

Quick, basic primer🧵- Decompressing a tension pneumothorax
A tension pneumothorax is a life-threatening emergency which will lead to death without immediate intervention. Understanding and recognizing one is vital to time dependent intervention.
(1/n)
A tension pneumothorax is a life-threatening emergency which will lead to death without immediate intervention. Understanding and recognizing one is vital to time dependent intervention.
(1/n)

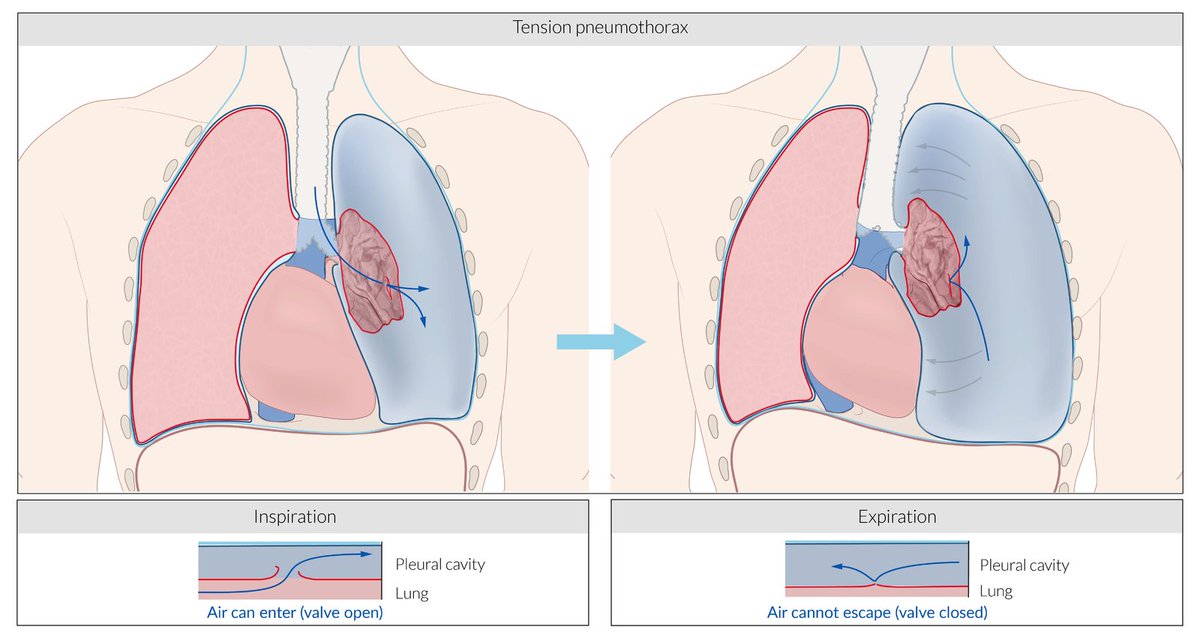
Patho-physiology of a closed pneumothorax is discussed here: which occurs when air accumulates between parietal & viscera layers of pleura- usually from a defect in the integrity of lung-pleural interface causing air to leak from alveoli into the pleural space.


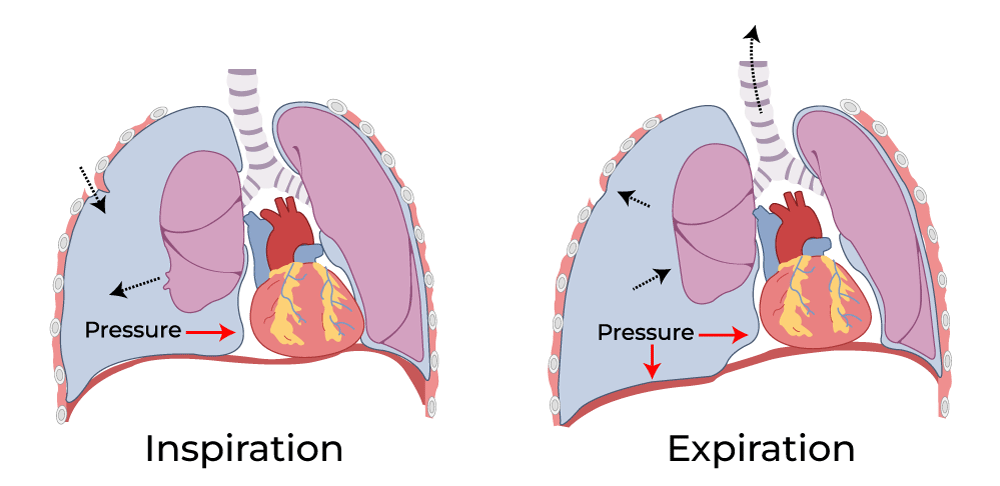
Air accumulates over time within the pleural cavity as the leak continues, due to negative pressure gradient caused by chest wall expansion during inspiration.
