

How do you titrate your PEEP in moderate to severe ARDS Patients?
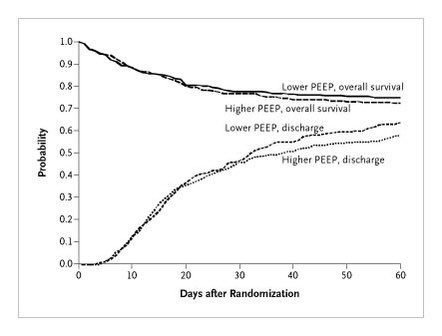
2004 alveoli trial
DOI: 10.1056/NEJMoa032193
549 Pts.
TV ~ 6 ml/kg
Pplat (24-27)
Low PEEP 8.3±3.2 cmh2o (death 24.9%)
High PEEP 13.2±3.5 cmh2o (death 27.5%)
Result= no significant difference between high or low PEEP
DOI: 10.1056/NEJMoa032193
549 Pts.
TV ~ 6 ml/kg
Pplat (24-27)
Low PEEP 8.3±3.2 cmh2o (death 24.9%)
High PEEP 13.2±3.5 cmh2o (death 27.5%)
Result= no significant difference between high or low PEEP
2008 ~ LOVS trial
JAMA. 2008;299(6):637-645
983 PTs
TV ~ 6 ml/kg
CG: Pplat<30, low PEEP mortality 40.4%
IG: Pplat <40, high PEEP ~ mortality 36.4%
The high PEEP group had lower rates of refractory hypoxemia (4.6% vs 10.2%)
JAMA. 2008;299(6):637-645
983 PTs
TV ~ 6 ml/kg
CG: Pplat<30, low PEEP mortality 40.4%
IG: Pplat <40, high PEEP ~ mortality 36.4%
The high PEEP group had lower rates of refractory hypoxemia (4.6% vs 10.2%)


