

1/ A case: I was asked to assess a pt that just arrived with hypotension and HR in the 20s by my co-attending in the ED. ECG was with no P waves and RBBB w/ LAFB & severe bradycardia. POC K was ordered, and echo done as epinephrine gtt started at 5 mcg/min.
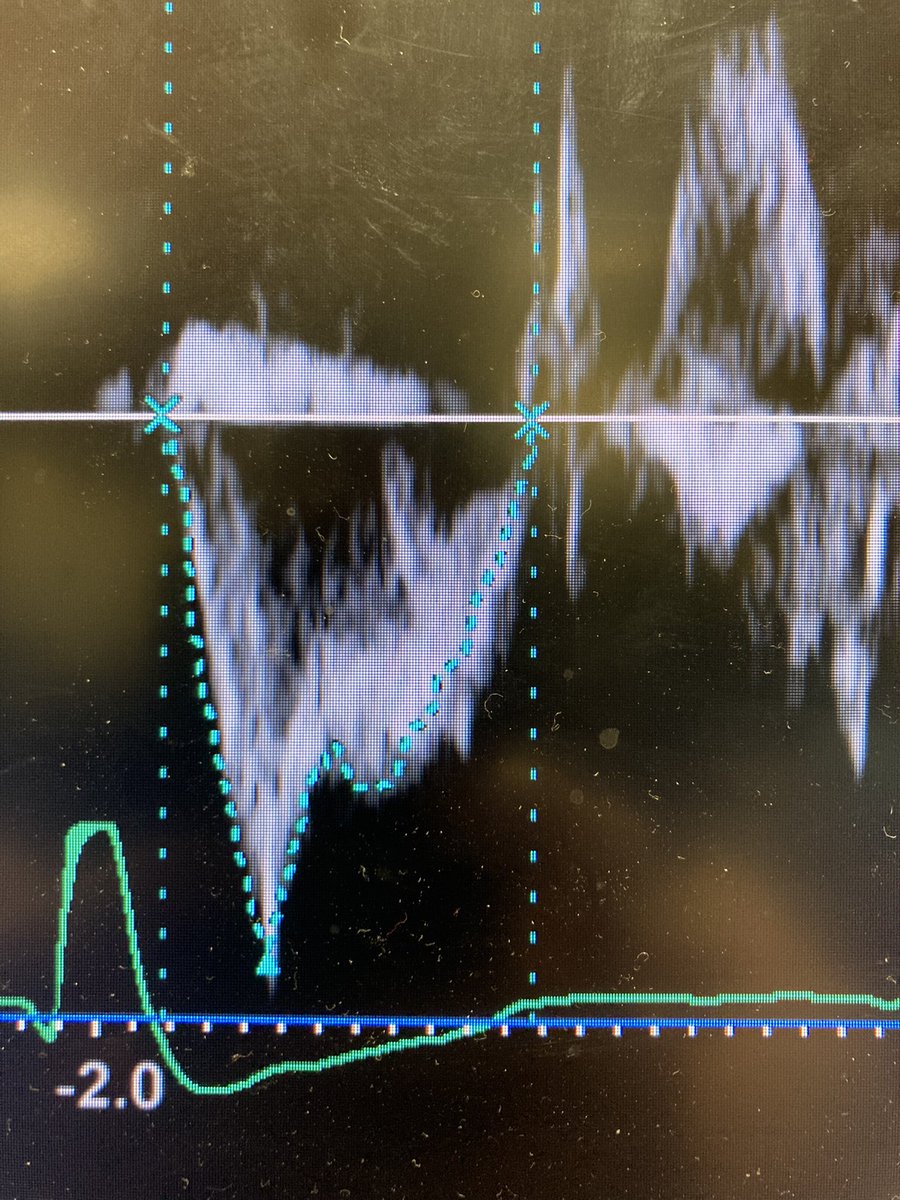