Eventually, pressure caused by the pneumothorax begins to compress and collapse the spongy & elastic lung parenchyma.
Eventually, pressure caused by the pneumothorax begins to compress and collapse the spongy & elastic lung parenchyma.

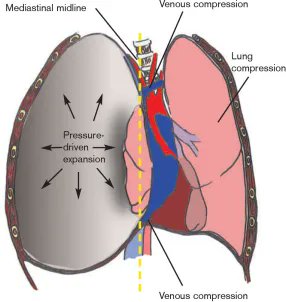
With each further breath (or when positive pressure ventilation in administered) the air volume + pressure progressively builds within the pleura, causing the pneumothorax to further expand.
This compresses other intrathoracic structures and causing the mediastinum to "shift".
This compresses other intrathoracic structures and causing the mediastinum to "shift".
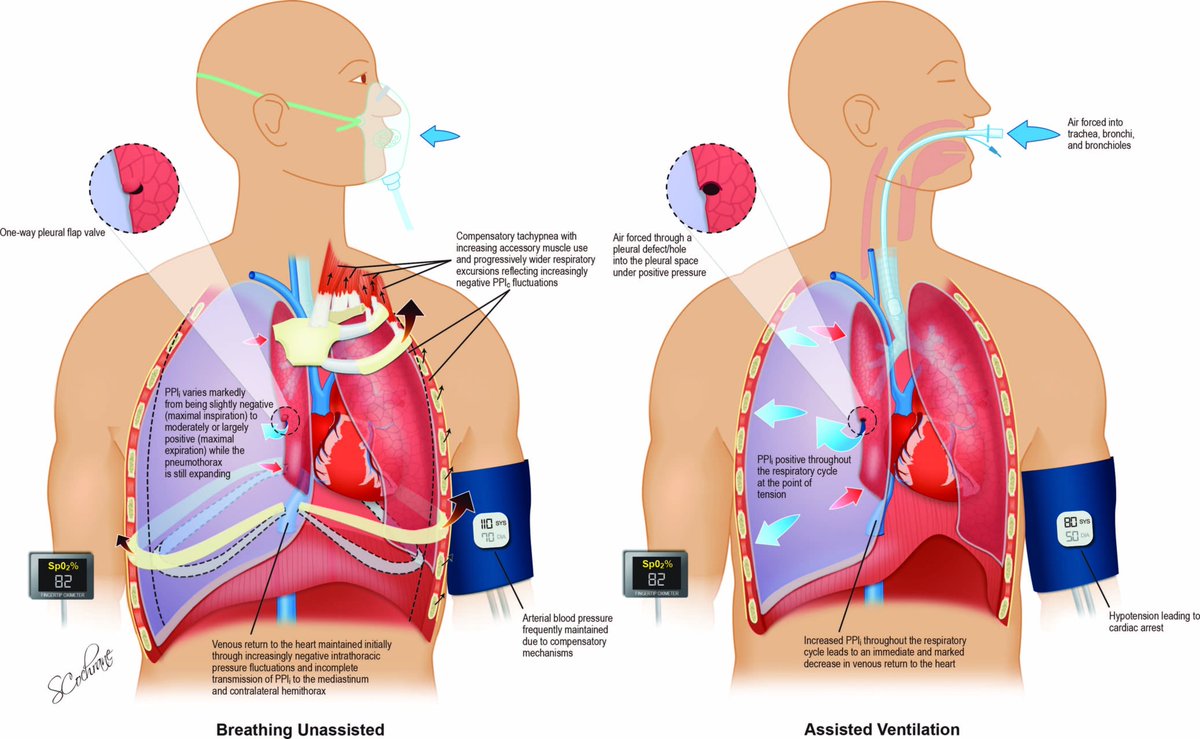
Positive pressure ventilation when used to provide respiratory support for critically ill patients causes increased thoracic pressure throughout the respiratory cycle.
This may lead to sudden increase in intrathoracic pressures and shock due to absent compensatory mechanisms.
This may lead to sudden increase in intrathoracic pressures and shock due to absent compensatory mechanisms.
This now leads to "tension physiology":
1. Respiratory compromise due to initial ipsilateral lung collapse and subsequent contra lateral lung compression impairing ventilation and consequentially oxygenation.
1. Respiratory compromise due to initial ipsilateral lung collapse and subsequent contra lateral lung compression impairing ventilation and consequentially oxygenation.
2. Increased intrathoracic pressure on the low pressure vena caval system leads to reduced venous return to the right side of the heart.
This in-turn leads to reduced cardiac output and hypotension from the obstructive shock, and eventually cardiac arrest.
This in-turn leads to reduced cardiac output and hypotension from the obstructive shock, and eventually cardiac arrest.
