

1/
One of the BIGGEST #POCUS misconceptions is that B lines 🟰 pulmonary edema 🤦♀️
Did you know that there is actually a wide DDx for B lines?
Check out the latest @ubcimpocus video about #LungUltrasound for interstitial syndromes 👀; or read on for the highlights 👇 🧵
youtube.com
One of the BIGGEST #POCUS misconceptions is that B lines 🟰 pulmonary edema 🤦♀️
Did you know that there is actually a wide DDx for B lines?
Check out the latest @ubcimpocus video about #LungUltrasound for interstitial syndromes 👀; or read on for the highlights 👇 🧵
youtube.com
2/
Remember that B lines are generated because of something filling the (normally aerated) interstitium and interlobular septae.
Fluid can of course fill these spaces; but so can other things!
Pus, cells, fibrosis, blood - anything that can give you an interstitial pattern on a chest X ray can give you B lines on ultrasound.
Remember that B lines are generated because of something filling the (normally aerated) interstitium and interlobular septae.
Fluid can of course fill these spaces; but so can other things!
Pus, cells, fibrosis, blood - anything that can give you an interstitial pattern on a chest X ray can give you B lines on ultrasound.
3/
Broadly speaking, we can divide B lines into 2 categories. B lines arising from:
- Cardiogenic pulmonary edema 🫀
vs
- Infectious/inflammatory pathology 🦠
The latter includes things like atypical or viral pneumonias, ARDS, interstitial lung disease, lymphangitic carcinomatosis, etc.
Broadly speaking, we can divide B lines into 2 categories. B lines arising from:
- Cardiogenic pulmonary edema 🫀
vs
- Infectious/inflammatory pathology 🦠
The latter includes things like atypical or viral pneumonias, ARDS, interstitial lung disease, lymphangitic carcinomatosis, etc.
4/
And there are several ultrasound features that we can use to tease apart these two types.
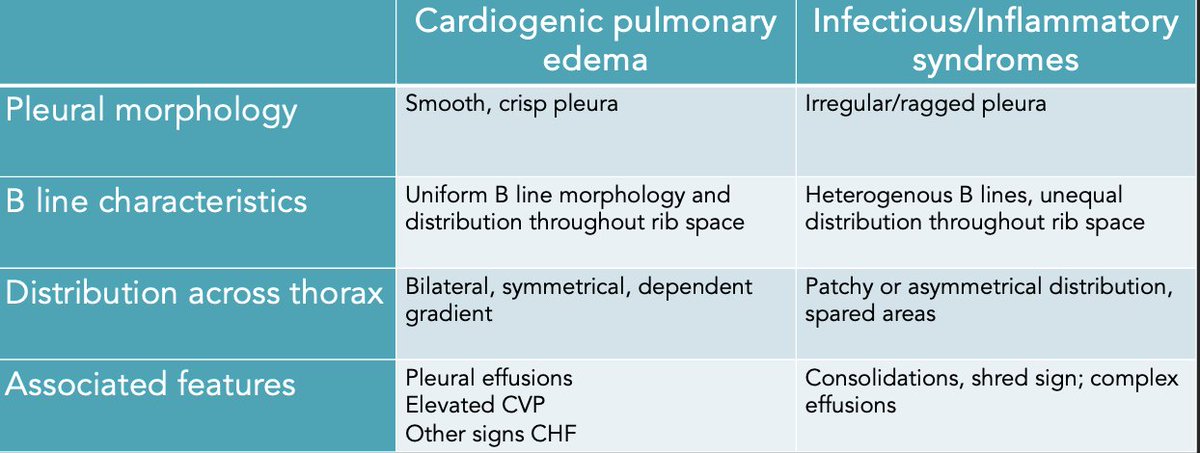
First: we can look at the pleural morphology.
B lines arising from a smooth, crisp, uniform pleural line are more likely to be from cardiogenic pulmonary edema. x.com
And there are several ultrasound features that we can use to tease apart these two types.
First: we can look at the pleural morphology.
B lines arising from a smooth, crisp, uniform pleural line are more likely to be from cardiogenic pulmonary edema. x.com

