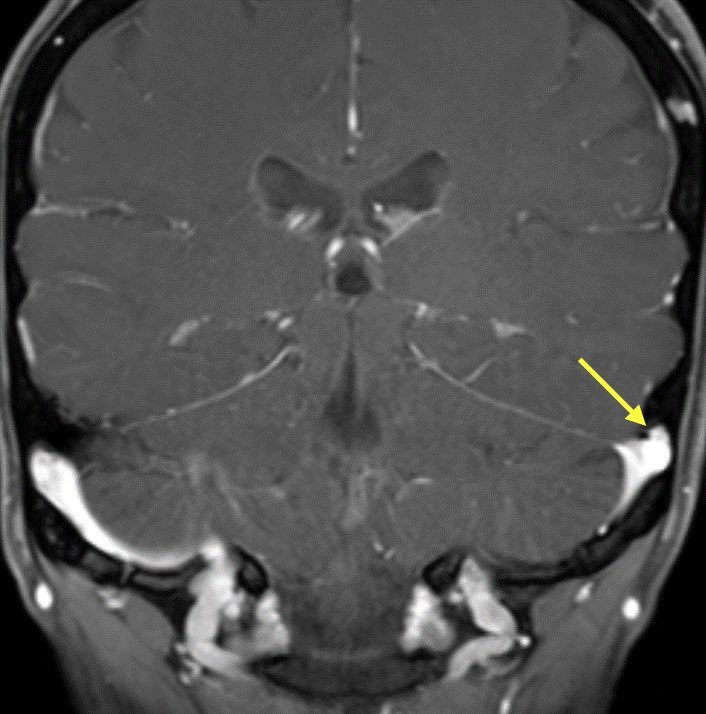
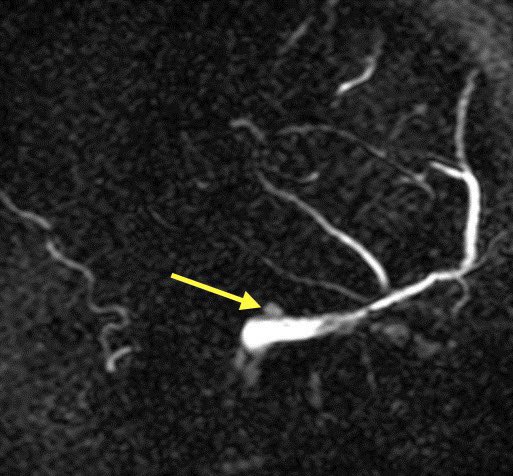
🔷TRANSVERSE SINUS STENOSIS & IDIOPATHIC INTRACRANIAL HYPERTENSION
🔸Intrinsic and extrinsic causes
🔸Intrinsic and extrinsic causes
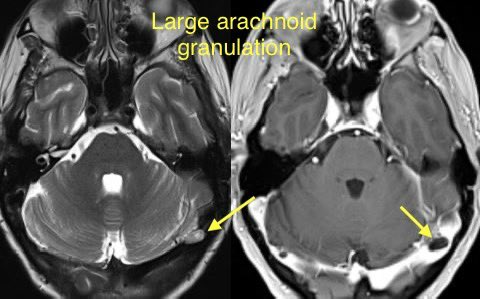
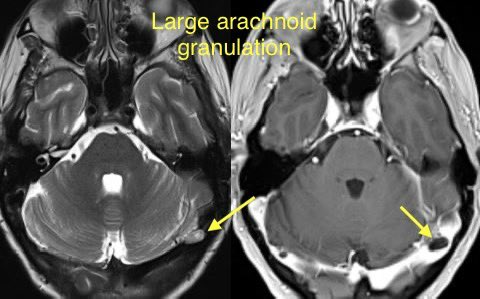
INTRINSIC: Typically arachnoid granulations
🔹Arachnoid granulations may be incidental though they can produce IIH when obstructing a dominant transverse sinus or simultaneously blocking both
🔹Look for a round/lobulated filling defect with CSF signal on all images
🔹Arachnoid granulations may be incidental though they can produce IIH when obstructing a dominant transverse sinus or simultaneously blocking both
