

Reviewing current evidence on #hyponatremia in #heartfailure together with our bright visiting fellow @GiulioMonde!
Tweetorial 👇
link.springer.com
Tweetorial 👇
link.springer.com
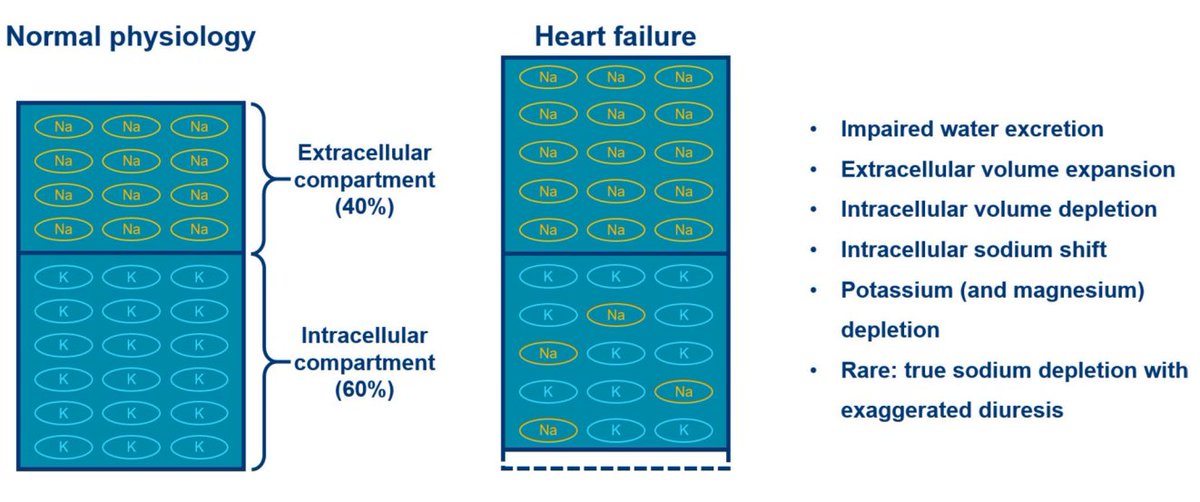
#hyponatremia in #heartfailure 🟰 mainly dilutional: ➡️Impaired water excretion & extracellular volume expansion!
However, we tend to underestimate the depletional component due to chronic potassium and magnesium losses
➡️Intracellular dehydration
➡️Intracellular sodium shift
However, we tend to underestimate the depletional component due to chronic potassium and magnesium losses
➡️Intracellular dehydration
➡️Intracellular sodium shift
Replenishing potassium & magnesium stores alone actually increases serum Na in depletional hyponatremia!
K & Mg go intracellular ➡️Na goes back extracellular
Best K level probably ~4.5 mmol/L
3.5-4.0 mmol/L: K deficit ~ 200 mmol (!), so be aggressive!
pubmed.ncbi.nlm.nih.gov
K & Mg go intracellular ➡️Na goes back extracellular
Best K level probably ~4.5 mmol/L
3.5-4.0 mmol/L: K deficit ~ 200 mmol (!), so be aggressive!
pubmed.ncbi.nlm.nih.gov

True Na depletion is very rare in #heartfailure unless there are extra-renal losses (e.g. gastro-intestinal)...
➡️Sodium avidity early on in heart failure (onlinelibrary.wiley.com)
➡️Interstitial sodium buffers full of Na
(sciencedirect.com)
➡️Sodium avidity early on in heart failure (onlinelibrary.wiley.com)
➡️Interstitial sodium buffers full of Na
(sciencedirect.com)

sciencedirect.com/science/articl…
The Pathophysiological Role of Interstitial Sodium in Heart Failure
The current understanding of heart failure (HF) does not fully explain the spectrum of HF symptoms....

