

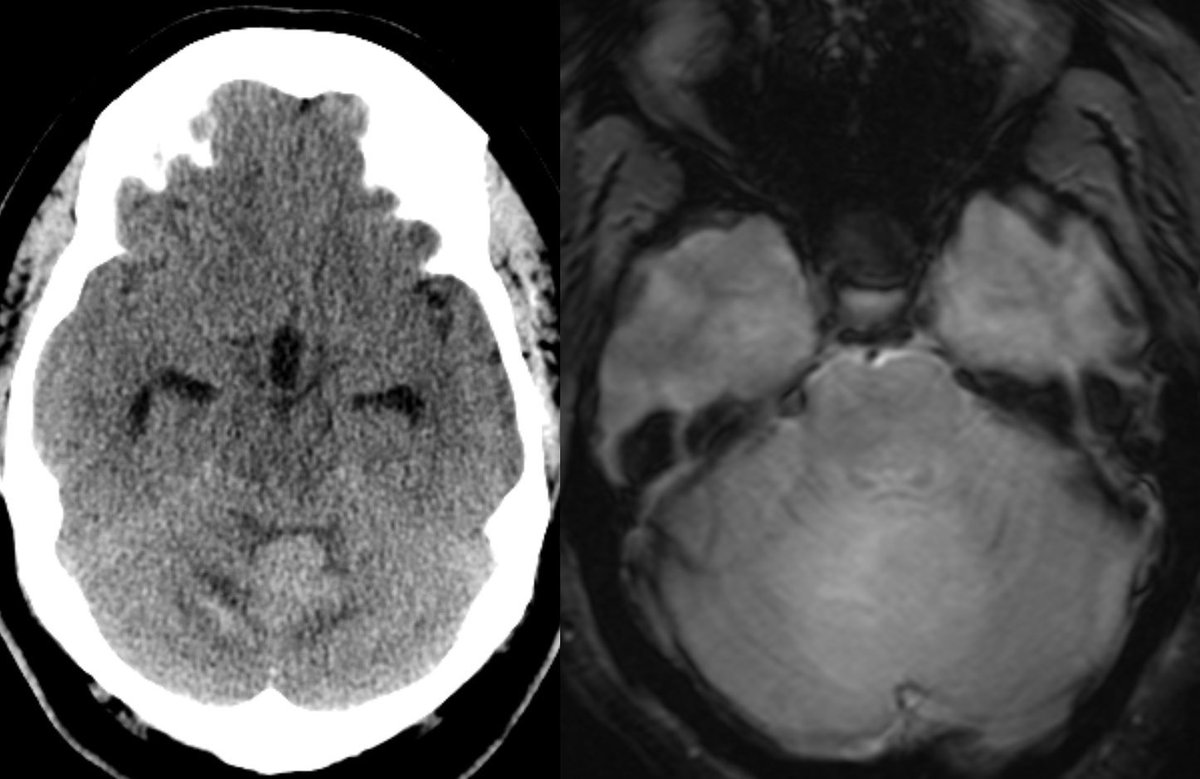
45 y/o M with no PMH presents w/ 1 month of persistent headaches followed by nausea & vomiting, what is the most likely diagnosis?