🔹Look for a round/lobulated filling defect with CSF signal on all images
EXTRINSIC: Defined as luminal narrowing with obtuse margins
🔹Typical cause of extrinsic stenosis is IIH though can occur without signs of IIH
🔹Tinnitus is present in up to 40-60% of patients with IIH (usually pulsatile and unilateral)
🔹Typical cause of extrinsic stenosis is IIH though can occur without signs of IIH
🔹Tinnitus is present in up to 40-60% of patients with IIH (usually pulsatile and unilateral)
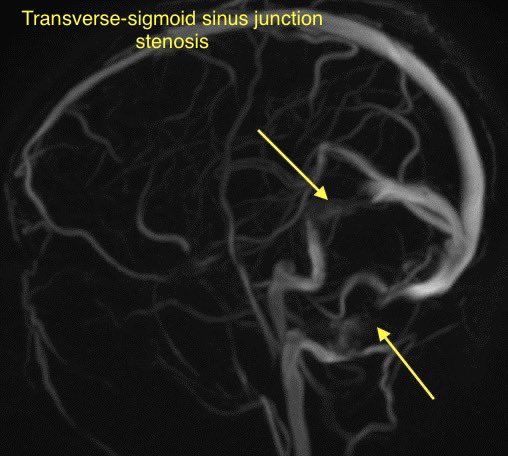

💡Bilateral transverse sinus stenosis is seen in 94% of patients with lIH
💡 Internal cephaloceles are another cause of extrinsic stenosis