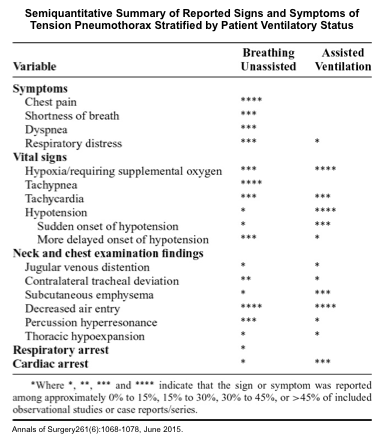
Early clinical signs to detect a pneumothorax:
1. Chest pain
2. Resp distress, tachypnea and mild hypoxia
3. Ipsilateral reduced chest expansion
4. Ipsilateral decreased breath sounds
5. Ipsilateral increased percussion note
6. Distended neck veins
7. Subcutaneous emphysema
1. Chest pain
2. Resp distress, tachypnea and mild hypoxia
3. Ipsilateral reduced chest expansion
4. Ipsilateral decreased breath sounds
5. Ipsilateral increased percussion note
6. Distended neck veins
7. Subcutaneous emphysema
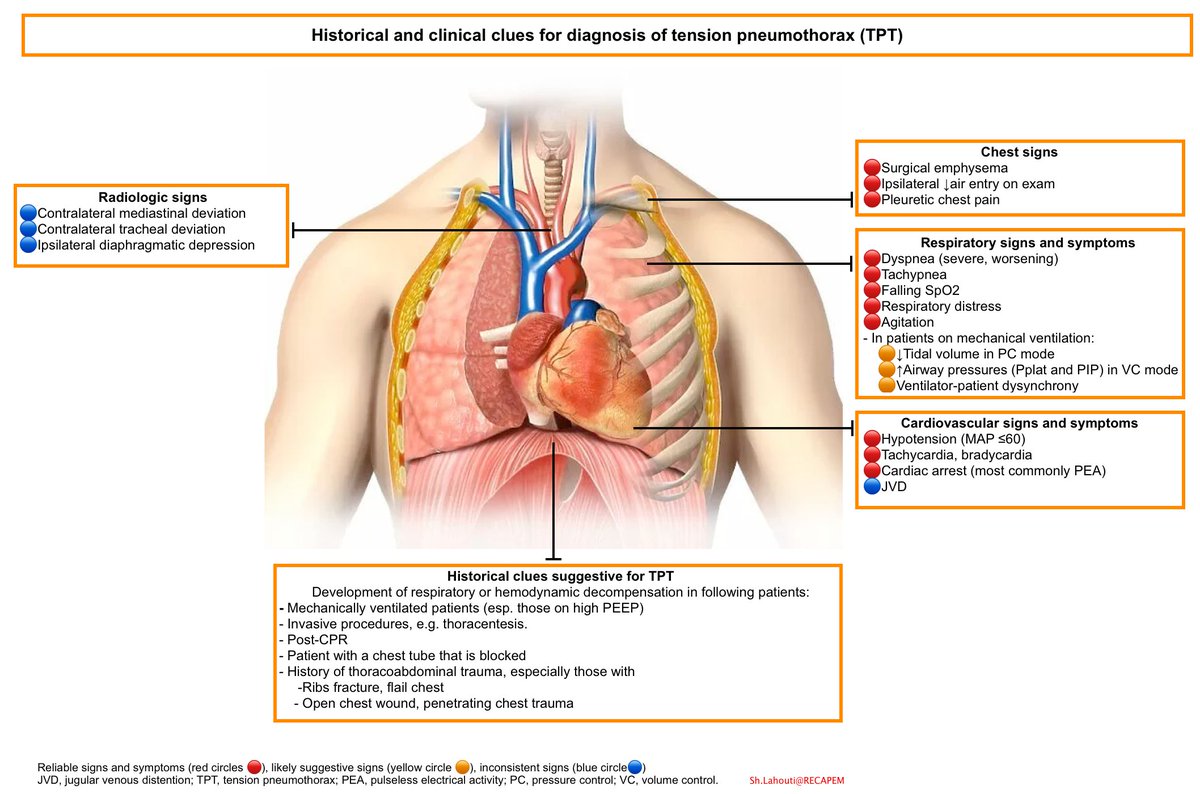
Signs of tension pneumothorax:
1. Profound hypoxia + cyanosis
2. Ipsilateral absent chest expansion, bulging
3. Ipsilateral absent breath sounds & reduced contralaterally
4. Bulging neck veins
5. Hypotension, particularly on inspiration
6. Pulsus paradoxus, electrical alternans
1. Profound hypoxia + cyanosis
2. Ipsilateral absent chest expansion, bulging
3. Ipsilateral absent breath sounds & reduced contralaterally
4. Bulging neck veins
5. Hypotension, particularly on inspiration
6. Pulsus paradoxus, electrical alternans
Confirmation: Tension pneumothorax is a CLINICAL diagnosis!!!