onlinelibrary.wiley.com/doi/10.1002/ej…
The kidney in congestive heart failure: ‘are natriuresis, sodium, and diuretics really the good, the bad and the ugly?’
European Journal of Heart Failure is an ESC journal dedicated to improving the understanding, preven...
Urine dilution is dependent on 3 processes:
1. NCC & ENaC activity in distal nephron to reabsorb salt
2. Impermeability of distal nephron for water
3. Adequate flux through distal nephron
1. NCC & ENaC activity in distal nephron to reabsorb salt
2. Impermeability of distal nephron for water
3. Adequate flux through distal nephron
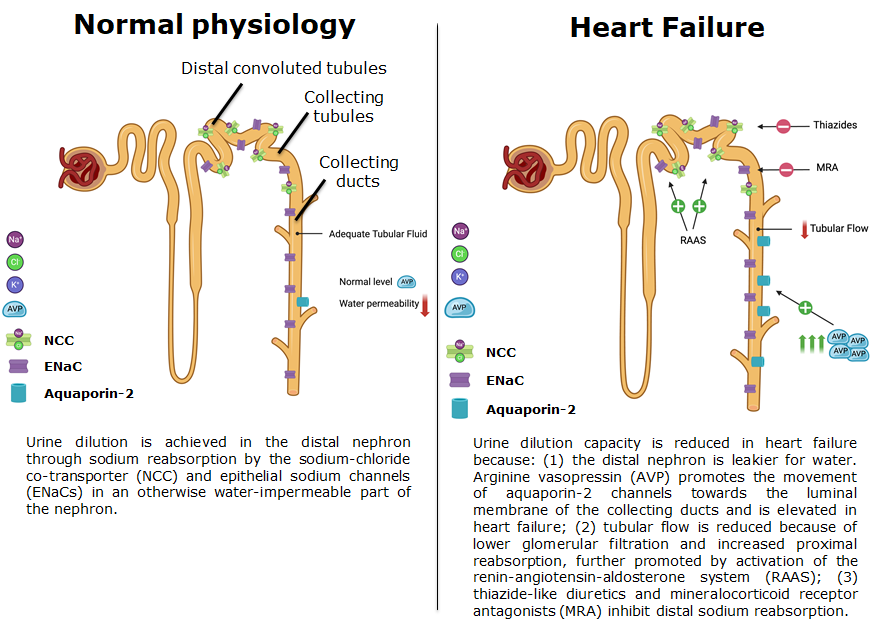
1. explains why #MRA, ENaC blockers (e.g. amiloride) & #thiazides facilitate hyponatremia development
➡️rarely main reason, 2. & 3. more important!
2. Distal nephron in #heartfailure = leakier because of 🔼AVP
➡️best R/ 🟰 neurohormonal blockers (GDMT!)
➡️rarely main reason, 2. & 3. more important!
2. Distal nephron in #heartfailure = leakier because of 🔼AVP
➡️best R/ 🟰 neurohormonal blockers (GDMT!)
By far the most important reason for #hyponatremia in #heartfailure is poor distal nephron flux !!!
➡️Improve nephron flow (hemodynamics!)
➡️Use powerful proximal diuretics to increase distal flow (#acetazolamide)
➡️AVP antagonists almost never needed!
sciencedirect.com
➡️Improve nephron flow (hemodynamics!)
➡️Use powerful proximal diuretics to increase distal flow (#acetazolamide)
➡️AVP antagonists almost never needed!
sciencedirect.com