#Neurosurgery #MedEd #medicine #radres #futureradres #Neurology #ENT @AlbanyMedRadRes @TheASNR x.com
#Neurosurgery #MedEd #medicine #radres #futureradres #Neurology #ENT @AlbanyMedRadRes @TheASNR x.com
🔷Answer: Medulloblastoma, sonic hedgehog (SHH) activated
▶️Medulloblastona can be divided into 4 subgroups, each with unique survival, age demographics, and genetics:
1️⃣Wingless (WNT)
2️⃣Sonic Hedgehog (SHH)
3️⃣Group 3
4️⃣Group 4 (most common subgroup)
▶️Medulloblastona can be divided into 4 subgroups, each with unique survival, age demographics, and genetics:
1️⃣Wingless (WNT)
2️⃣Sonic Hedgehog (SHH)
3️⃣Group 3
4️⃣Group 4 (most common subgroup)
▶️Subgroup sonic hedgehog: ~30% of medulloblastomas
▶️Arise from granule cell precursors to FORM THE CEREBELLAR CORTEX (why SHH subgroup often looks cortically based in the cerebellum)
▶️Arise from granule cell precursors to FORM THE CEREBELLAR CORTEX (why SHH subgroup often looks cortically based in the cerebellum)
🔷Epidemiology: Bimodal age distribution of infants and adults w/ slight M predominance
🔷Prognosis is intermediate though worsened by associated MYCN or TP53 mutations
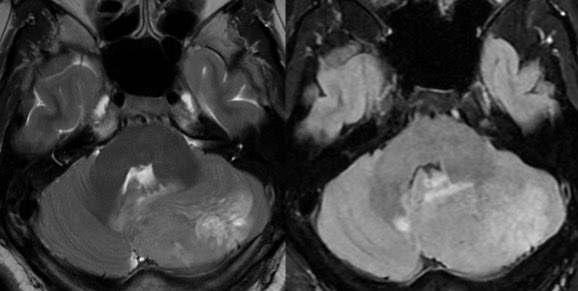
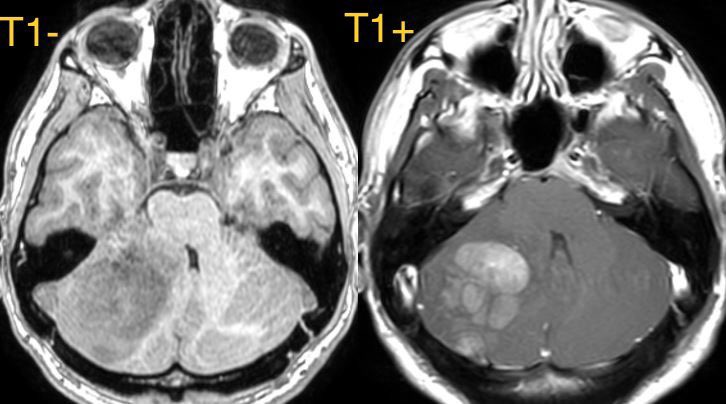
🔷Location: Most commonly LATERALLY IN THE CEREBELLAR HEMISPHERES (~62%)
🔷Prognosis is intermediate though worsened by associated MYCN or TP53 mutations
🔷Location: Most commonly LATERALLY IN THE CEREBELLAR HEMISPHERES (~62%)
🔷Predicting subgroup by LOCATION (not exclusive):
1️⃣Cerebellar peduncle/CP angle cistem: Wingless (WNT)
2️⃣Cerebellar hemispheres (lateral): Sonic Hedgehog (SHH)
3️⃣Midline/intraventricular: Predominantly but not exclusively groups 3 and 4
1️⃣Cerebellar peduncle/CP angle cistem: Wingless (WNT)
2️⃣Cerebellar hemispheres (lateral): Sonic Hedgehog (SHH)