Confirm with #POCUS signs of a pneumothorax if available at the bedside. Undue delays to obtain X-ray or CT imaging MUST NOT delay your intervention, as progression may cause your patient to further deteriorate.
Confirm with #POCUS signs of a pneumothorax if available at the bedside. Undue delays to obtain X-ray or CT imaging MUST NOT delay your intervention, as progression may cause your patient to further deteriorate.

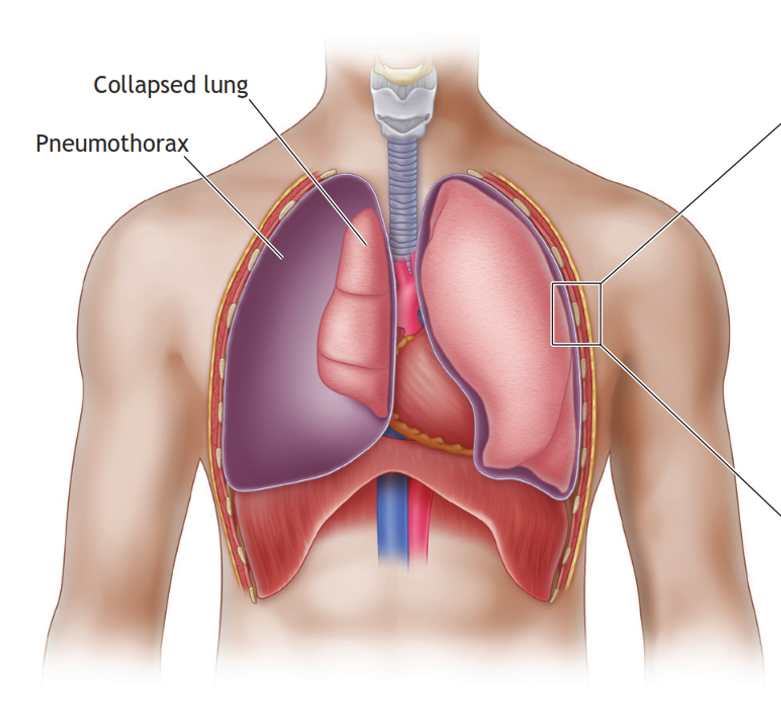
The aim of the immediate life-saving intervention is to decompress the pleura, reduce the intrathoracic pressure, thus relieving the "tension pathophysiology".
This in essence is trying to convert a tension pneumothorax (Lt panel) to a simple pneumothorax (Rt panel).
This in essence is trying to convert a tension pneumothorax (Lt panel) to a simple pneumothorax (Rt panel).