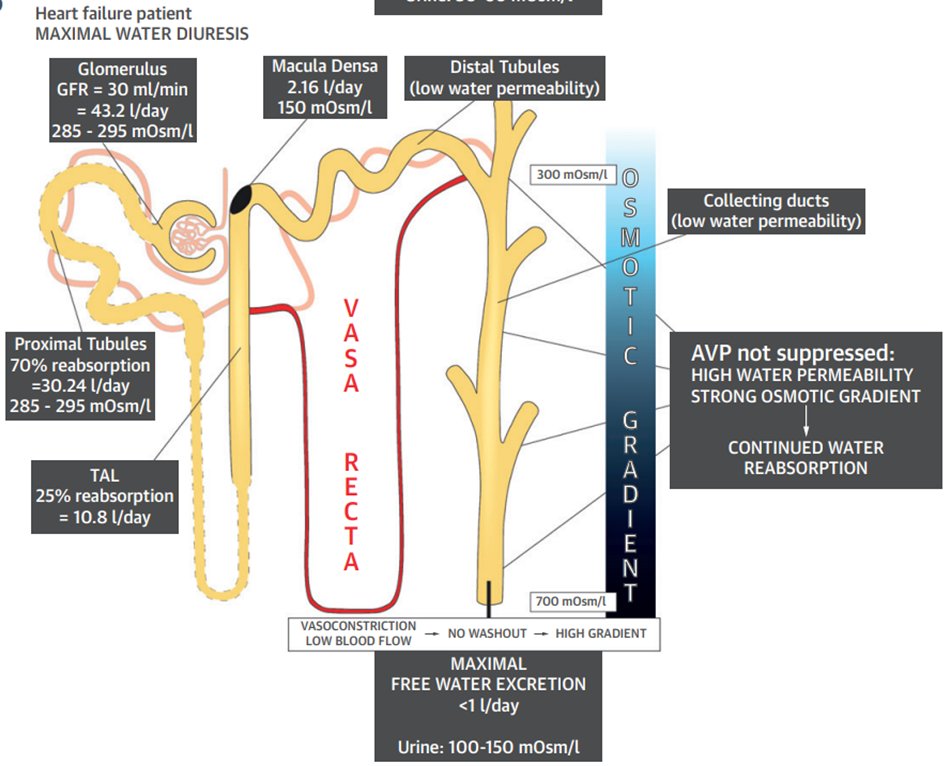
With a GFR of 30 mL/min/1.73m² & 70% proximal reabsorption (not uncommon in heart failure)
➡️Distal nephron flux as low as 2L (normally 18 L!!!)
➡️Shows how ineffective fluid restriction is in these cases, instead bring more tubular fluid distal (#acetazolamide!)
➡️Distal nephron flux as low as 2L (normally 18 L!!!)
➡️Shows how ineffective fluid restriction is in these cases, instead bring more tubular fluid distal (#acetazolamide!)
So how do we practically approach this problem?
1. Confirm that there is true hypotonic hyponatremia (Plasma osmolality <275 mOsm/L)
➡️Good history taking & clinical exam
➡️Key lab tests
1. Confirm that there is true hypotonic hyponatremia (Plasma osmolality <275 mOsm/L)
➡️Good history taking & clinical exam
➡️Key lab tests