3️⃣Midline/intraventricular: Predominantly but not exclusively groups 3 and 4
🔷Imaging:
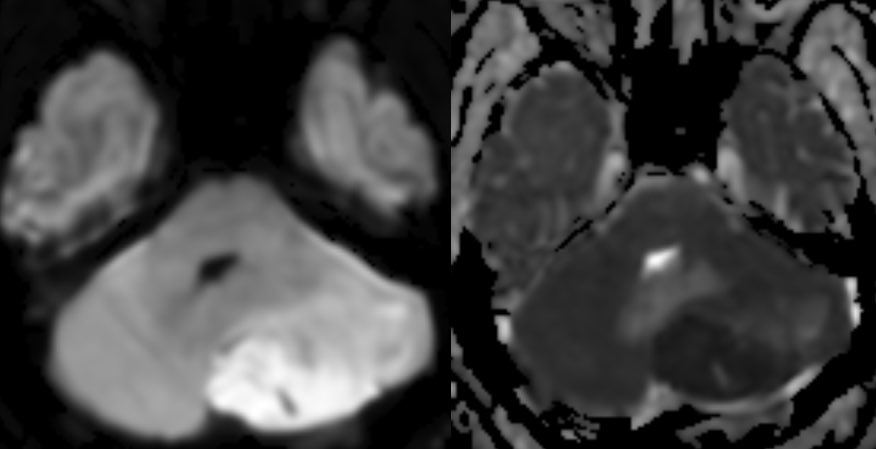
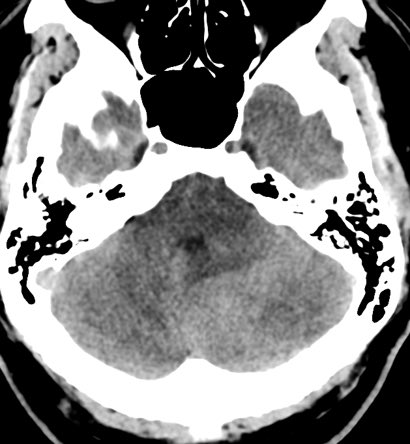
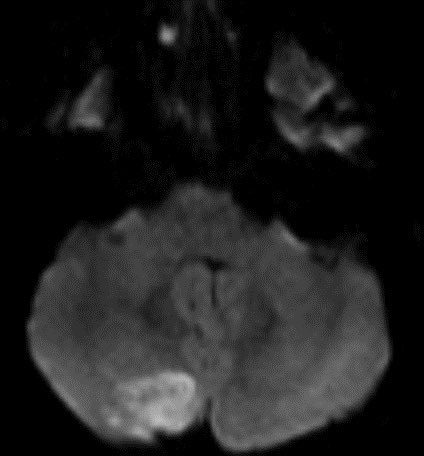
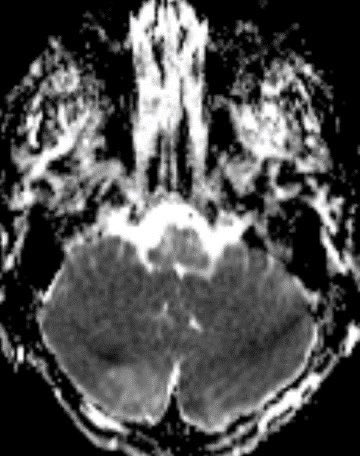
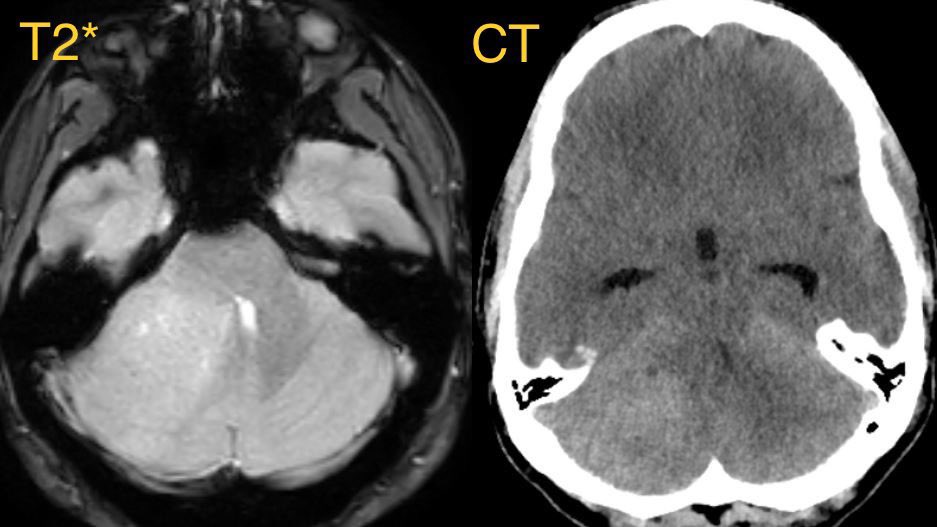
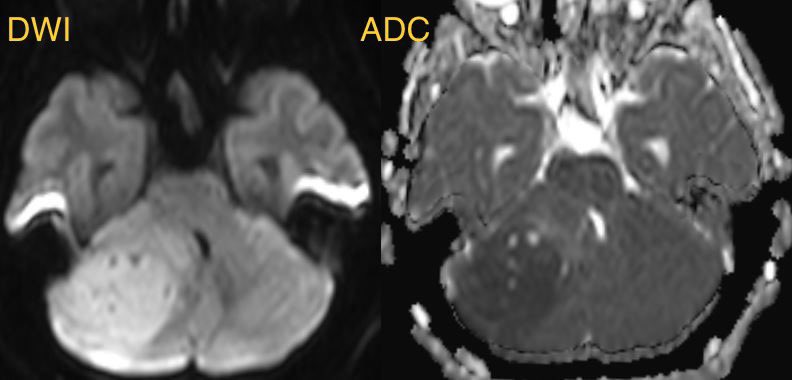
💡 Hypercellular tumor so DENSE on CT and DIFFUSION RESTRICTION (consistent feature)
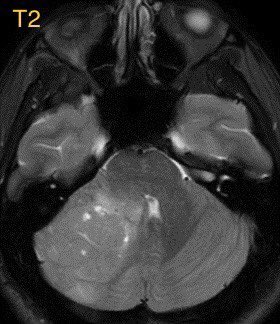
▶️Round/lobulated morphology
▶️Hemorrhage is rare but calcifications seen in ~20%
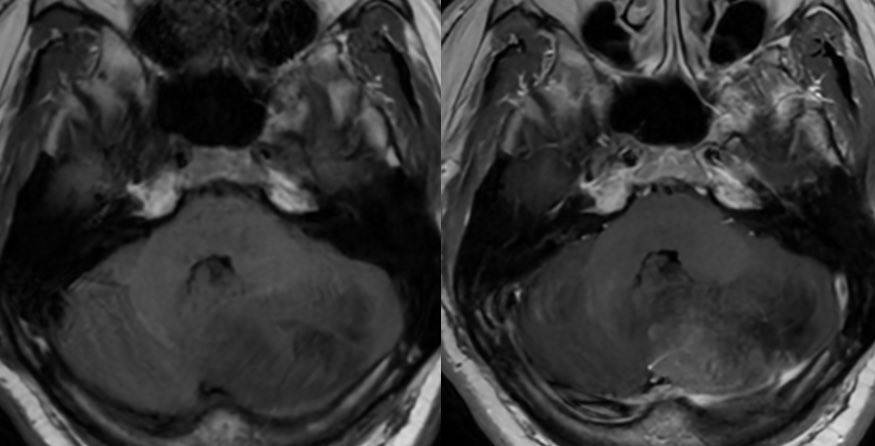
💡 Most medulloblastomas enhance except group 4 which may have minimal to no enhancement
💡 Hypercellular tumor so DENSE on CT and DIFFUSION RESTRICTION (consistent feature)
▶️Round/lobulated morphology
▶️Hemorrhage is rare but calcifications seen in ~20%
💡 Most medulloblastomas enhance except group 4 which may have minimal to no enhancement
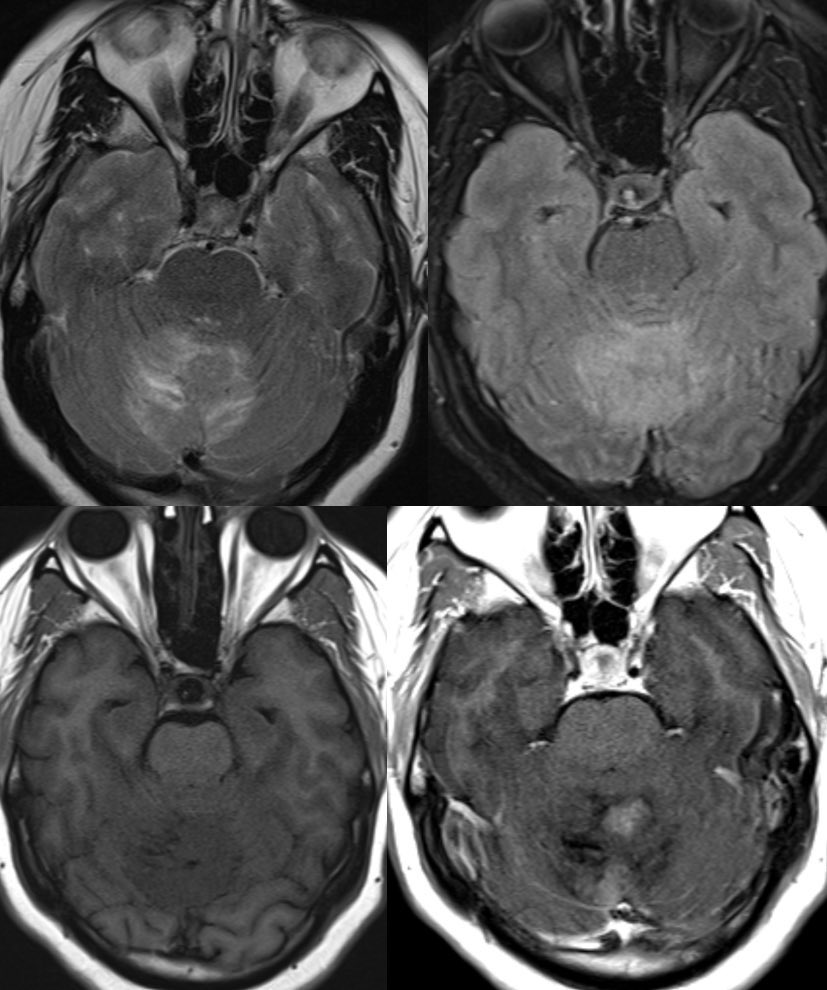