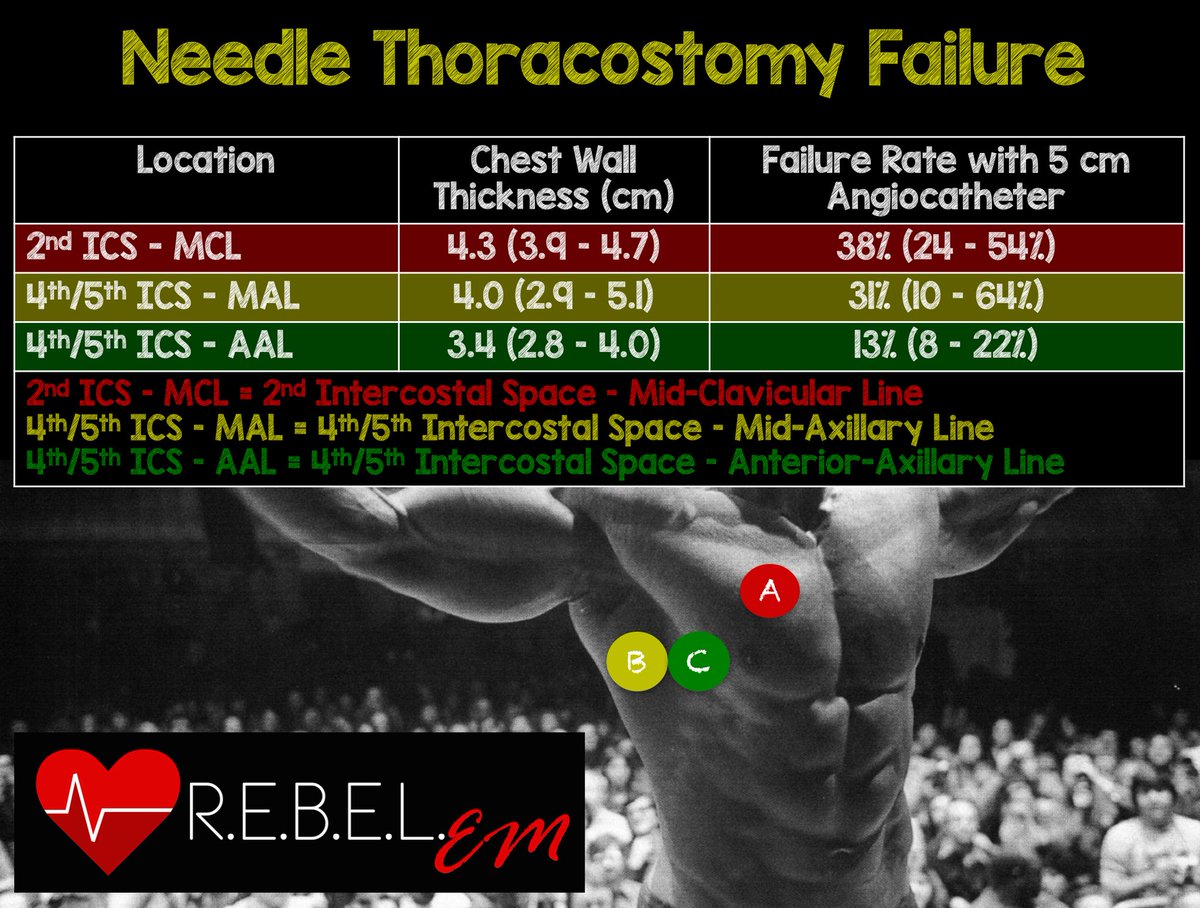
Needle thoracostomy via the anterior chest (2nd ICS along mid clavicular line) maybe the quickest approach. It has it's limitations - Risk of failure in thick chest wall or if needle isn't long enough.
The lateral wall (4th-5th ICS) is an alternate site for needle decompression.
The lateral wall (4th-5th ICS) is an alternate site for needle decompression.
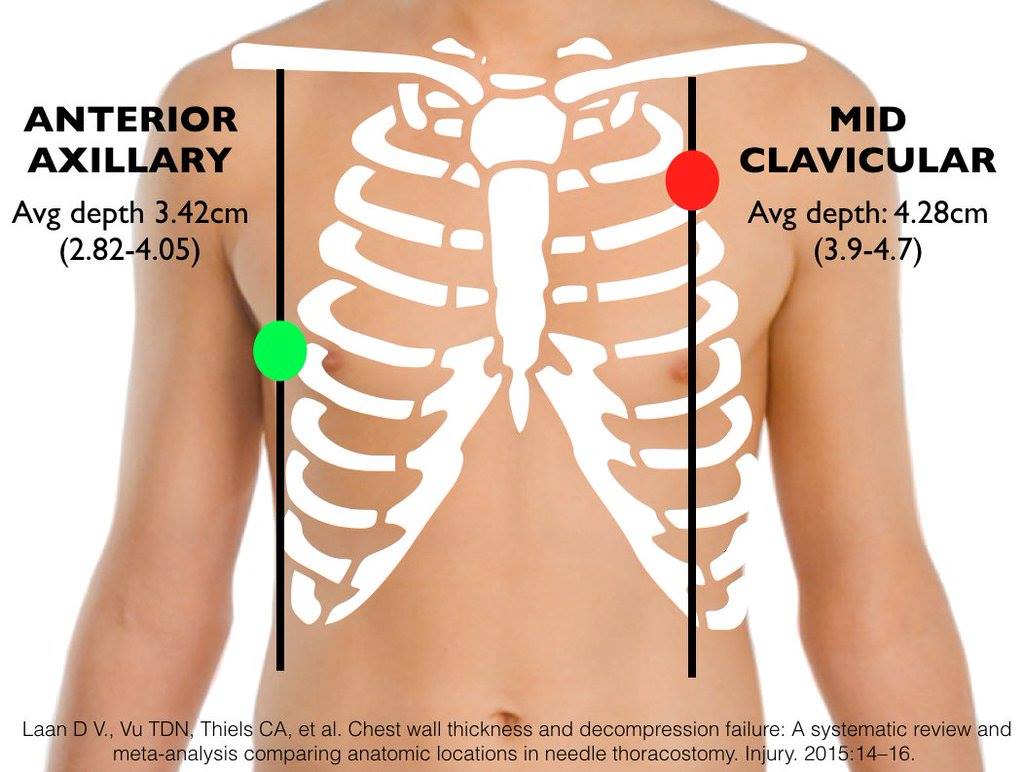
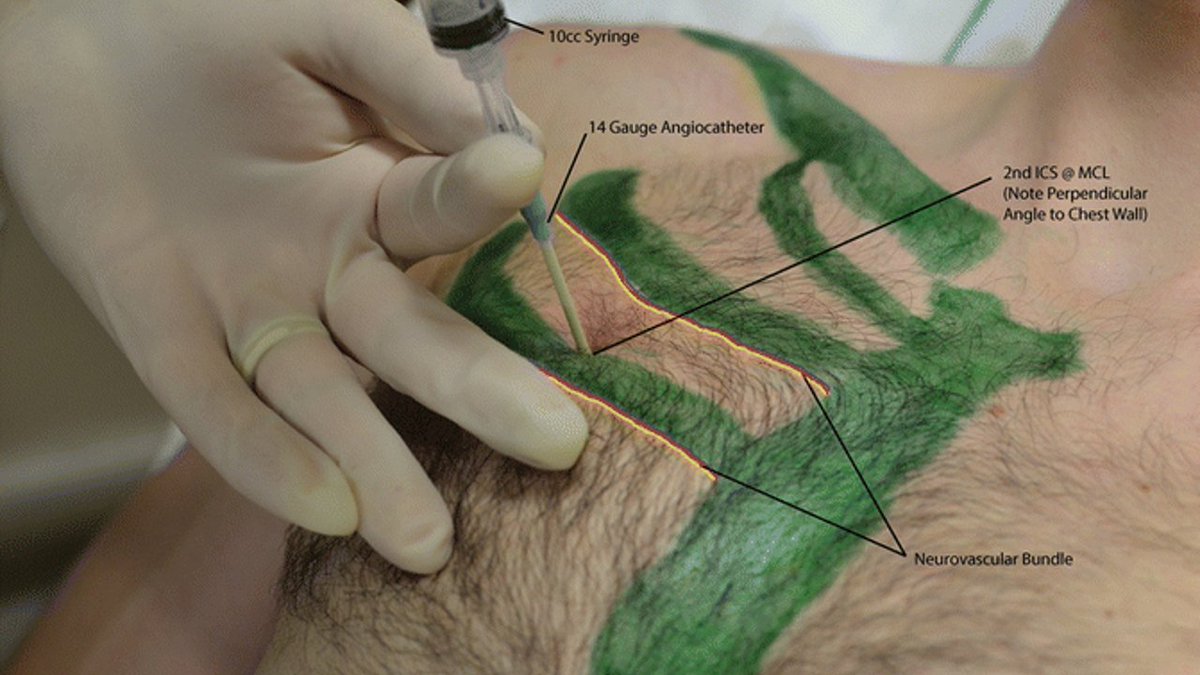
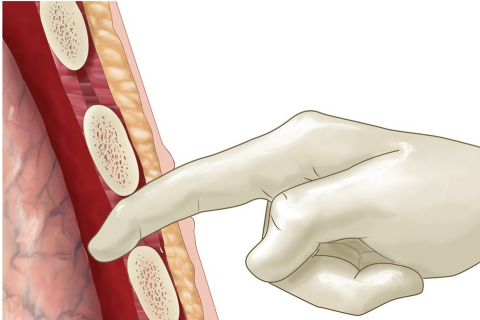
Quick prep the skin. Go in vertically, perpendicular to the skin above upper border of the inferior rib with a wide bore cannula or an angiocath, aspirating for air once skin is passed. Once free air aspirated, remove the needle to allow air to 💨
