


2/Purpose of mechanical thrombectomy is to save tissue that is still alive in the face of a large vessel occlusion
It’s like firefighters running into a burning building—they are only going to go in if someone is still alive to be rescued
Otherwise, it’s not worth the risk.
It’s like firefighters running into a burning building—they are only going to go in if someone is still alive to be rescued
Otherwise, it’s not worth the risk.

3/So it’s key in stroke to distinguish between unsalvageable tissue, called the core, and salvageable tissue, called the penumbra.
Saving penumbra is what prompts thrombectomy.
Going after core infarct is like running into a burning building with no survivors inside.
Saving penumbra is what prompts thrombectomy.
Going after core infarct is like running into a burning building with no survivors inside.

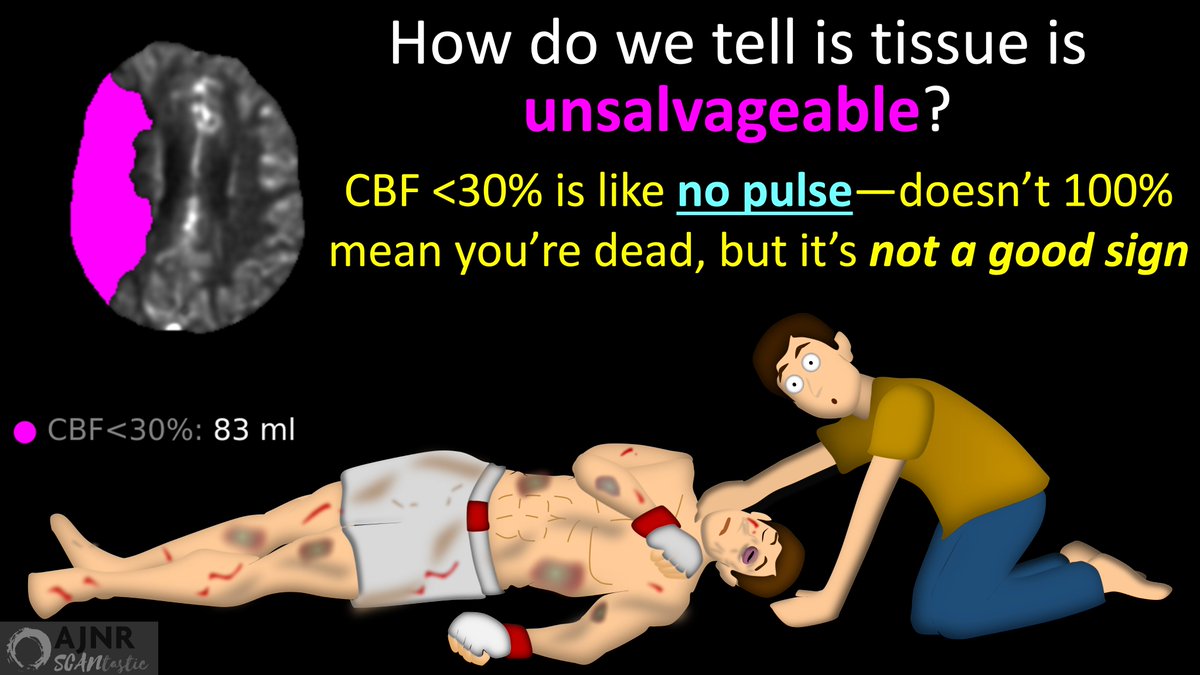
4/So how to determine what’s unsalvageable? How to know when to give up hope?
There must be a threshold
For thrombectomy it’s CBF < 30%
It’s like a threshold of no pulse—it doesn’t 100% mean you’re dead, but it’s a pretty strong indicator things will go that way.
There must be a threshold
For thrombectomy it’s CBF < 30%
It’s like a threshold of no pulse—it doesn’t 100% mean you’re dead, but it’s a pretty strong indicator things will go that way.
5/This threshold is VERY important
We don’t want to intervene if there is no hope of salvage
But you don’t want to accidentally misclassify tissue that has a chance of survival as core infarct.
You don’t want to leave someone in the burning building by mistake
We don’t want to intervene if there is no hope of salvage
But you don’t want to accidentally misclassify tissue that has a chance of survival as core infarct.
You don’t want to leave someone in the burning building by mistake

