

1/ What is your differential diagnosis for an individual who is having recurrent asthma exacerbations despite optimal therapy? @VCU_PCCM @crit_caring_MD @PDjack1984 @MichaeLheureux @KevinSwiatek @AndreaMytinger @lkbrath @PSinkam @samirashojaee @AvrahamCooperMD #tweetorial

2/ The differential diagnosis is broad but potential etiologies include:
1⃣ Does this patient actually have asthma?
2⃣ Infectious (bacterial, fungal, viral)
3⃣ GERD
4⃣ Congestive Heart Failure
5⃣ Vocal Cord Dysfunction
@mdlizs @mkashiouris @B_M_Wiese @ptfaddenMD @DxRxEdu
1⃣ Does this patient actually have asthma?
2⃣ Infectious (bacterial, fungal, viral)
3⃣ GERD
4⃣ Congestive Heart Failure
5⃣ Vocal Cord Dysfunction
@mdlizs @mkashiouris @B_M_Wiese @ptfaddenMD @DxRxEdu
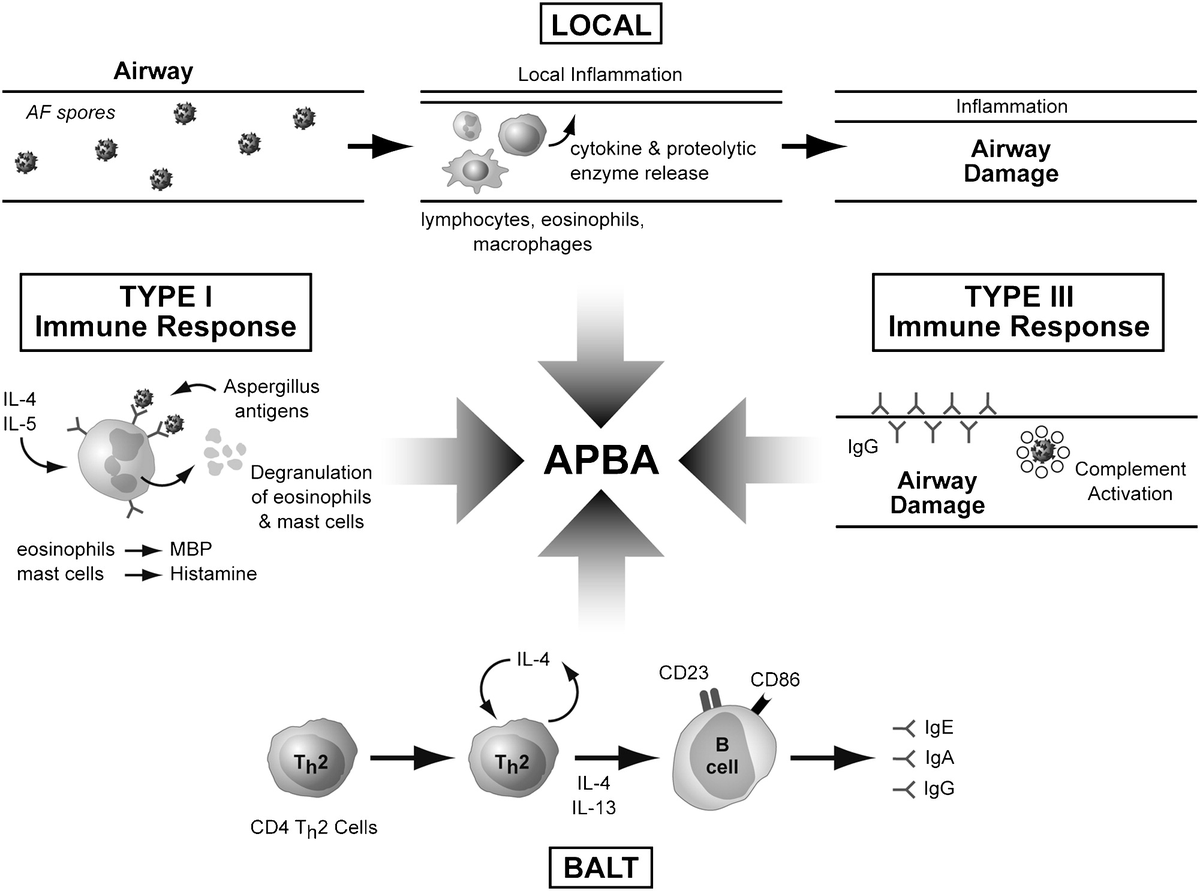
3/ Today we will discuss allergic bronchopulmonary aspergillosis (ABPA), which is an immunological disorder due to hypersensitivity to aspergillus fumigatus. The prevalence of this disease is not widely known; however, literature suggests it be around 13% in asthma clinics.