Water seal is NOT necessary.
Water seal is NOT necessary.
Drain until air stops gushing out - this, combined with improvement in haemodynamics suggests adequate decompression.
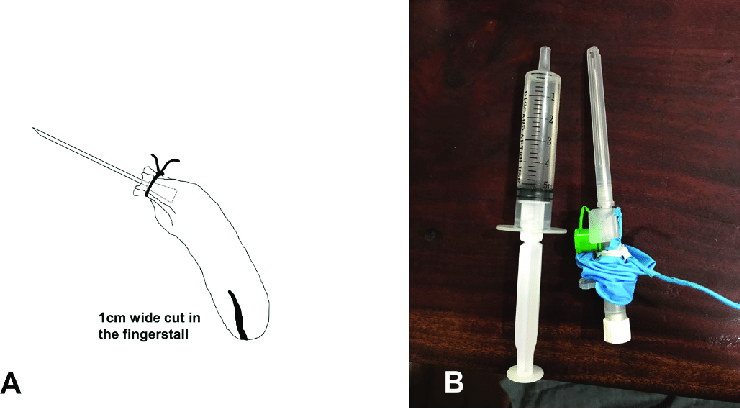
Few ml of sterile water in the syringe as an indicator (not intended as a water seal) shows when the air stops gushing; and if it enters the pleura- no problemo.
Few ml of sterile water in the syringe as an indicator (not intended as a water seal) shows when the air stops gushing; and if it enters the pleura- no problemo.

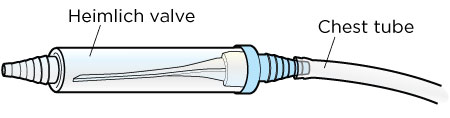
Other methods of ensuring that the device introduced does not become a conduit for atmospheric air to get sucked into the pleura once negative thoracic pressure is attained is to connect it to a one-way valve.