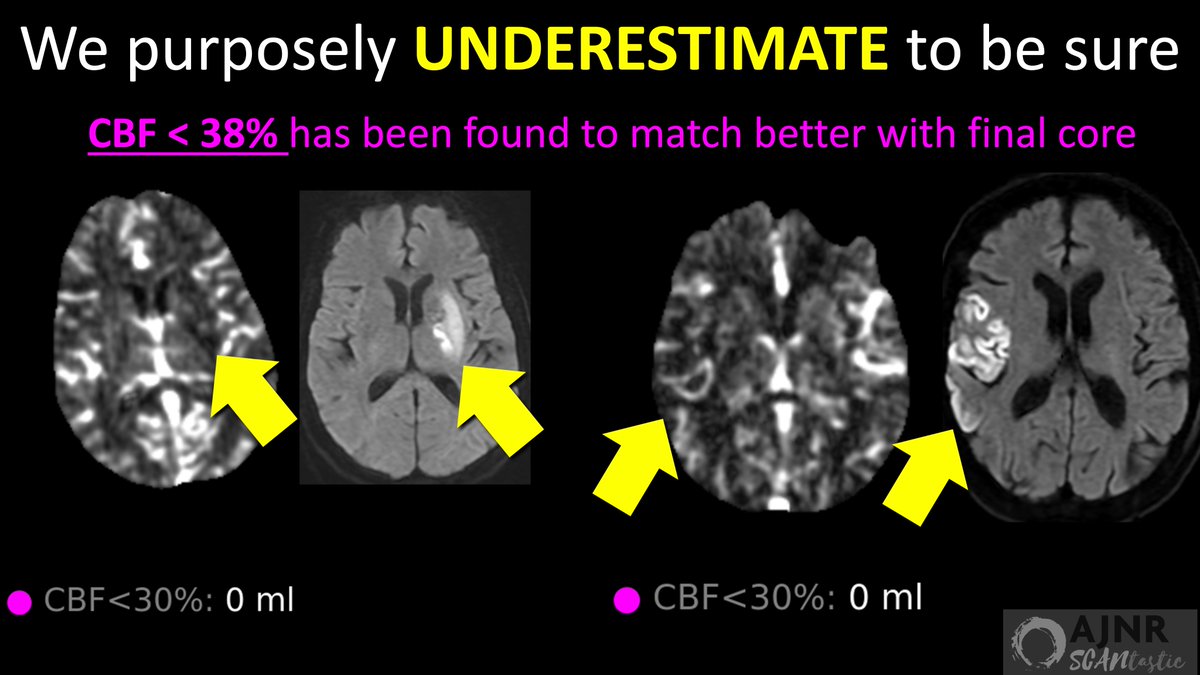
6/To avoid accidentally calling tissue unsalvageable that isn’t, we purposely underestimate the core
Data shows that CBF < 38% more accurately predicts the actual infarct size
But we made the threshold even harder to meet at <30%.
Why? Why would we want to be less accurate?
Data shows that CBF < 38% more accurately predicts the actual infarct size
But we made the threshold even harder to meet at <30%.
Why? Why would we want to be less accurate?
7/We’re less accurate & more conservative bc we want to make sure core is really core
It’s like going all-in in poker—you’re only doing it if you have a strong hand & probability of winning
For stroke, we want a strong hand or probability of being right bc we’re betting brain
It’s like going all-in in poker—you’re only doing it if you have a strong hand & probability of winning
For stroke, we want a strong hand or probability of being right bc we’re betting brain
8/It’s kind of like how your boss always underestimates how long it will take to complete a project.
If you overestimate the work, no one will sign on.
So you underestimate to help get people to help.
We underestimate to try to help any possible penumbra
If you overestimate the work, no one will sign on.
So you underestimate to help get people to help.
We underestimate to try to help any possible penumbra
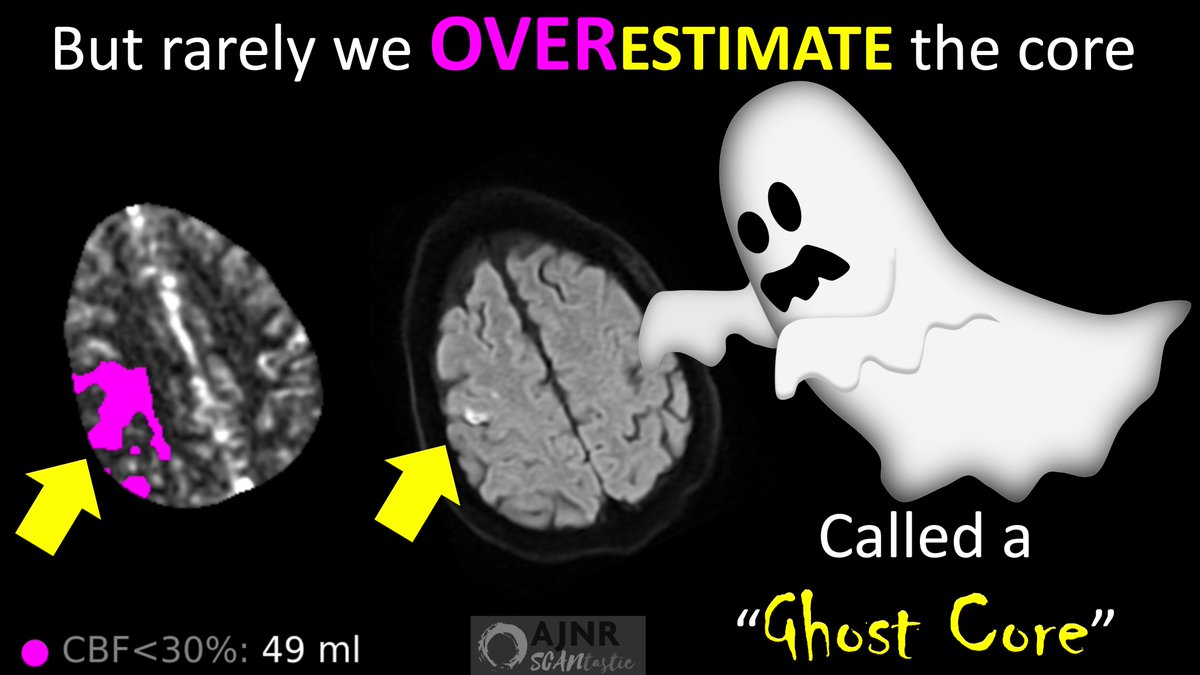
9/But occasionally, patients surprise us!
Rarely, we end up overestimating the core—saying tissue was unsalvageable when it actually was salvageable.
This is called a “Ghost Infarct Core” bc it was there on perfusion & vanished like a ghost on follow up MRI after thrombectomy.
Rarely, we end up overestimating the core—saying tissue was unsalvageable when it actually was salvageable.
This is called a “Ghost Infarct Core” bc it was there on perfusion & vanished like a ghost on follow up MRI after thrombectomy.
10/So what happened?
Weren’t we supposed to be underestimating the core w/our very conservative threshold?!
How did we end up overestimating it?!
Did endovascular end up raising up brain from the dead?!
Weren’t we supposed to be underestimating the core w/our very conservative threshold?!
How did we end up overestimating it?!
Did endovascular end up raising up brain from the dead?!
11/You must go back to the fact that our perfusion threshold is just a probability
It is like going in on a really good hand.
Usually you are going to win, but occasionally someone has a better hand & beats you
Occasionally, the brain beats the odds against it
It is like going in on a really good hand.
Usually you are going to win, but occasionally someone has a better hand & beats you
Occasionally, the brain beats the odds against it
12/So clearly, there must be favorable conditions.
Data shows that brain with CBF <30% overwhelming goes on to infarct.
So what conditions allows brain to survive despite having such low blood flow?