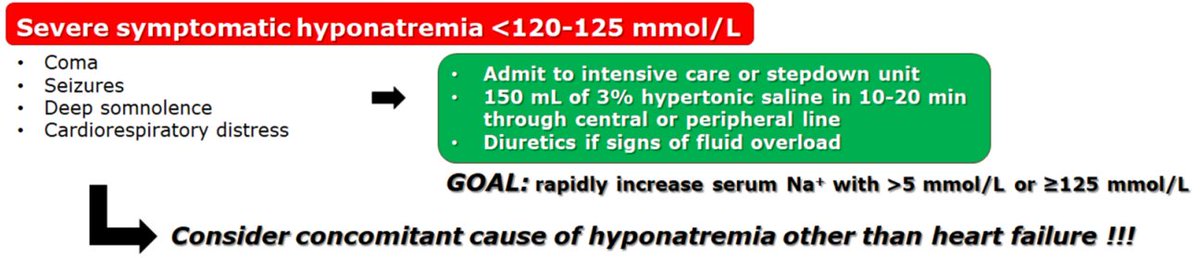
2. Evaluate whether hyponatremia is severe & symptomatic
➡️Only indication where you truly need #hypertonicsaline!
Remember: very unusual for #heartfailure to be to sole cause of severe hyponatremia <120 mmol/L!
➡️Only indication where you truly need #hypertonicsaline!
Remember: very unusual for #heartfailure to be to sole cause of severe hyponatremia <120 mmol/L!
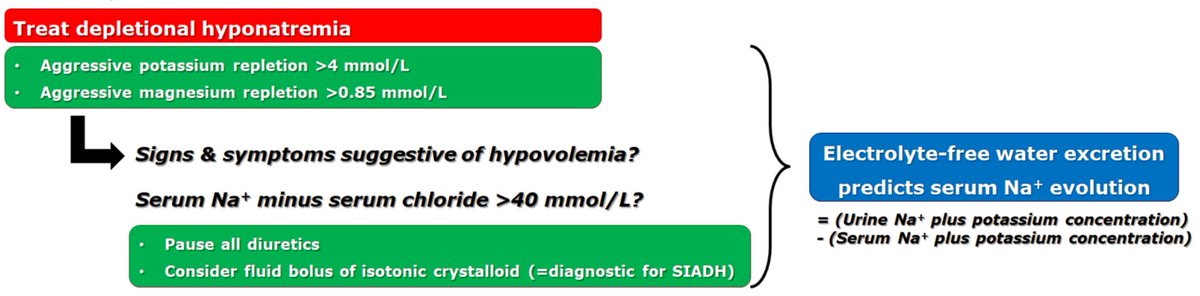
3. Treat the depletional component of hyponatremia
➡️Mainly K & Mg: be aggressive !!!
➡️If chloride depletion ([Na+]-[Cl-]>40 mmol/L), need to replete as well, suggests "true" salt depletion
Tip: KCl is your best friend in depletional #hyponatremia!
➡️Mainly K & Mg: be aggressive !!!
➡️If chloride depletion ([Na+]-[Cl-]>40 mmol/L), need to replete as well, suggests "true" salt depletion
Tip: KCl is your best friend in depletional #hyponatremia!
4. Finally, tackle the dilutional component of hyponatremia:
➡️First focus on hemodynamics: restore low output (#vasodilatorswork)
➡️GDMT (in particular start/uptitrate #SGLT2i & renin-angiotensin blockers
➡️Fluid restriction may help, but rarely a gamechanger!
➡️Diuretics!!!
➡️First focus on hemodynamics: restore low output (#vasodilatorswork)
➡️GDMT (in particular start/uptitrate #SGLT2i & renin-angiotensin blockers
➡️Fluid restriction may help, but rarely a gamechanger!
➡️Diuretics!!!
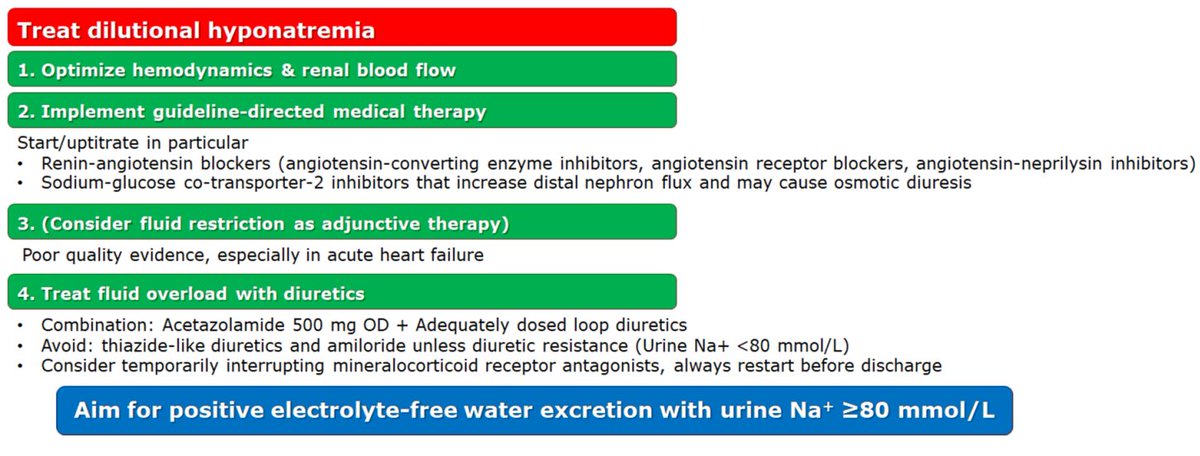
#Diuretics in #hyponatremia:
1. Backbone: Acetazolamide & adequately dosed loop diuretics
2. Avoid #thiazides, BUT sometimes needed for adequate diuretic response
3. UNa makes your life easy! Aim for positive electrolyte-free water excretion!
Target UNa
>80 mmol/L
<plasma [Na+]
1. Backbone: Acetazolamide & adequately dosed loop diuretics
2. Avoid #thiazides, BUT sometimes needed for adequate diuretic response
3. UNa makes your life easy! Aim for positive electrolyte-free water excretion!
Target UNa
>80 mmol/L
<plasma [Na+]
Don't forget to calculate potassium in your electrolyte-free water equation, thus more accurate:
UNa + UK schould be < [Na+]plasma + [K]plasma
Who can say electrolytes are not fun!
UNa + UK schould be < [Na+]plasma + [K]plasma
Who can say electrolytes are not fun!

Loading suggestions...