4/ This schematic from Riscili et al. from Clinics in Chest Medicine (2009) demonstrates that there is an abnormal local and systemic response to aspergillus antigens resulting in airway damage and a proinflammatory response. @PaulNWilliamz @DoctorWatto @BrighamSK
5/ 3 large case series of ABPA patients published in @accpchest shows that the most common clinical signs of APBA include:
1⃣ Low Grade Fever
2⃣ Wheezing
3⃣ Bronchial Hyperreactivity
4⃣ Productive Cough (brown sputum plugs in 31-69% pts)
5⃣ Hemoptysis
@CPSolvers @thecurbsiders
1⃣ Low Grade Fever
2⃣ Wheezing
3⃣ Bronchial Hyperreactivity
4⃣ Productive Cough (brown sputum plugs in 31-69% pts)
5⃣ Hemoptysis
@CPSolvers @thecurbsiders
6/ Laboratory findings seen in ABPA include:
1⃣ Elevated total blood eosinophil count (>500 cells/microL)
2⃣ Elevated total serum IgE level (>1000)
3⃣ Specific IgE and IgG antibiodies to aspergillus fumigatus on immunoassay
@EuroRespSoc @aoglasser @gsmartinmd @rabihmgeha
1⃣ Elevated total blood eosinophil count (>500 cells/microL)
2⃣ Elevated total serum IgE level (>1000)
3⃣ Specific IgE and IgG antibiodies to aspergillus fumigatus on immunoassay
@EuroRespSoc @aoglasser @gsmartinmd @rabihmgeha
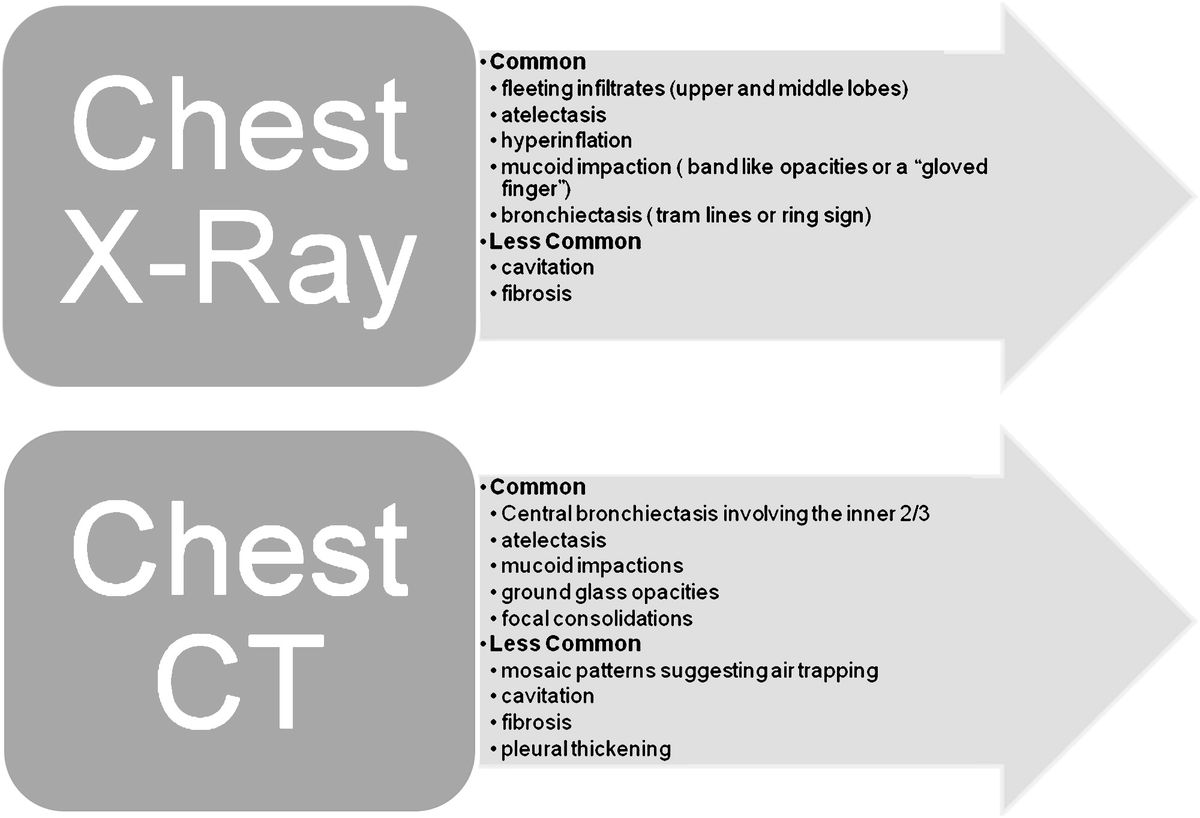
7/ Radiographic findings for ABPA are diverse but typically show fleeting opacities, bronchiectasis, and mucoid impaction. This wonderful graphic from @accpchest summarizes the typical findings. @tony_breu @alan_dow @Leighmurr23 @MESternberg
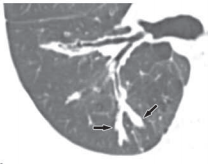
8/ "Finger-in-Glove" or "Gloved Finger" sign on imaging demonstrates airway filling of mucoid secretions that typically radiate from the hilum toward the periphery of the lung. @VCURadRes @marinanaz @NateWarnerMD @jackpenner @AdamRodmanMD @rvawellmd