An improvised Heimlich valve may be fashioned using a glove finger.
An improvised Heimlich valve may be fashioned using a glove finger.
A method preferred to needle compression in combat scenarios & currently recommended by ATLS is lateral wall finger thoracostomy.
This can be used even in individuals with bulky or muscular chest walls and has the advantage of not interfering with chest compressions during CPR.
This can be used even in individuals with bulky or muscular chest walls and has the advantage of not interfering with chest compressions during CPR.


The finger thoracostomy is more invasive and technical, however has higher rates of success, and attains faster decompression. Also, upon completion of the procedure it allows to proceed with the insertion of a chest drain tube for definitive management of the pneumothorax.
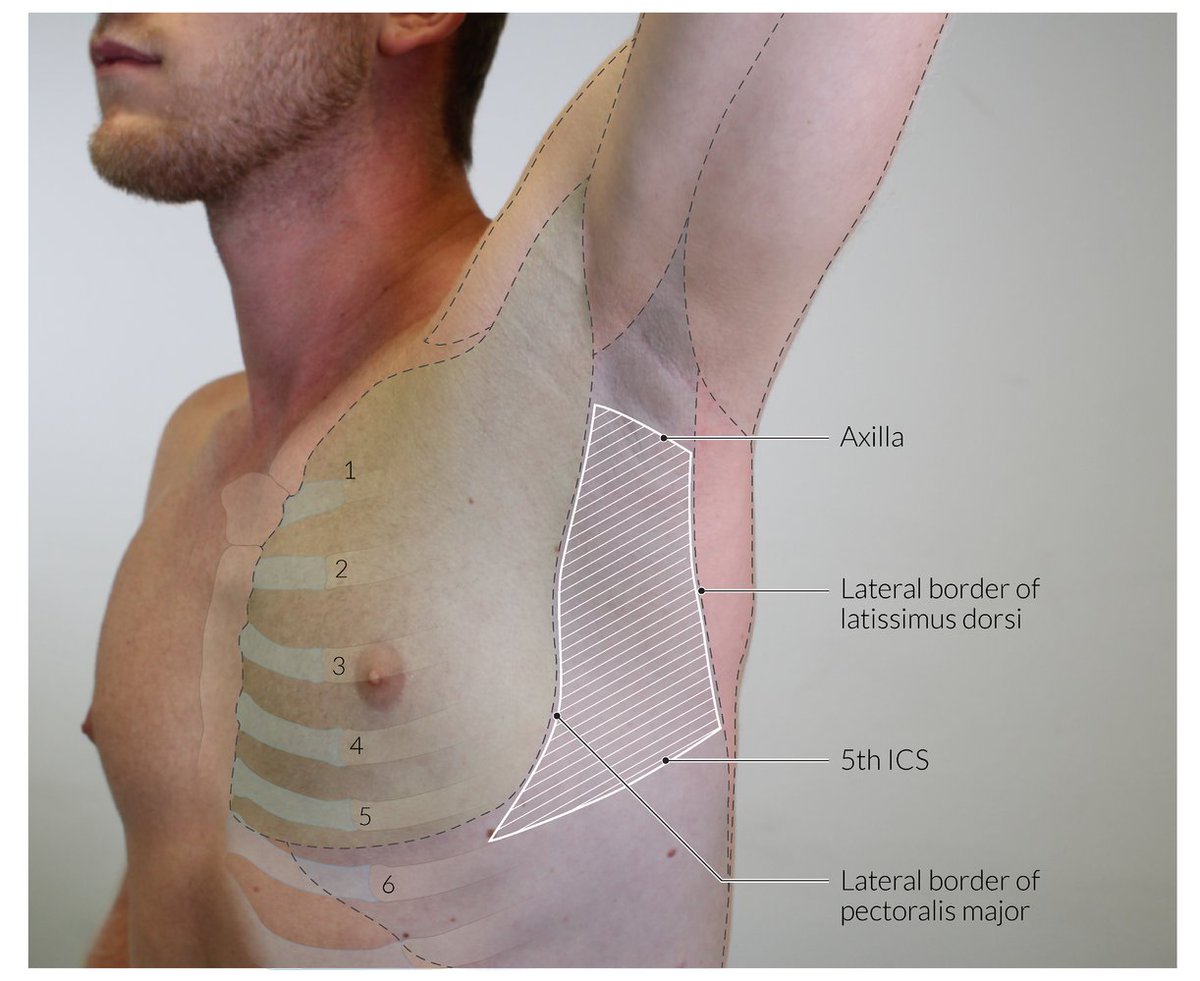
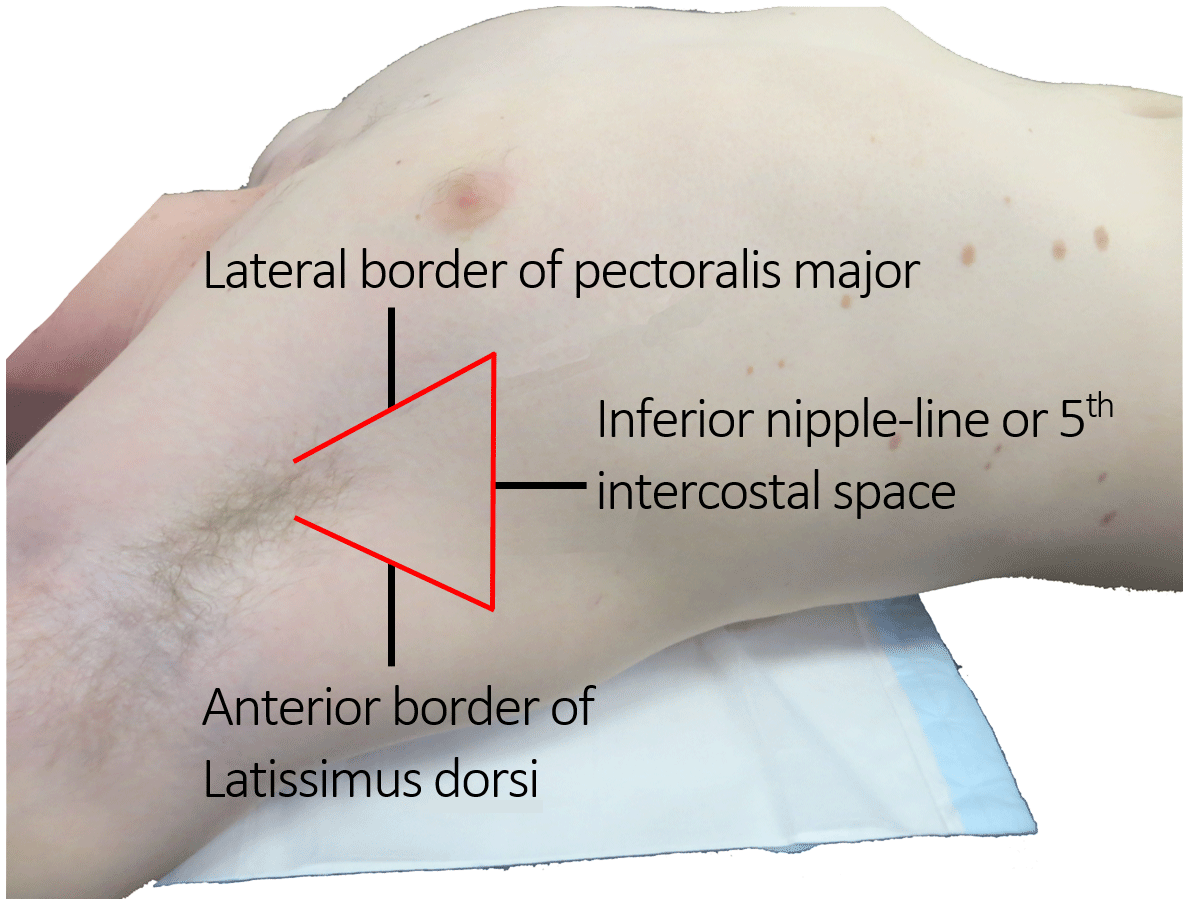
Incision parallel to the 5th rib is made on the lateral chest wall in the "Triangle of safety", and blunt dissection of a tract is performed with a closed forceps.
The pleural is entered and a gloved finger is introduced into the space and air drained.
clinical.stjohnwa.com.au
The pleural is entered and a gloved finger is introduced into the space and air drained.
clinical.stjohnwa.com.au

⚠️Important: Essential to follow up either a needle thoracostomy or a finger thoracostomy with definitive management - a chest tube or a catheter via either surgical or Seldinger technique, with a water seal.
Failure to do so may result in re-accumulation of tension pneumothorax.
Failure to do so may result in re-accumulation of tension pneumothorax.

TL;DR
◾️Tension pneumothorax is a progressive pathology
◾️Life threatening as it worsens
◾️Diagnosed clinically
◾️Requires emergency decompression:
◾️Needle & finger thoracostomy are options
◾️Follow-up with tube thoracostomy for definitive treatment
End/🧵
Image credits in ALT
◾️Tension pneumothorax is a progressive pathology
◾️Life threatening as it worsens
◾️Diagnosed clinically
◾️Requires emergency decompression:
◾️Needle & finger thoracostomy are options
◾️Follow-up with tube thoracostomy for definitive treatment
End/🧵
Image credits in ALT
Thanks for reading. Please RT/QT from the 1st tweet of the thread which can be found here:
#Medtwitter #MedX #FOAMed #MedEd #Trauma
#Medtwitter #MedX #FOAMed #MedEd #Trauma
Loading suggestions...