💡 Stent placement is safe and effective in patients with transverse sinus stenosis (w/ or w/o lIH)
💡 Internal cephaloceles are another cause of extrinsic stenosis
💡 Stent placement is safe and effective in patients with transverse sinus stenosis (w/ or w/o lIH)
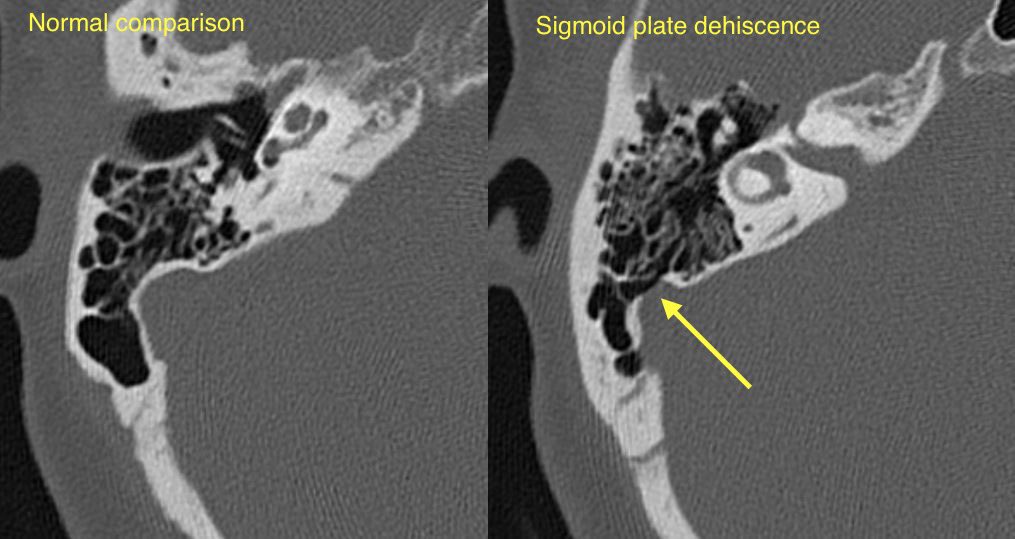
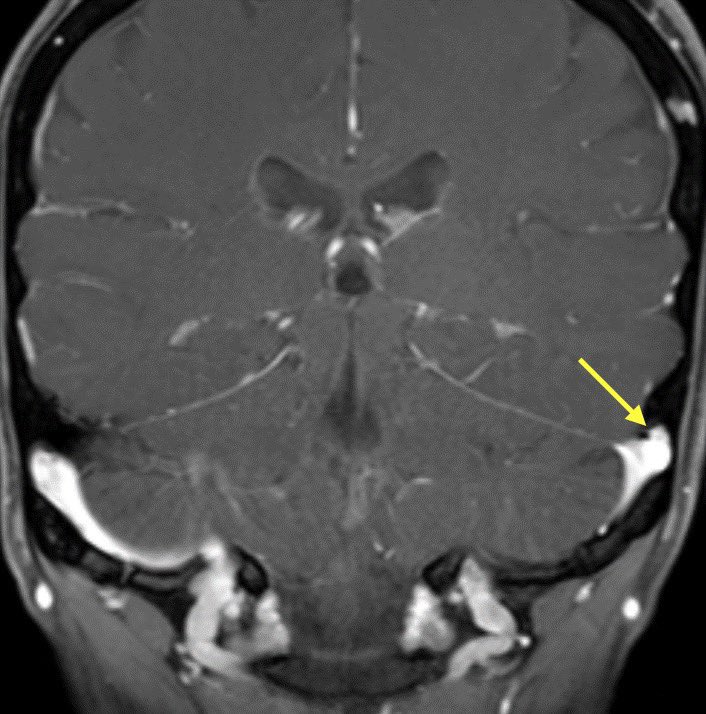
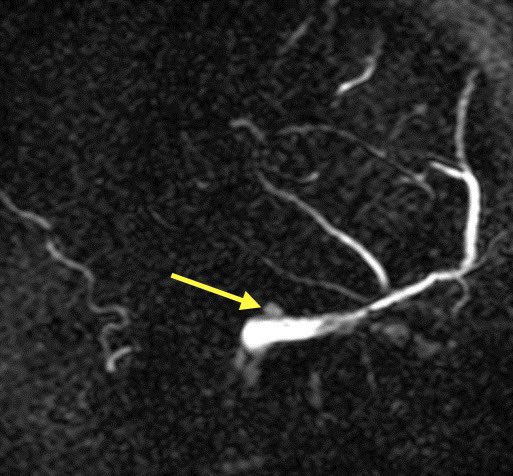
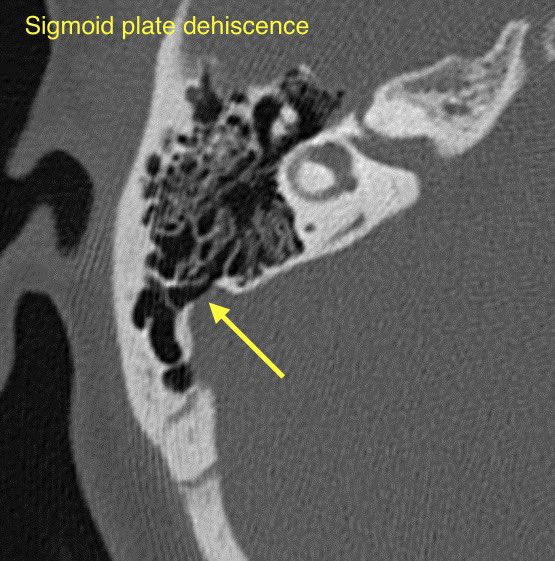
🔷SIGMOID SINUS WALL ANOMALIES
1️⃣Sigmoid plate dehiscence
2️⃣Sigmoid sinus diverticulum
1️⃣Sigmoid plate dehiscence
2️⃣Sigmoid sinus diverticulum
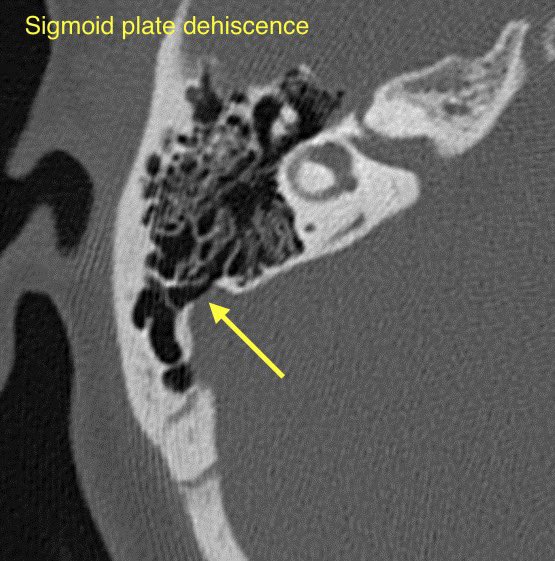
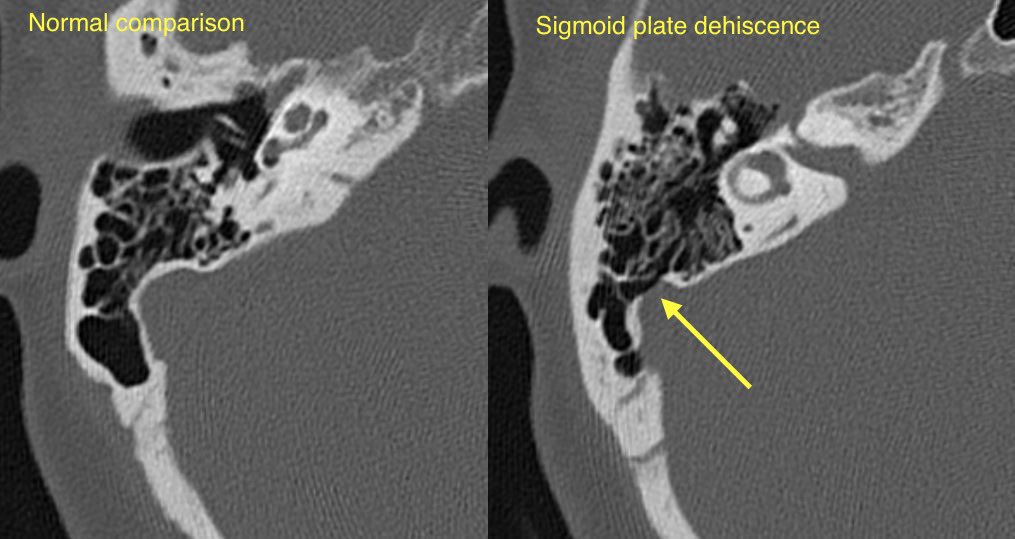