⭐️ Companion case of Lhermitte-Duclos - Unilateral cerebellar mass w/ striations due to hyperintense expanded fovea on T2 w/ normal signal intervening parenchyma
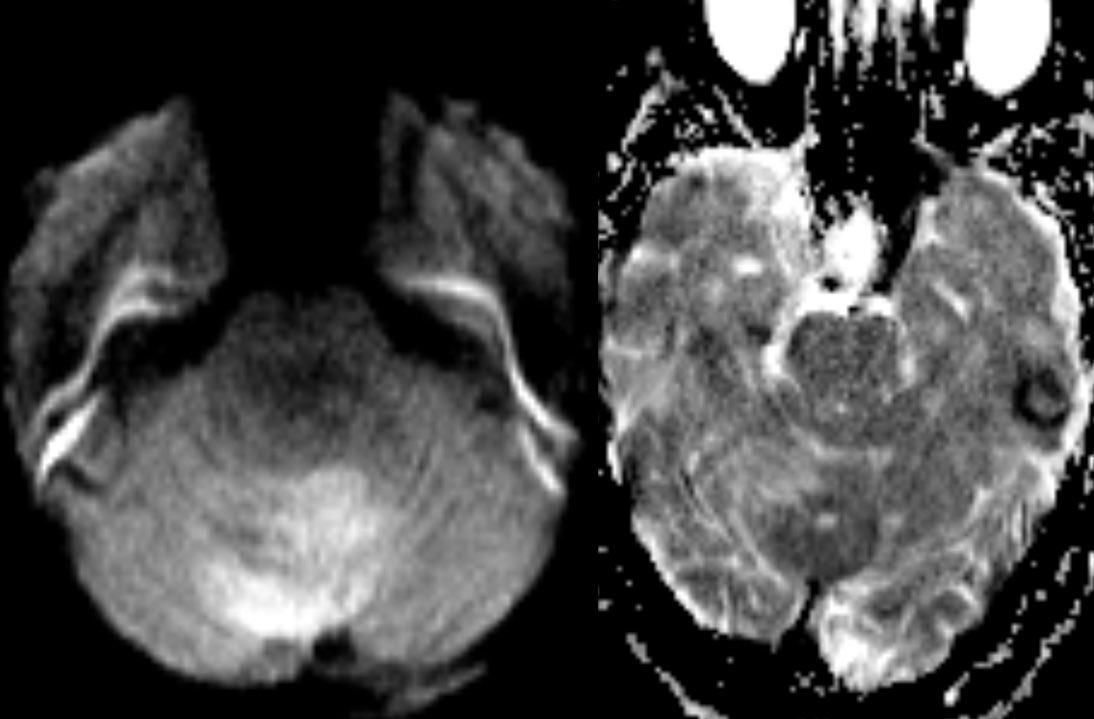
Typically there is no to little enhancement and high signal on DWI due to T2 shine-through w/ high signal on ADC x.com
Typically there is no to little enhancement and high signal on DWI due to T2 shine-through w/ high signal on ADC x.com



💡 Most important job as a rad is to search for metastatic disease (leptomeningeal and systemic)!
💡 Both Lhermitte-Duclos & Medulloblastoma SHH can have a striated appearance! Use DWI/ADC, density on CT, & enhancement to distinguish!
For more 📖 pubmed.ncbi.nlm.nih.gov
💡 Both Lhermitte-Duclos & Medulloblastoma SHH can have a striated appearance! Use DWI/ADC, density on CT, & enhancement to distinguish!
For more 📖 pubmed.ncbi.nlm.nih.gov

Loading suggestions...