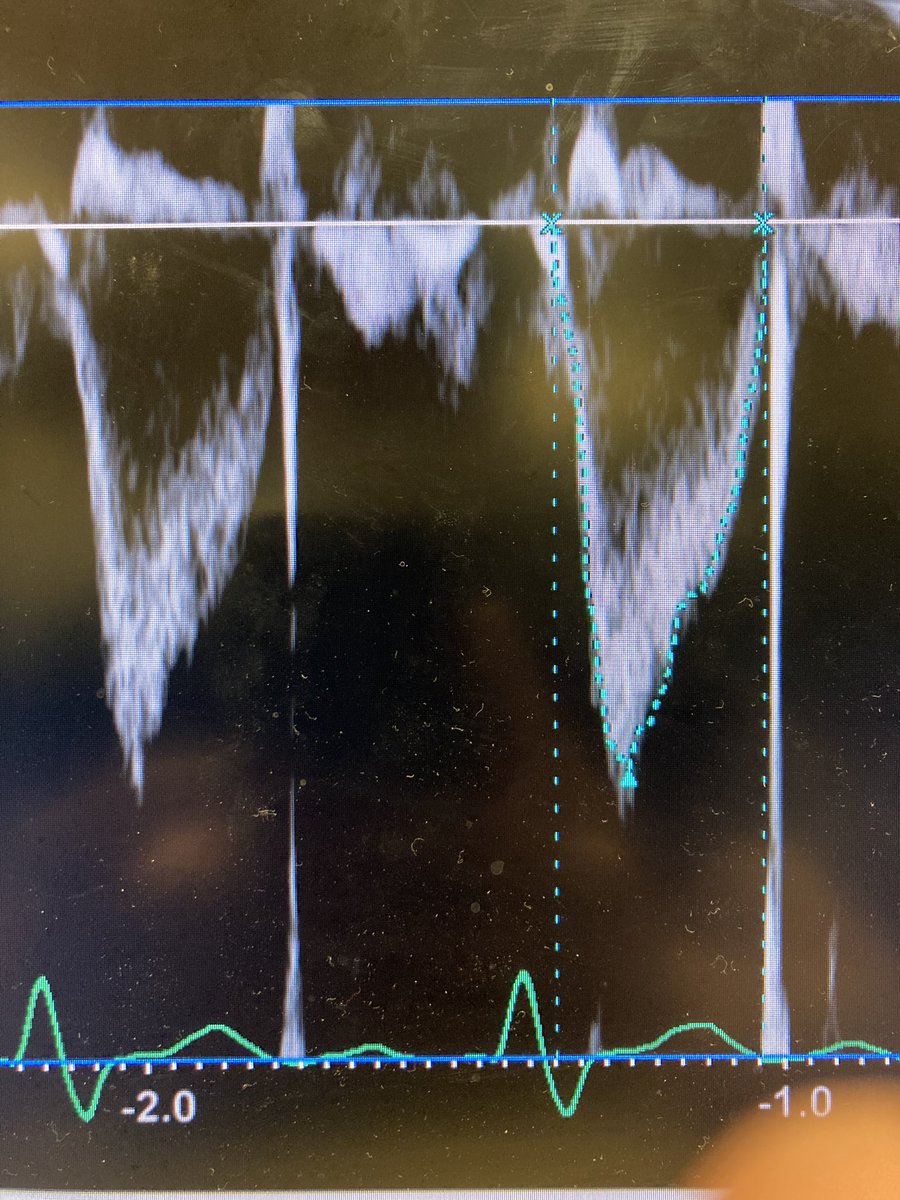
2/ POC echo done immediately. IVC plethoric. Here is LVOT VTI. Note SV 78 cc, HR 30, CO 2.3, calc SVR is 1,160 dynes*sec/cm^5. I didn’t trust diastolic parameters due to the bradycardia so I won’t include but E/e’ was 12.7 & I caught a small A wave not associated with the QRS.