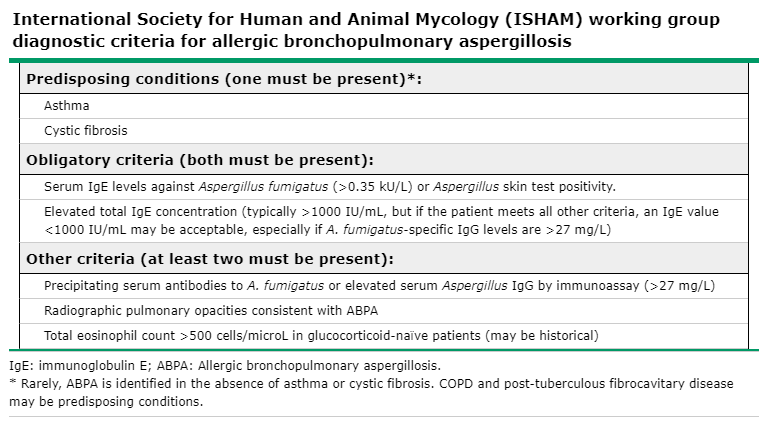
9/ There is currently not a well agreed upon diagnostic criteria for ABPA. However, @ISHAM_Mycology has developed a simplified schema in aiding in the diagnosis of ABPA. @UpToDate
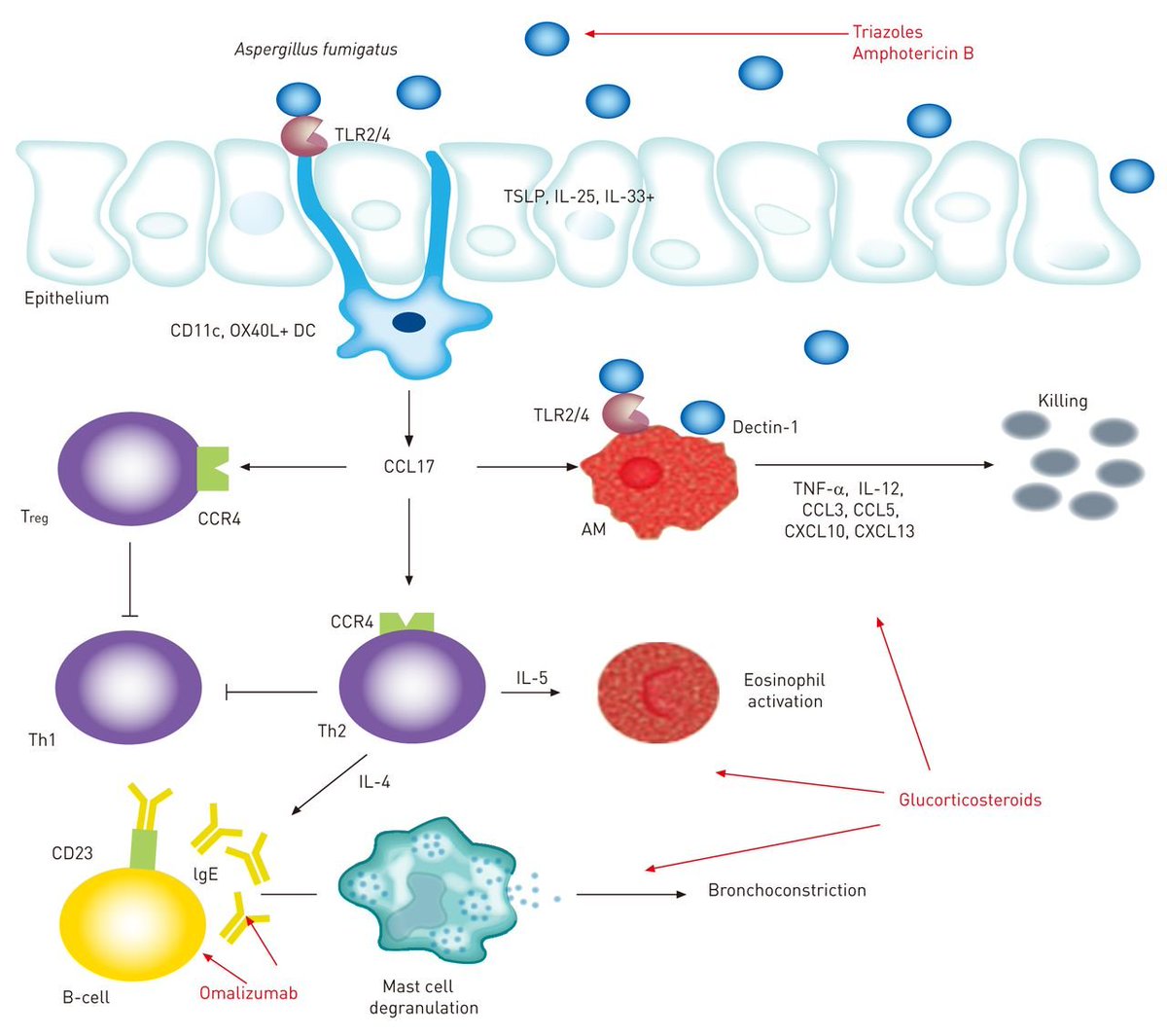
10/ The backbone of treatment is limiting the inflammatory response; therefore, steroids (prednisone 0.5mg/kg/day in acute exacerbations) have been shown to reduce systemic inflammation and improve bronchospasm. @palettala