🔹Sigmoid plate dehiscence: Thinning or absence of the normal cortical bone covering the sigmoid sinus resulting in direct contact of the venous sinus wall with mastoid air cells
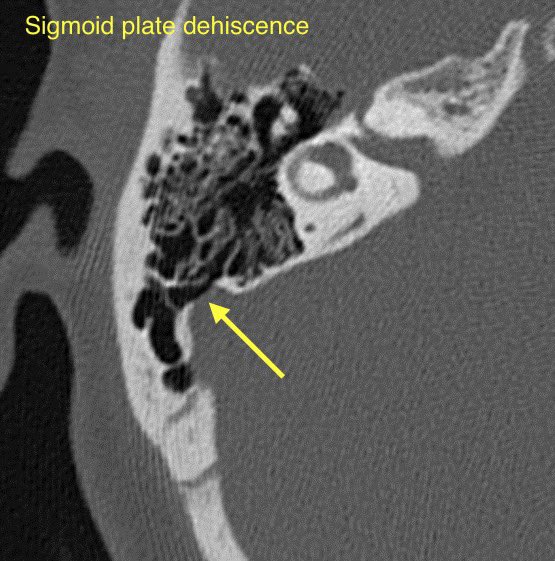

🔹Sigmoid sinus diverticulum: Lateral outpouching of the transverse sigmoid sinus junction with intrusion into the adjacent bone


💡 Sigmoid plate dehiscence w/ or w/o diverticulum is one of the most common imaging abnormalities at CT for pulsatile tinnitus (up to 40%). These findings are more prevalent in patients with TSS and IIH
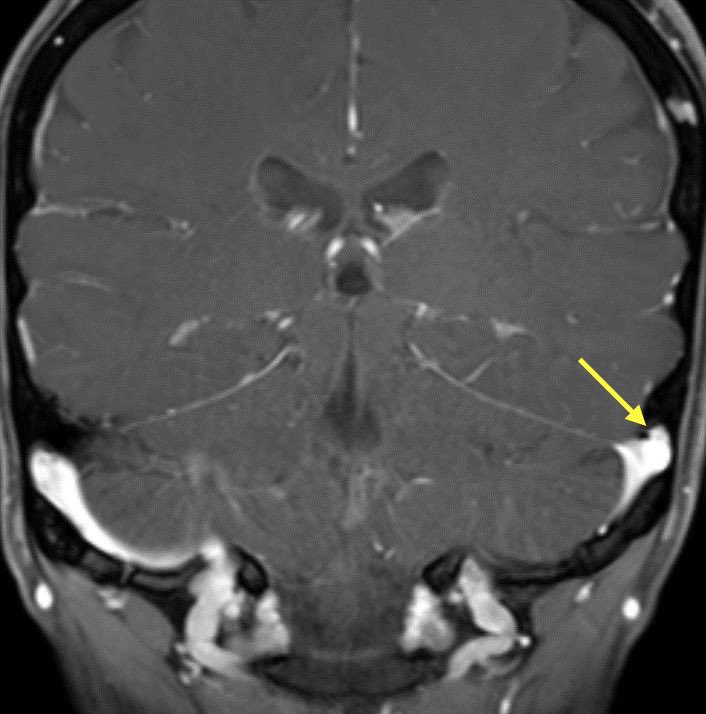
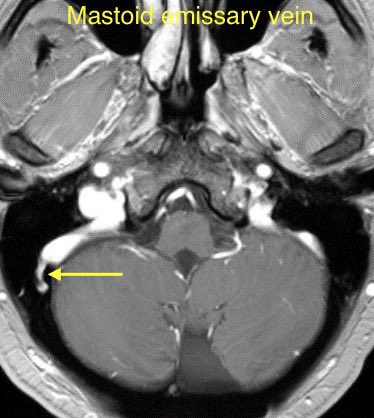
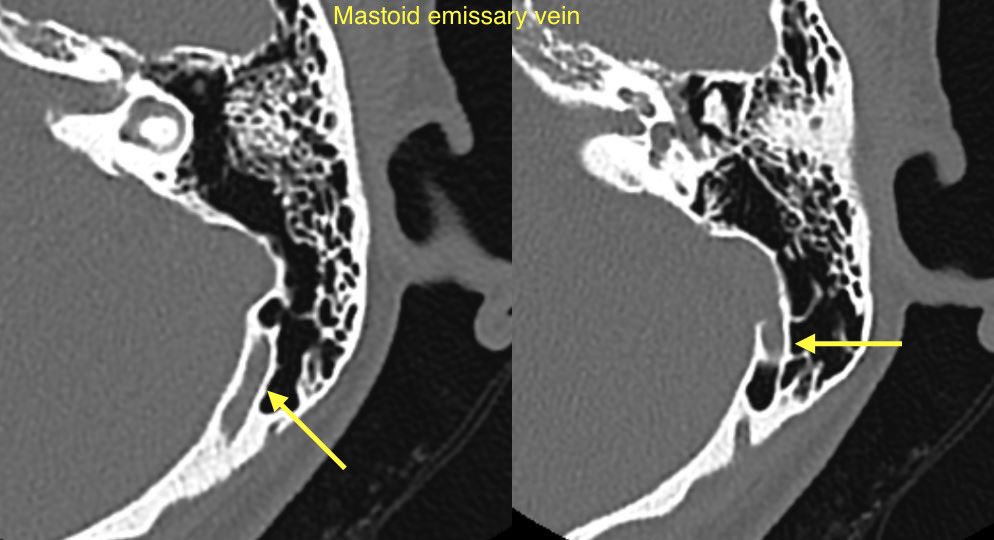
🔷EMISSARY VEIN ANOMALIES AND VARIANTS
