
The Fraud of Breast Cancer Overdiagnosis
This thread is the most comprehensive and educational I've done on the subject.
If you find it valuable, please RT.
🧵
This thread is the most comprehensive and educational I've done on the subject.
If you find it valuable, please RT.
🧵

The implementation of the mammography screening program in the US was accompanied by a significant increase in the incidence of breast cancer. This is not surprising, as the goal of screening is to detect cancers years in advance.
The problem is that this incidence has never returned to its initial level, far from it. However this should have occurred if it were simply a matter of advancing the diagnosis.
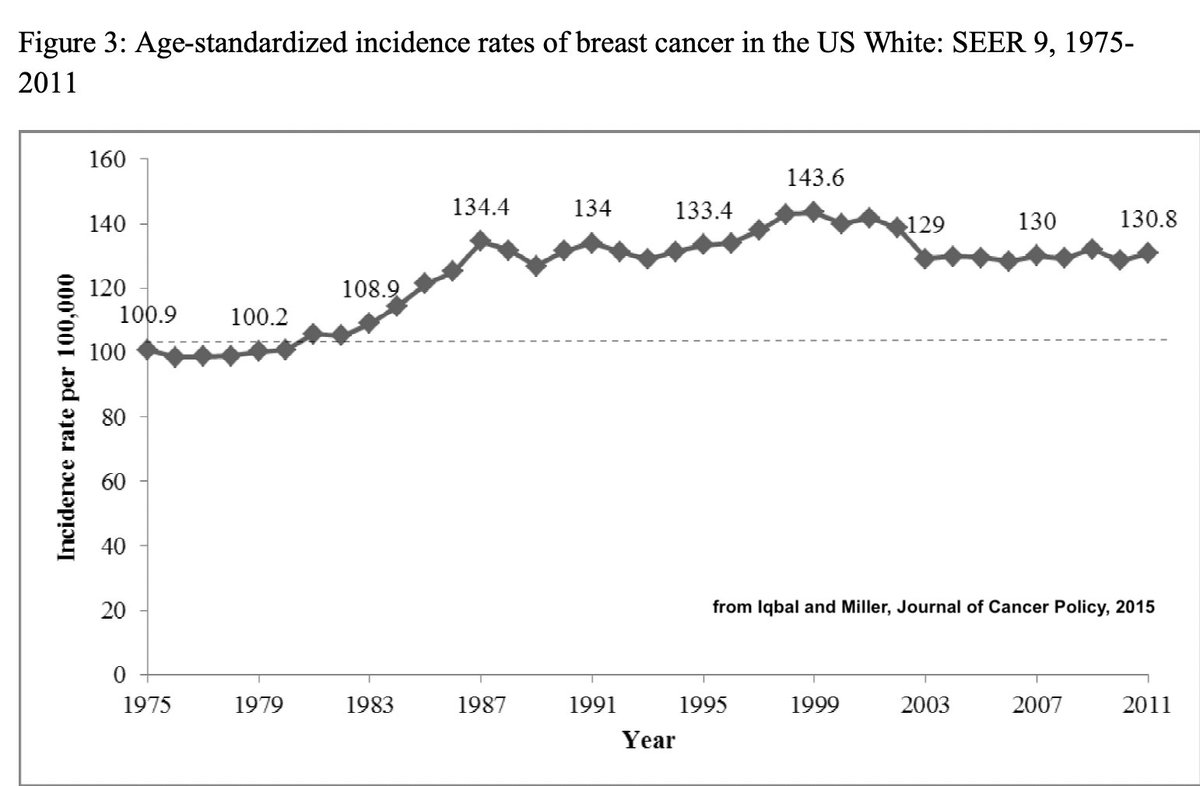
American women ended up with a higher risk of having breast cancer over their lifetime than before screening.
The same increase was observed in all countries that have used mammography screening.
The same increase was observed in all countries that have used mammography screening.
There were two ways to explain the increase:
1) Mammography detected cancers that would never have manifested (overdiagnosis).
2) Mammography itself created cancers because of X-rays.
1) Mammography detected cancers that would never have manifested (overdiagnosis).
2) Mammography itself created cancers because of X-rays.
The second explanation seemed excluded. Why? Because a commission of experts supervised by the U.S. military had evaluated that the risk associated with the radiation dose used for a mammogram was harmless.
There is no data to support this claim; on the contrary.
There is no data to support this claim; on the contrary.
The claim was supported by absurd arguments, such as the fact that the dose received during a one-second mammogram was the same as that received from the natural surroundings over 7 weeks, in an unprecedented propaganda campaign.
cancer.org
cancer.org
In reality, the cancer risks associated with the medical use of X-rays had been identified as early as the late 1960s by John Gofman, who was in charge of studying the biological effects of radiation at the U.S. Atomic Energy Commission.
en.wikipedia.org
en.wikipedia.org