5/
In contrast, B lines arising from an irregular, ragged, interrupted pleural line are more likely to be from infectious/inflammatory pathologies.
(If you want to know WHY this happens - check out the video posted above!👆)
Note that it is key here for you as the scanner to use proper #LUS technique and employ fanning to ensure that your beam is perpendicular to the pleura.
In contrast, B lines arising from an irregular, ragged, interrupted pleural line are more likely to be from infectious/inflammatory pathologies.
(If you want to know WHY this happens - check out the video posted above!👆)
Note that it is key here for you as the scanner to use proper #LUS technique and employ fanning to ensure that your beam is perpendicular to the pleura.

6/
Next, we can look at the distribution of B lines across the interspace.
Pleural fluid fills interlobular septae in a predictable and regular way; which generates B lines that are evenly spaced throughout the whole interspace. x.com
Next, we can look at the distribution of B lines across the interspace.
Pleural fluid fills interlobular septae in a predictable and regular way; which generates B lines that are evenly spaced throughout the whole interspace. x.com

7/
In contrast, with infectious/inflammatory pathologies, you will see B lines which are NOT homogenous throughout the interspace.
You may see all the B lines arising from a single point on the pleura; or even A lines throughout part of the interspace. x.com
In contrast, with infectious/inflammatory pathologies, you will see B lines which are NOT homogenous throughout the interspace.
You may see all the B lines arising from a single point on the pleura; or even A lines throughout part of the interspace. x.com

8/
Next, we can look at the distribution of B lines across the thorax.
Note that this is why we always have to scan representative areas of BOTH sides of the chest - you cannot just take a single clip and call it pulmonary edema‼️
B lines arising from pulmonary edema should be bilateral, symmetrical, and in a dependent gradient (ie. most prominent at the bases).
B lines from infectious/inflammatory pathologies, on the other hand, are often asymmetrical, non-gravitational, and may display skipped or spared areas.
Next, we can look at the distribution of B lines across the thorax.
Note that this is why we always have to scan representative areas of BOTH sides of the chest - you cannot just take a single clip and call it pulmonary edema‼️
B lines arising from pulmonary edema should be bilateral, symmetrical, and in a dependent gradient (ie. most prominent at the bases).
B lines from infectious/inflammatory pathologies, on the other hand, are often asymmetrical, non-gravitational, and may display skipped or spared areas.

9/
Finally, we can look at other associated pathology.
In heart failure, for example, we will often see other features such as bilateral simple pleural effusions; plus cardiac findings supportive of CHF.
In inflammatory/infectious causes, you may see things like unilateral consolidations, dynamic air bronchograms, shred signs, complex effusions, etc.
Finally, we can look at other associated pathology.
In heart failure, for example, we will often see other features such as bilateral simple pleural effusions; plus cardiac findings supportive of CHF.
In inflammatory/infectious causes, you may see things like unilateral consolidations, dynamic air bronchograms, shred signs, complex effusions, etc.

10/
Of course - it goes without saying! - that all of these ultrasound findings should be incorporated with the rest of the clinical picture to help you reach a decision 🩺 x.com
Of course - it goes without saying! - that all of these ultrasound findings should be incorporated with the rest of the clinical picture to help you reach a decision 🩺 x.com
11/
Thanks for reading! 🙏
For more on #LungUltrasound, including image acquisition and common pitfalls - check out the rest of the videos on the ubcimpocus site ✨
Drop you #LUS pearls here! #MedTwitter #Tweetorial #POCUS #LungUltrasound
ubcimpocus.com
Thanks for reading! 🙏
For more on #LungUltrasound, including image acquisition and common pitfalls - check out the rest of the videos on the ubcimpocus site ✨
Drop you #LUS pearls here! #MedTwitter #Tweetorial #POCUS #LungUltrasound
ubcimpocus.com

Ping some fellow #POCUS nerds - @G2Disrupt @ria_dancel @DrGalenMD @ross_prager @KiranRikhraj @shanearish @BuddingSprout @HoosierPocus
Loading suggestions...