1️⃣Mastoid emissary veins
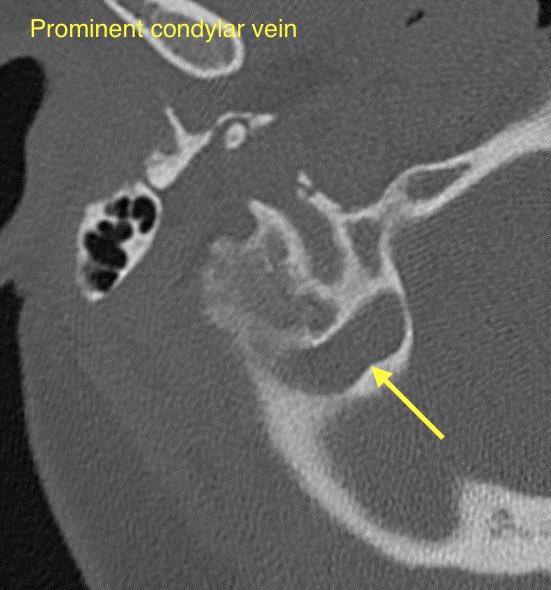
2️⃣Condylar veins
3️⃣Petrosquamosal emissary veins
1️⃣Mastoid emissary veins
2️⃣Condylar veins
3️⃣Petrosquamosal emissary veins
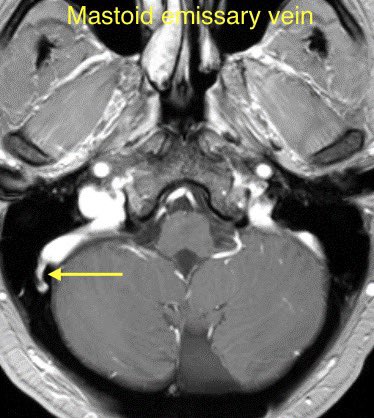
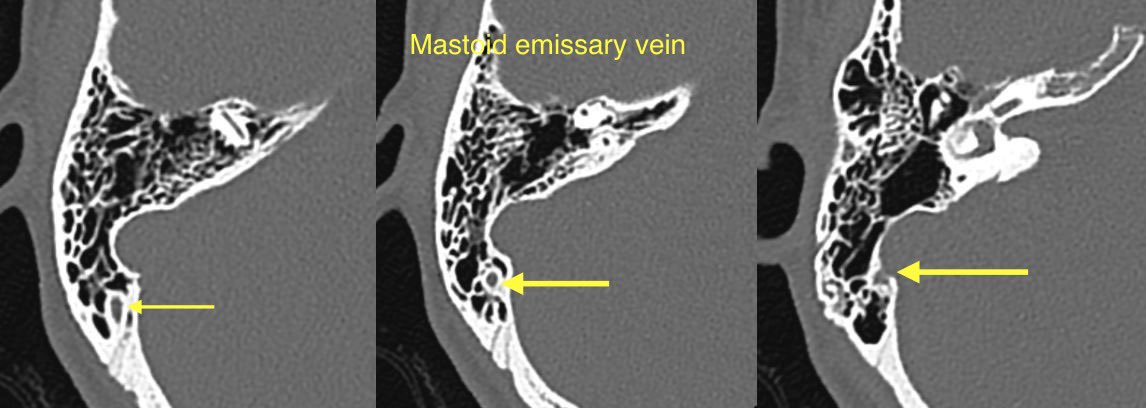
🔹Mastoid emissary veins (connect posterior auricular or occipital veins with the sigmoid sinus). These are common & usually incidental findings though have been associated with PT

🔹Condylar veins are anastomotic emissary veins that connect the distal sigmoid sinuses or proximal jugular veins with the suboccipital and deep cervical venous plexus
🔹These are often observed incidentally though have been associated with PT