His assessment was not acceptable to the army (which oversaw the implementation of civilian nuclear power, as it was a project on DURC), so they cut his funding and pushed him out. Instead, the AEC selected compliant experts who largely minimized the risk of these radiations.
Later, in 1995, after gathering substantial evidence, Gofman published a book on the risk of radiation and breast cancer, which achieved some success but was met with complete silence from medical and scientific journals, except for negative reviews.
ratical.org
ratical.org
Gofman's scientific articles on this subject, despite his having over 100 publications to his name, were censored. This was the first indication that publications on topics related to dual-use research of concern had to receive the imprimatur of the US Department of Defense.
Towards the late 1990s, information emerged that should have served as a warning: mammography screening had not reduced breast cancer mortality in Sweden.
These initial results were confirmed in all countries: although breast cancer mortality had been reduced thanks to therapeutic advances, screening played no role in this reduction.
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov

These results are paradoxical because screening had shown a significant effect on mortality within 7 years in an RCT under less favorable conditions pubmed.ncbi.nlm.nih.gov
and BC was a type of cancer for which there were strong reasons to predict the efficacy of screening.
and BC was a type of cancer for which there were strong reasons to predict the efficacy of screening.

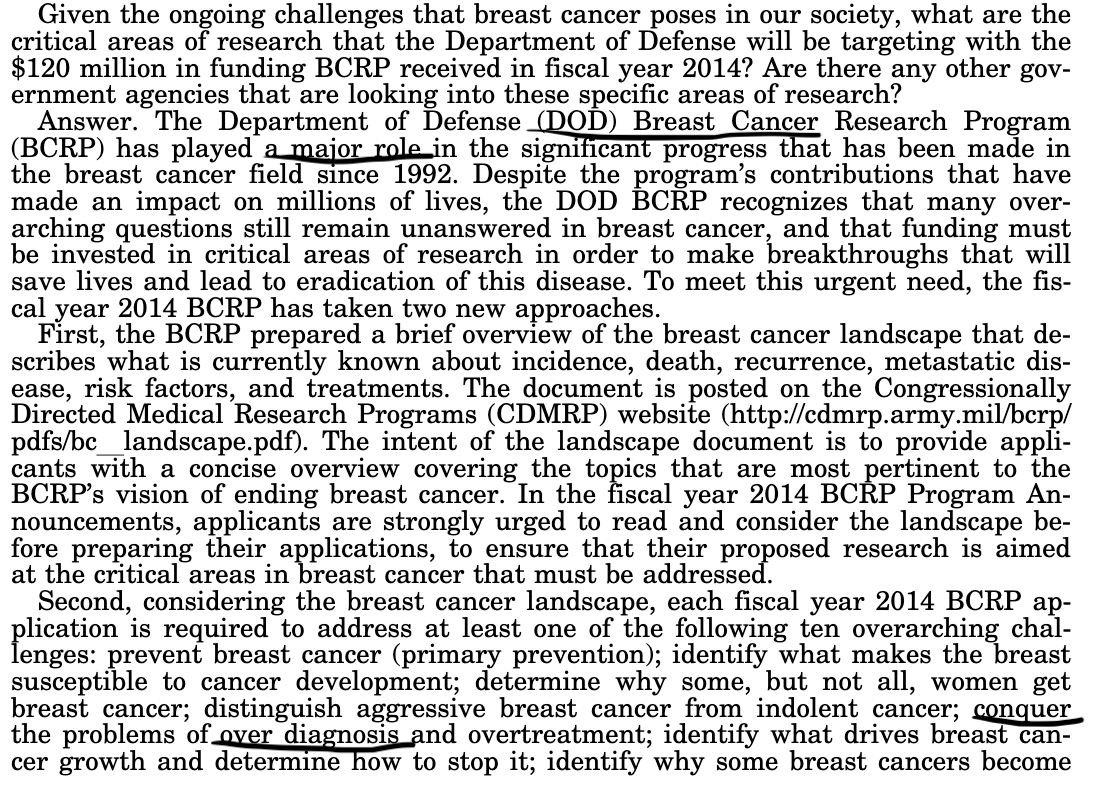
The explanation that should have come to mind was that the benefit was nullified by K caused by X-rays. However, this explanation was off-limits, and instead, a wave of opponents to mammographic screening emerged arguing that the excess cancers observed were due to overdiagnosis.
In reality, the hypothesis of overdiagnosis was very convenient for the U.S. Department of Defense, which risked having 30 years of cover-up with incalculable consequences exposed. As a result, they started steering researchers in this direction.
When studying the incidence of metastatic cancer in the USA, epidemiologist Gil Welch made an even more troubling observation: breast cancer screening had not reduced the incidence of metastatic breast cancer at all.
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov

Here, any explanation regarding an adverse hidden effect of treatments could be excluded, and to explain the lack of reduction, there was only one reasonable explanation: cancers induced by mammograms.
However, Welch proposed another far-fetched explanation, suggesting that aggressive cancers were slipping through the net. And among the co-authors was a well-known figure whose presence in an epidemiology paper was quite puzzling.
David Gorski, a surgeon conducting cell biology research on breast cancer, is best known for opposing medical "disinformation" and promoting pro-vaccine propaganda. Many have suspected him of being a stooge for Big Pharma.
However, if you look at his funding, this is not the case. Gorski is funded by the Department of Defense. Since the NIAID became an appendage of the DoD, vaccines and the overdiagnosis hypothesis of breast cancer have become major concerns for the DoD.
Welch's work led me to develop methods to distinguish excess cancers related to X-rays from cancers related to detection (which could correspond to overdiagnosis) by studying the occurrence dates by age group.
biorxiv.org
biorxiv.org
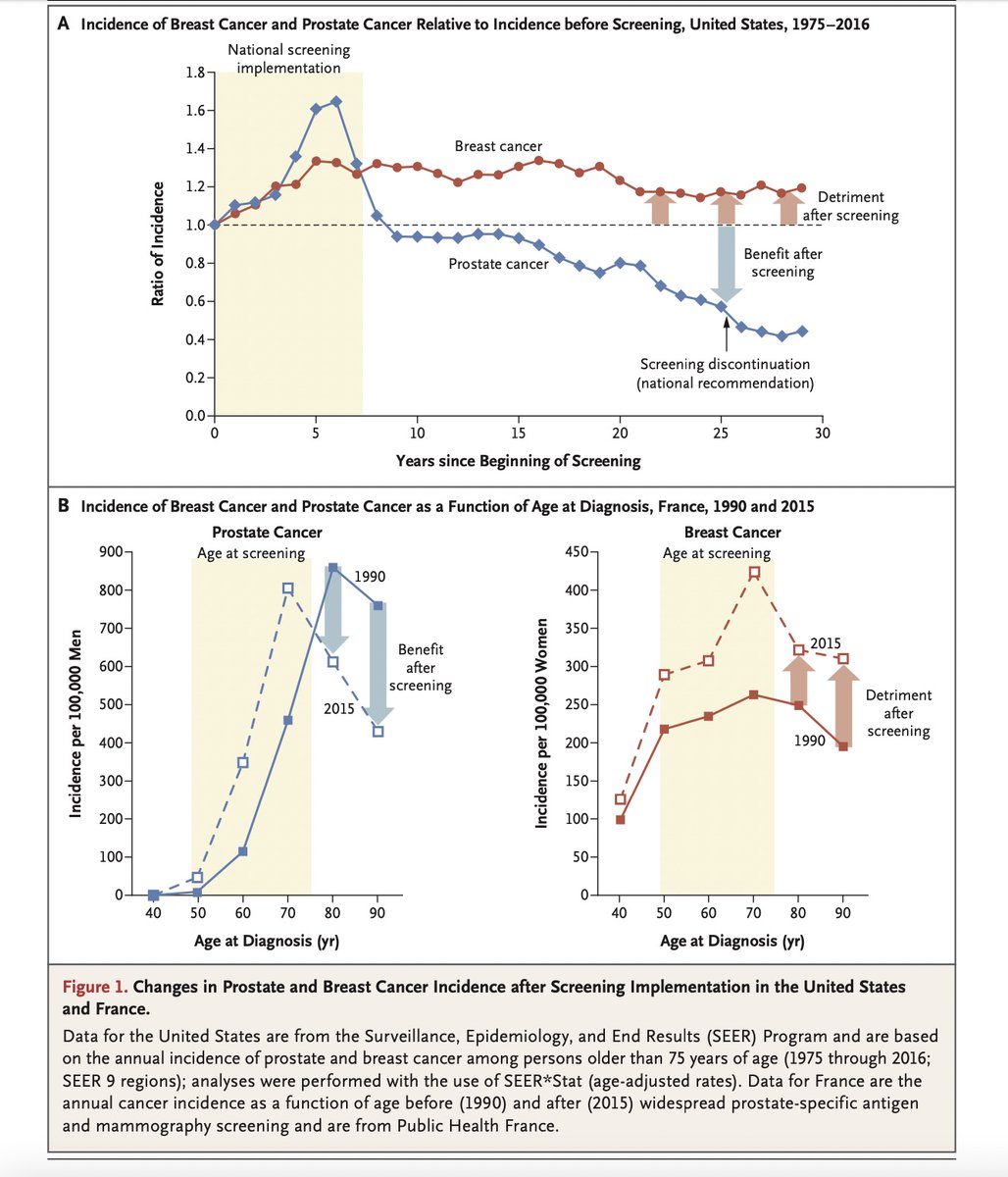

The result is unambiguous: the majority of the long-term increase in incidence is related to delayed-onset cancers. This work led to my dismissal from Inserm by Yves Lévy, a friend of Fauci, the head of US biodefense.
Meanwhile, the fraudsters promoting breast cancer overdiagnosis, who remain on the denial of radiological risks, continue to publish and hold conferences. Any resemblance to what is happening regarding the origins of Covid could only be coincidental.
Loading suggestions...