Data shows that brain with CBF <30% overwhelming goes on to infarct.
So what conditions allows brain to survive despite having such low blood flow?
13/In this month’s issue of AJNR, Ospel et al found that ghost cores occurred in about 10% of thrombectomy patients
They found 2 conditions helped the brain to overcome what prior data has shown to be dire conditions & come back, when it should be dead
They found 2 conditions helped the brain to overcome what prior data has shown to be dire conditions & come back, when it should be dead
14/First was younger age.
This makes sense. Ischemia is an insult to brain, like a punch is to the face.
Who will better recover from a punch to the face—you or your 90-year-old grandfather?
Younger brains have more capacity to survive under adverse conditions.
This makes sense. Ischemia is an insult to brain, like a punch is to the face.
Who will better recover from a punch to the face—you or your 90-year-old grandfather?
Younger brains have more capacity to survive under adverse conditions.
15/Second was shorter time from last known well.
This also makes sense. Depriving a brain of blood from an occlusion is like putting it in a chokehold
The shorter time you’re in a chokehold, the more likely you are to recover.
Shorter time at low perfusion helps.
This also makes sense. Depriving a brain of blood from an occlusion is like putting it in a chokehold
The shorter time you’re in a chokehold, the more likely you are to recover.
Shorter time at low perfusion helps.
16/Ghost cores were also associated w/better reperfusion after thrombectomy
Brain w/o blood is like being in a desert w/o water
If you’re dying of thirst in a desert, you won’t recover as well if you just get a small amount to drink vs flooding you w/all the water you want
Brain w/o blood is like being in a desert w/o water
If you’re dying of thirst in a desert, you won’t recover as well if you just get a small amount to drink vs flooding you w/all the water you want
17/Finally, ghost cores were associated w/better collateral status.
If a stroke is like the brain being in a chokehold, then having collaterals is like having friends there to help you get air.
If friends or collaterals help you to get oxygen faster, you do better.
If a stroke is like the brain being in a chokehold, then having collaterals is like having friends there to help you get air.
If friends or collaterals help you to get oxygen faster, you do better.
18/So remember thresholds are just probabilities!
Individual patients may have less core & more penumbra than you think especially if they:
1)are young
2)have short time from LKW
3)get better reperfusion
4)have good collaterals
Individual patients may have less core & more penumbra than you think especially if they:
1)are young
2)have short time from LKW
3)get better reperfusion
4)have good collaterals

Loading suggestions...