🔹These are often observed incidentally though have been associated with PT

🔹Petrosquamosal emissary veins: (developmental venous variants) Look for them coursing along the upper aspect of the petrosquamosal suture
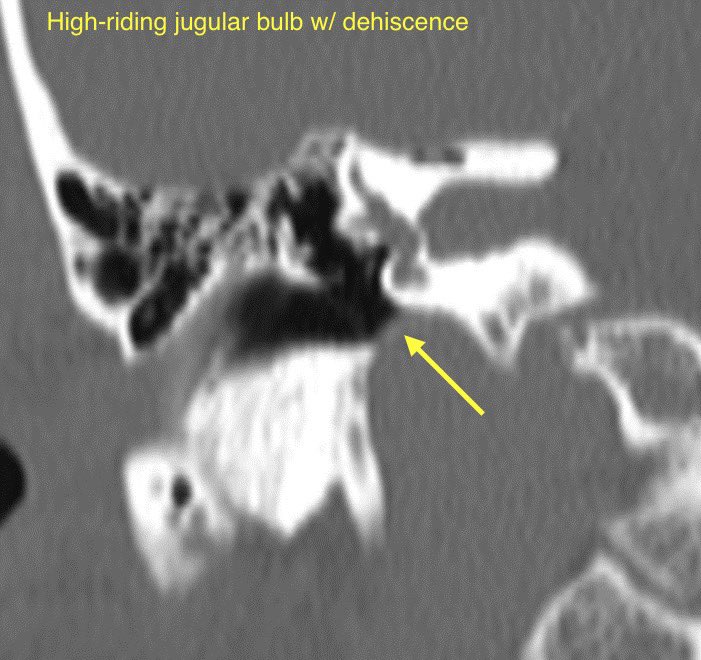
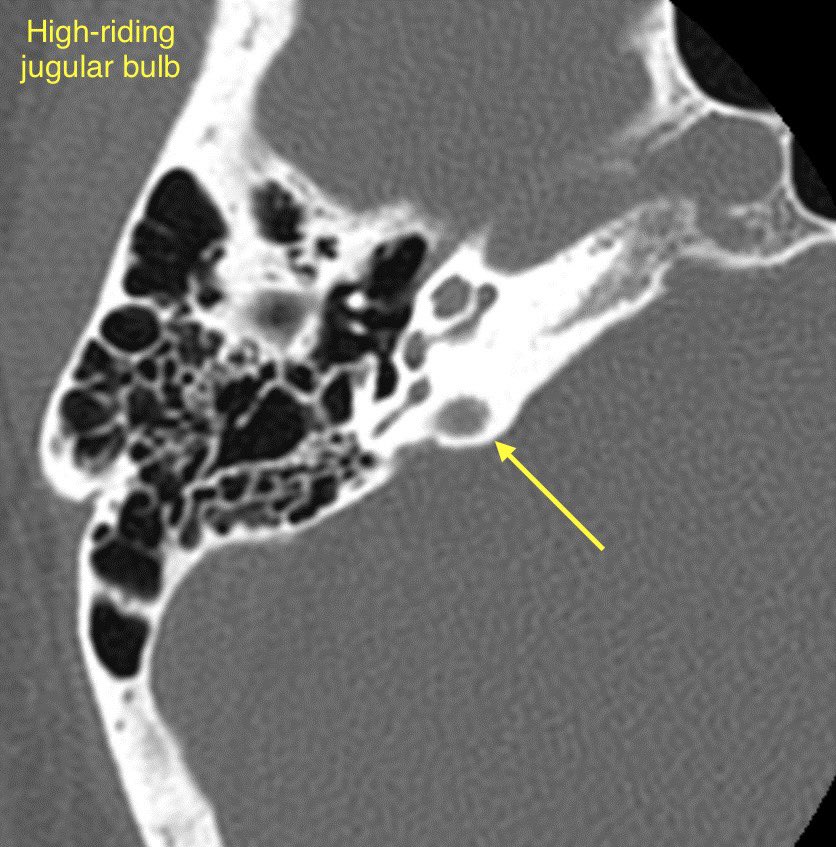
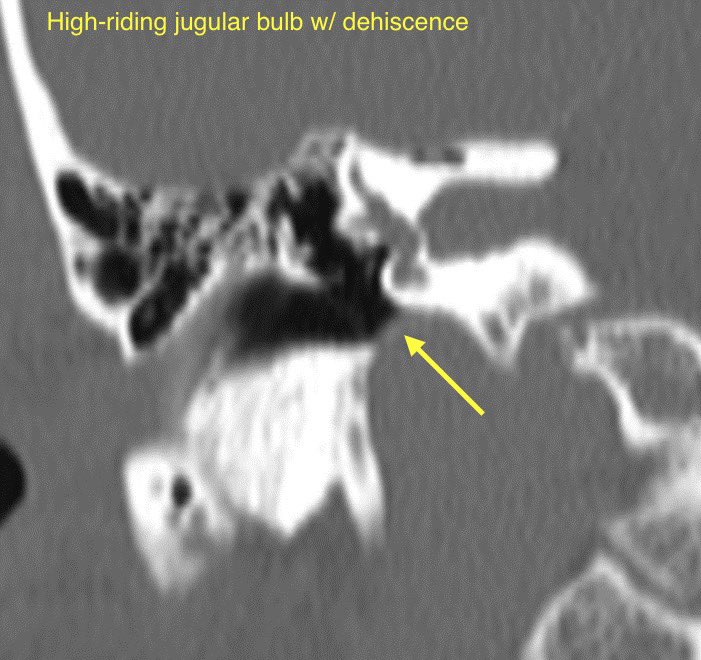
🔷JUGULAR BULB ABNORMALITIES
1️⃣High-riding jugular bulb
2️⃣Jugular bulb dehiscence
3️⃣Jugular bulb diverticulum
1️⃣High-riding jugular bulb
2️⃣Jugular bulb dehiscence
3️⃣Jugular bulb diverticulum
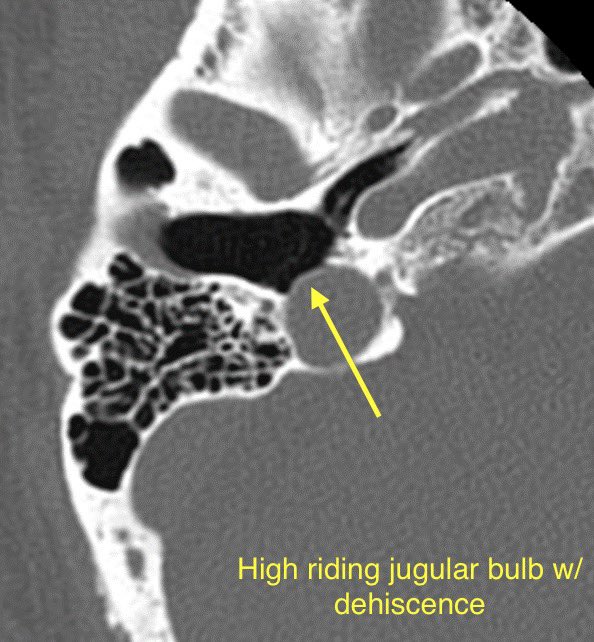
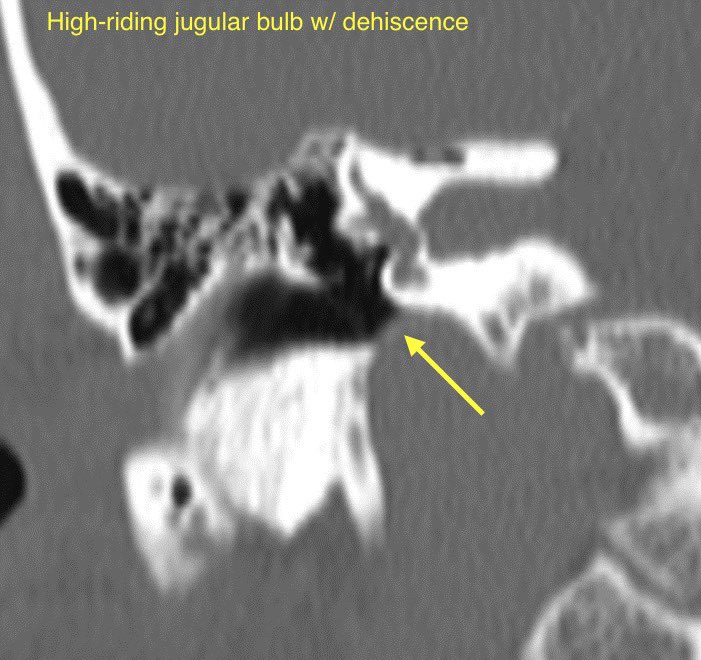
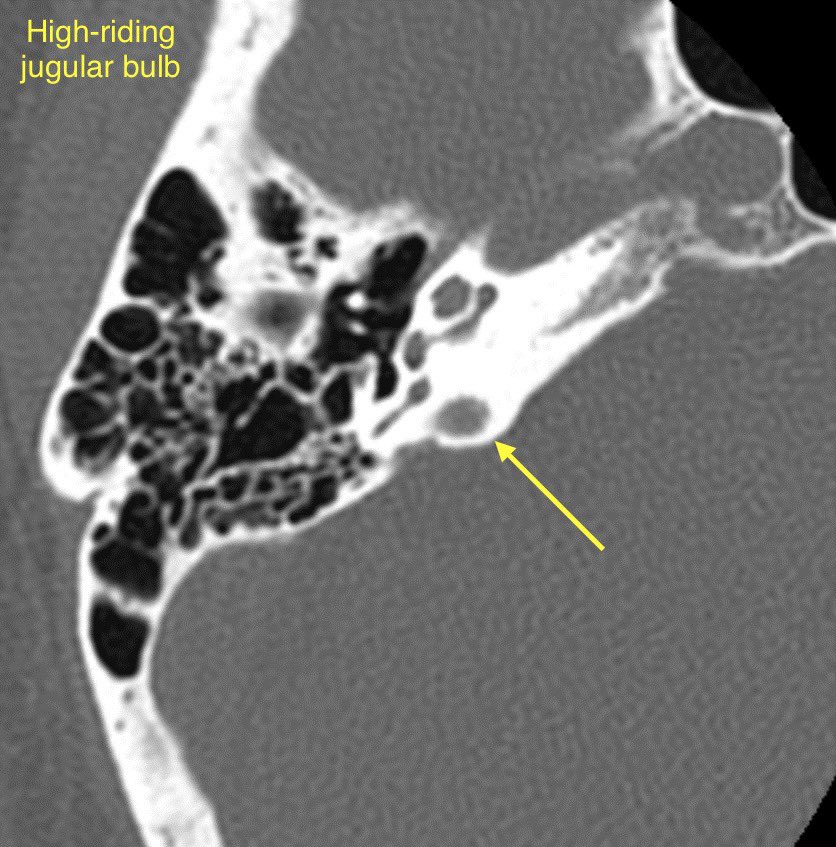