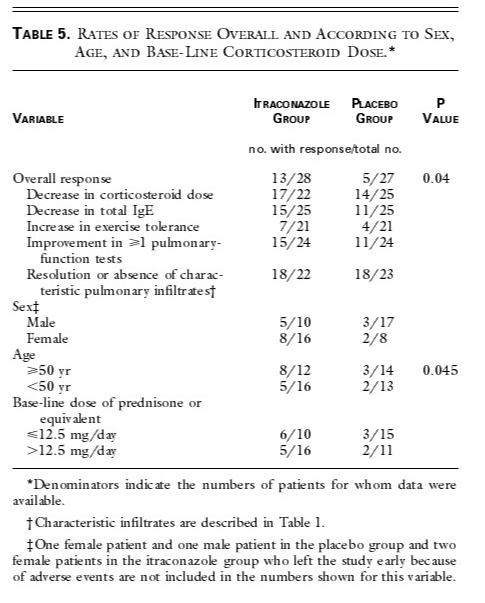
11/ Other adjunctive therapies include anti-fungals, especially itraconazole (best studied). Itraconazole has been shown to improve symptoms, clear infiltrates, and lower the required maintenance steroid therapy. bit.ly
@Dr_Mike_Stevens @ERitterMD @RabiaQaiser3
@Dr_Mike_Stevens @ERitterMD @RabiaQaiser3
12/ Omalizumab (anti-IgE monoclonal Ab) has also been shown to be successful in some case reports; however, there have been no proper controlled studies to demonstrate its efficacy at this time. bit.ly

13/ For further reading, check out this wonderful review on ABPA from @accpchest. bit.ly

Loading suggestions...