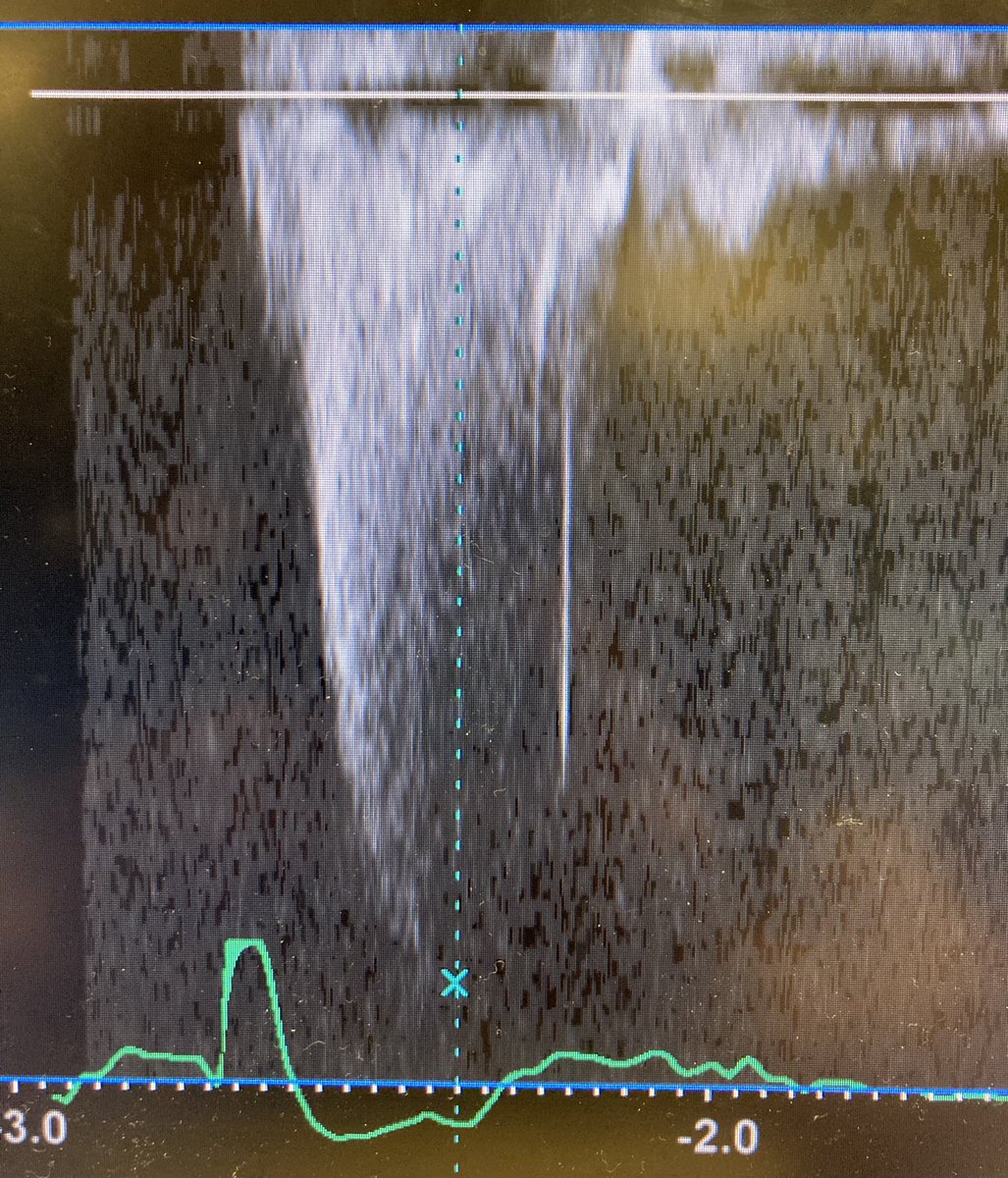
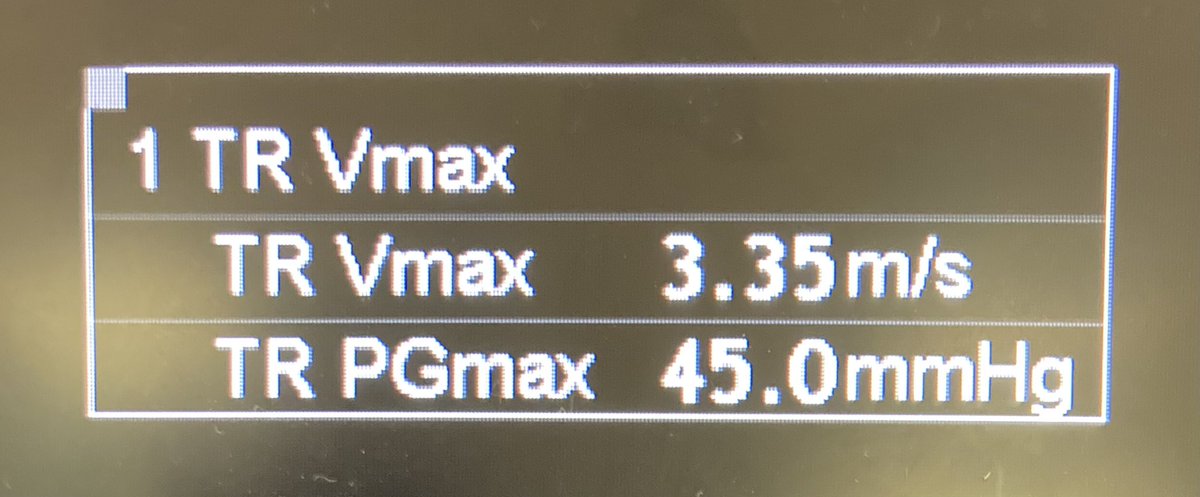
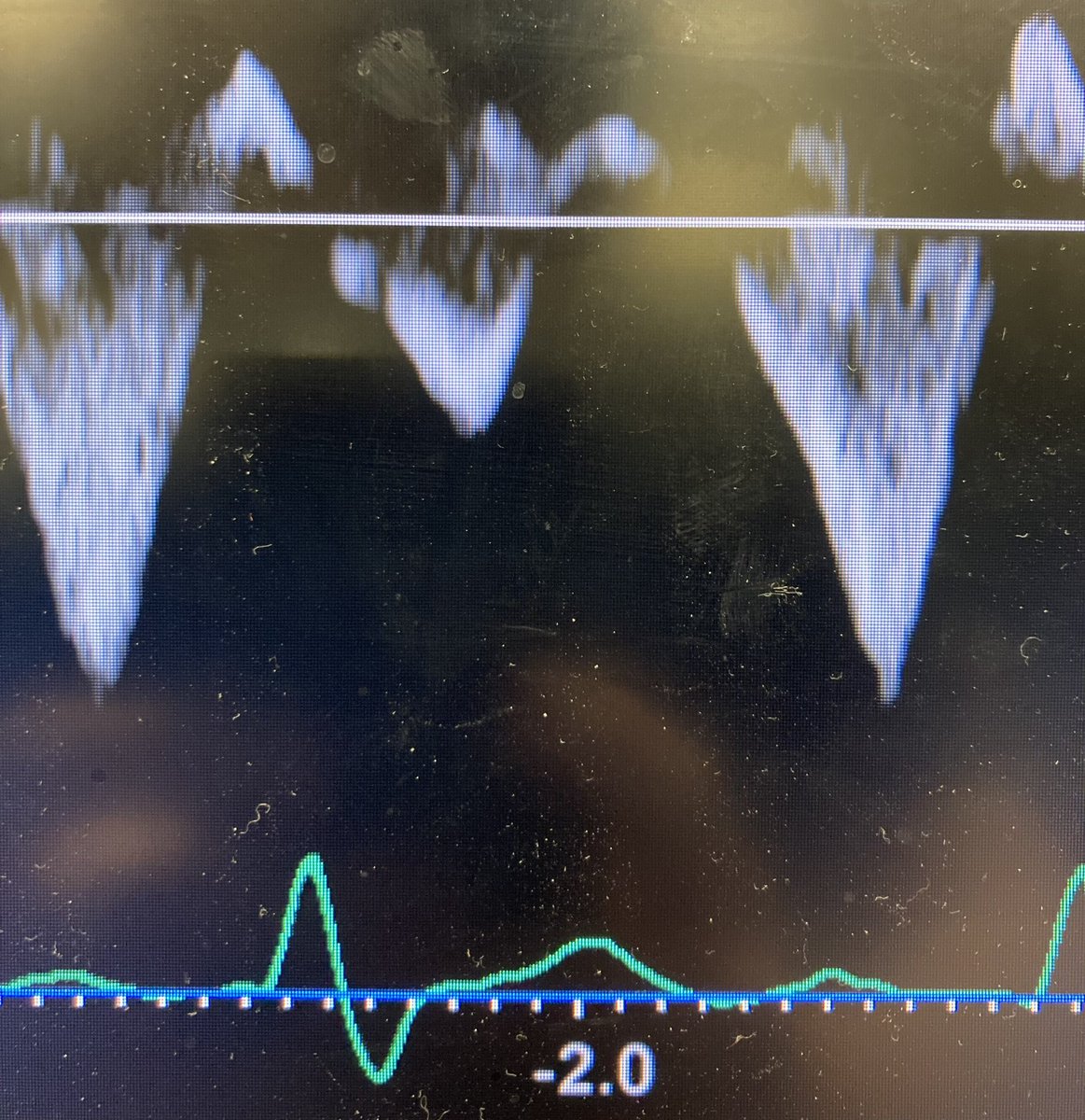
3/ Here is some of right side of the heart: TRpg 37 mmHg (sPAP ~57 mmHg), note the midsystolic notch of the RVOT VTI (highly suggestive of ⬆️PVR), HVD with systolic reversal (due to the very slow rate you can see the D wave first here then S reversal at the end of the trace).