🔹High-riding jugular bulb is associated with jugular bulb dehiscence
💡"High" = within 2mm of the floor of the IAC, above the lower border of the round window, above the posterior semicircular canal, or above the basal turn of the cochlea
💡"High" = within 2mm of the floor of the IAC, above the lower border of the round window, above the posterior semicircular canal, or above the basal turn of the cochlea
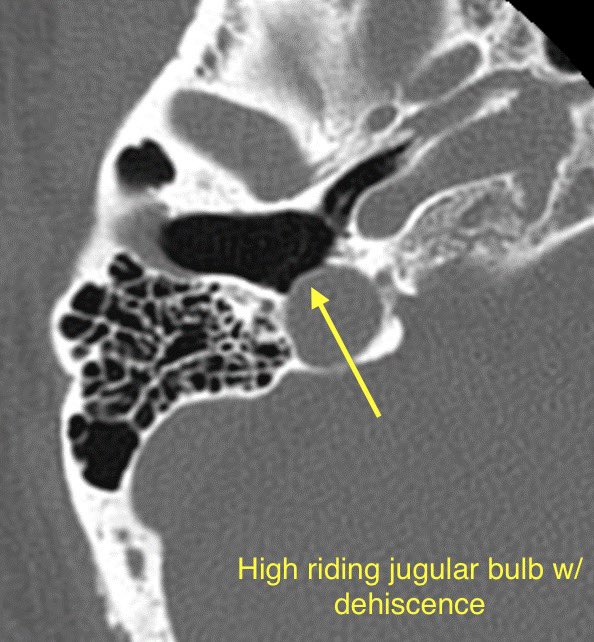
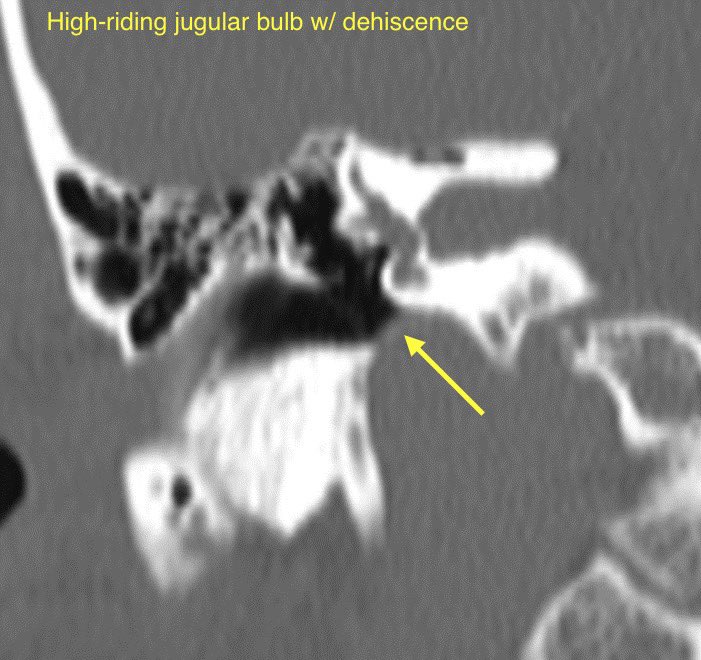
🔹Jugular bulb dehiscence: Thinning or visible defect of the jugular plate
🔹Jugular bulb diverticulum is a round outpouching arising from the jugular bulb and usually projects superomedially into the petrous bone
🔹Jugular bulb diverticulum is a round outpouching arising from the jugular bulb and usually projects superomedially into the petrous bone
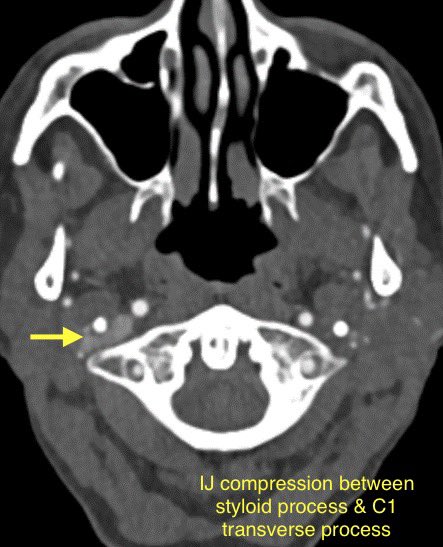
🔷OTHER CAUSES OF VENOUS PULSATILE TINNITUS
1️⃣Jugular vein outflow obstruction by the styloid process (common incidental finding in asymptomatic patients)
2️⃣Condylar vein diverticulum
3️⃣Prominent occipital sinus
4️⃣Occipital sinus stenosis
1️⃣Jugular vein outflow obstruction by the styloid process (common incidental finding in asymptomatic patients)
2️⃣Condylar vein diverticulum
3️⃣Prominent occipital sinus
4️⃣Occipital sinus stenosis
For more reading 📖
pubs.rsna.org
pubs.rsna.org
Loading suggestions...