4/ In addition there was interventricular septal shift in systole and diastology: further evidence of increased PVR and RV pressures > LV pressures.
5/ POC K was 7.4 and so the patient was given CaCl2, NaHCO3, Insulin/D10, Albuterol, and furosemide. HR immediately increased to 70s, BP became slightly elevated, and the pt became alert. Skin from ashen to pink. Epinephrine gtt was able to be turned off.
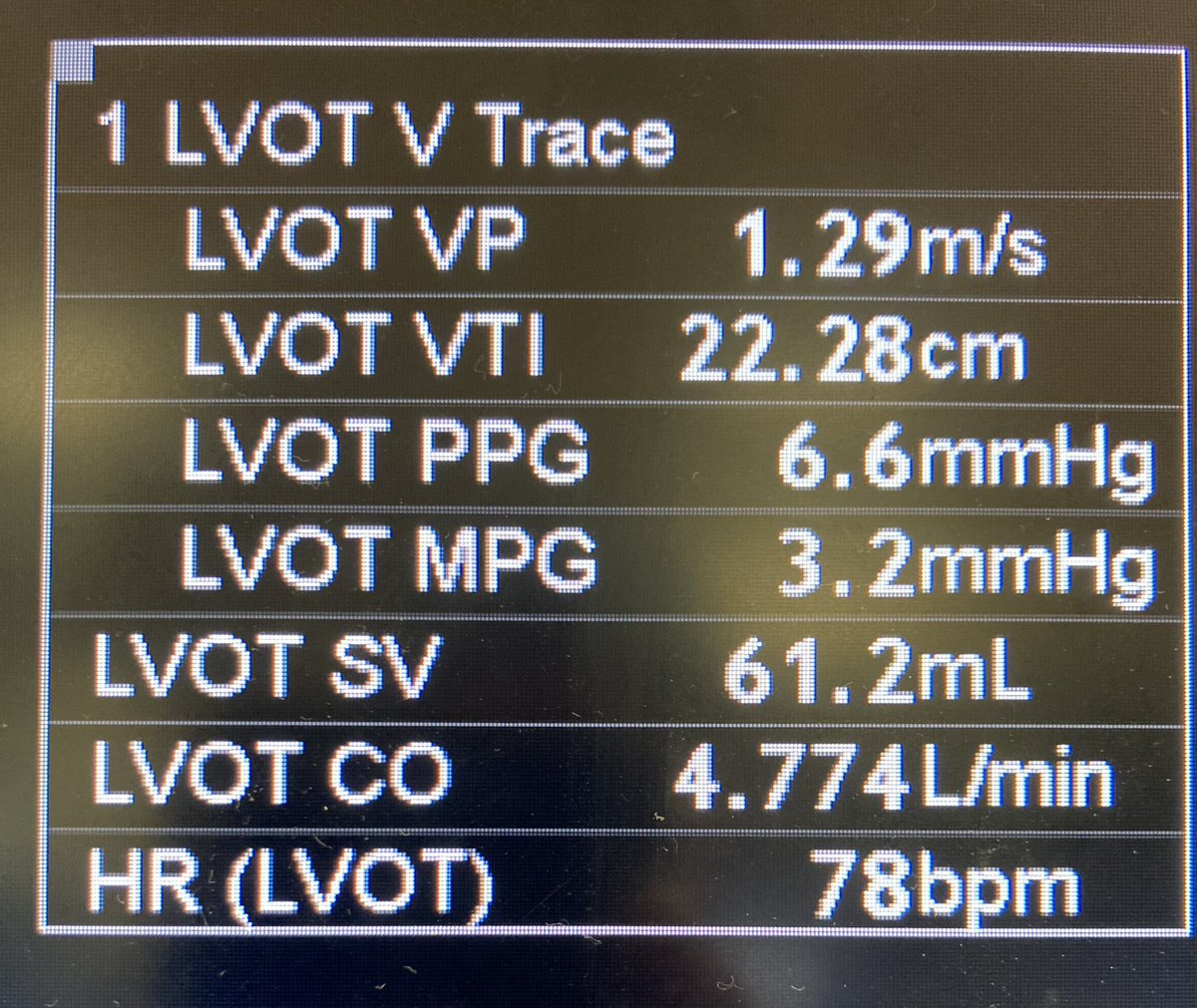
6/ After things had settled down, a repeat POC echo was done. Here is the LVOT data. IVC was now collapsing > 50% and SVR was 880 dynes*sec/cm^5. LAP seemed slightly high from diastolic parameters
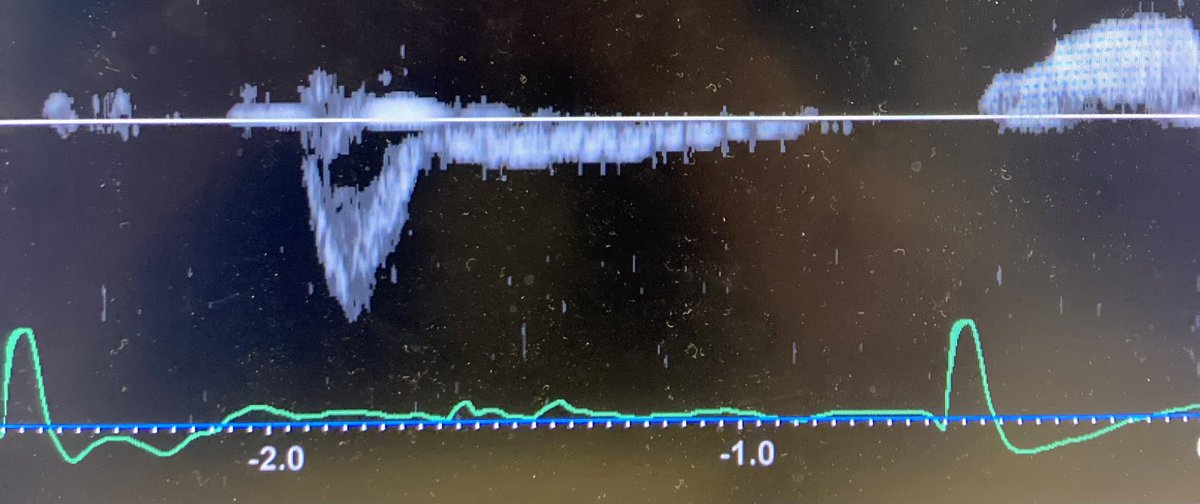
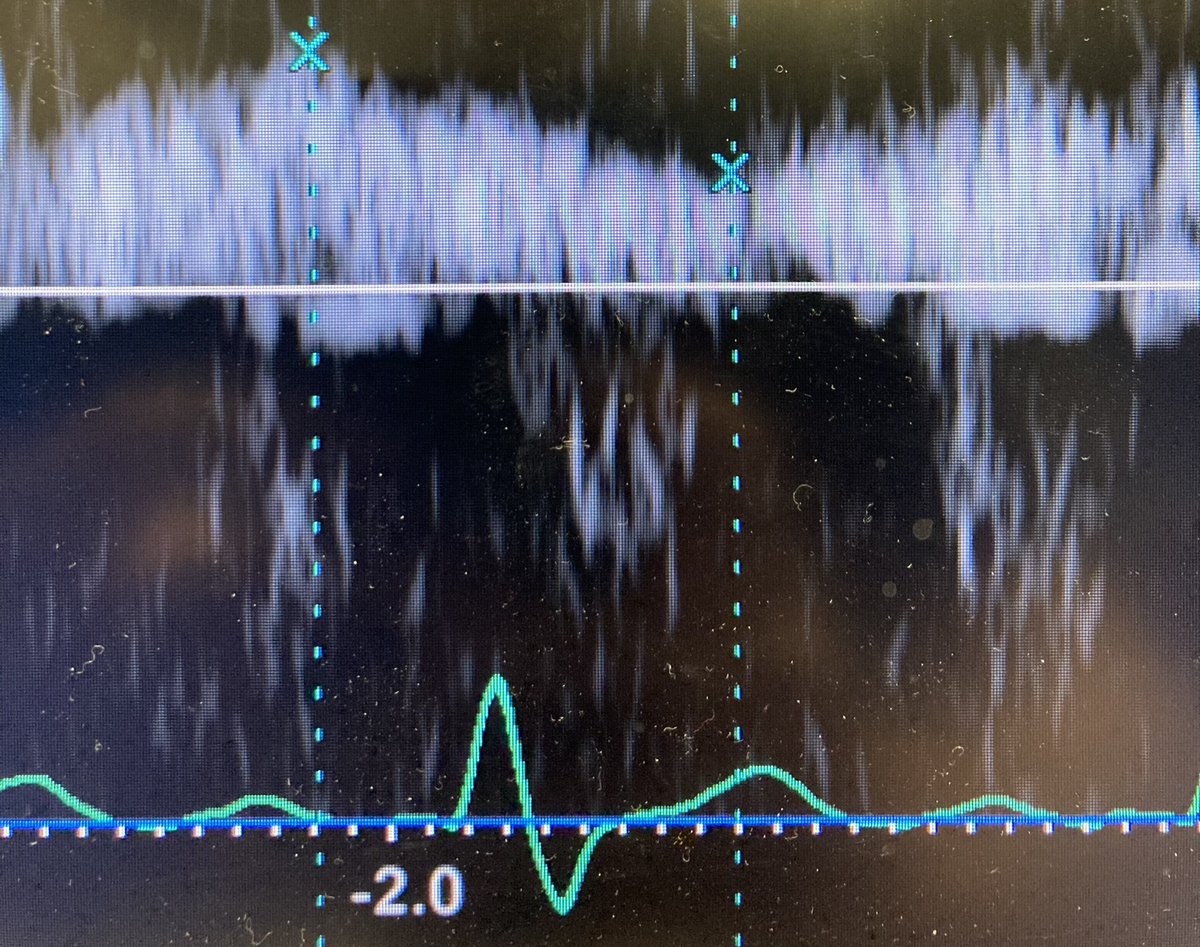
7/ Here are the new right sided findings: Note the RVOT VTI has lost the midsystolic notch and is increased to 22.4. VExUS is grade 2 with S wave now with forward flow, and PV PPI 0.53. The septal shift is now reversed. There was a R pleural effusion noted.
8/ ECG: NRS now with the same RBBB & LAFB.
9/ So when the patient was shocked, there seemed to be a cardiogenic shock (due to ⬇️HR, SV preserved), and RV/PA uncoupling from elevated PVR. This seems to have completely resolved after potassium was corrected and HR/BP normalized.
10/ So a couple points: 1) hemodynamics are often a moving target and it is important to take a second look when things are done or things have changed. 2) In a sick patient, no inferences should be made about baseline cardiac function when not sick.
11/11 Finally, I’d be interested in comments on this patient’s changes in hemodynamic profile. I thought it was quite interesting for things to change so much with only potassium treatment.
Loading suggestions...