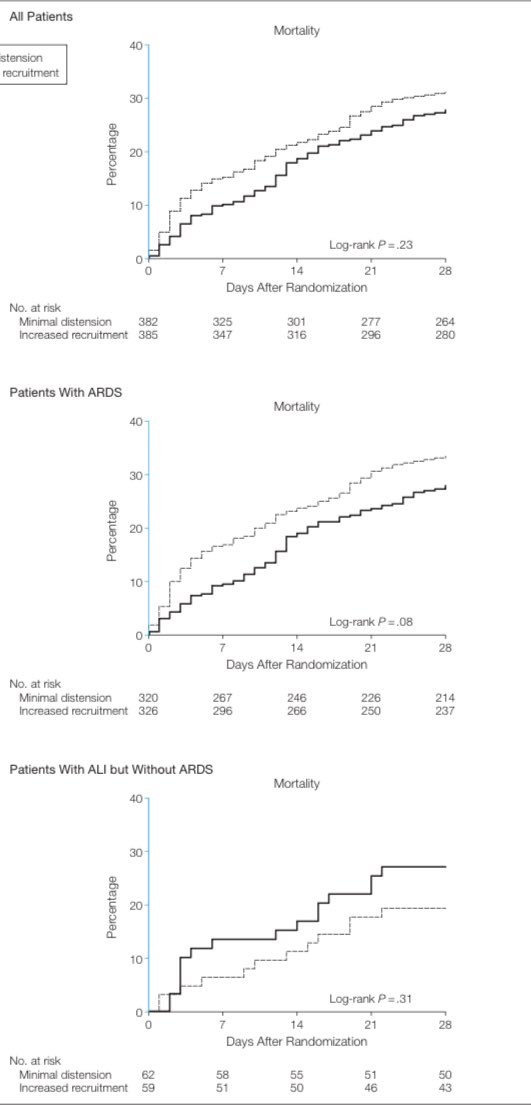
2008 EXPRESS Trial
JAMA. 2008;299(6):646-655
767 Pts.
TV ~ 6 ml/kg
CG: PEEP 5-9 cm H2O
IG: PEEP titrated to reach Pplat 28 to 30.
No Mortality difference
JAMA. 2008;299(6):646-655
767 Pts.
TV ~ 6 ml/kg
CG: PEEP 5-9 cm H2O
IG: PEEP titrated to reach Pplat 28 to 30.
No Mortality difference
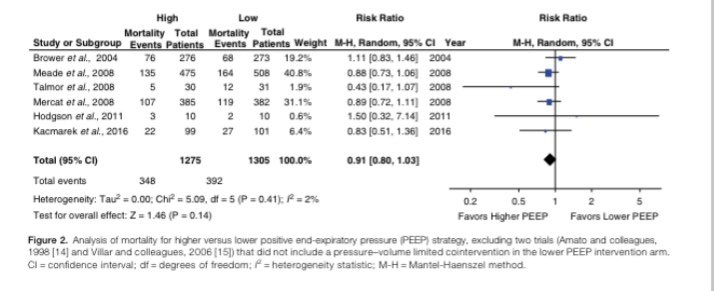
2017 meta-analysis
http://10.0.5.233/AnnalsATS.201704-338OT
6 trials
No mortality difference, but in subgroup analysis in moderate to severe ARDS high PEEP showed trend toward improve outcome
http://10.0.5.233/AnnalsATS.201704-338OT
6 trials
No mortality difference, but in subgroup analysis in moderate to severe ARDS high PEEP showed trend toward improve outcome
BuT WAiT WhatS aBoUt OxygenAtiOn?
There is better oxygantion with higher PEEP
There is better oxygantion with higher PEEP
2022 network Meta-analysis
Jose Dianti et al. Am J Respir Crit Care Med. 2022.
18 RCT
4646 Pts
Conclusion;
In patients with moderate to severe ARDS, higher PEEP without lung recruitment maneuver is associated with a lower risk of death than lower PEEP.
Jose Dianti et al. Am J Respir Crit Care Med. 2022.
18 RCT
4646 Pts
Conclusion;
In patients with moderate to severe ARDS, higher PEEP without lung recruitment maneuver is associated with a lower risk of death than lower PEEP.

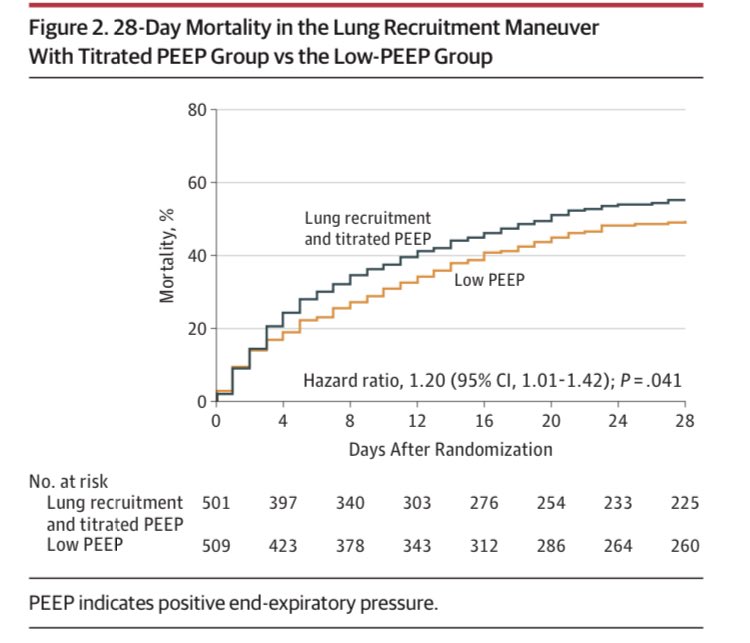
A higher PEEP with prolonged lung recruitment maneuver (LRM) strategy is associated with increased risk of death when compared with higher PEEP without LRM.
What is Prolonged LRM?
ART trial in JAMA
2017
1010 Pts
PEEP 25 ➡️ 1 minute, ➡️ 35 cm H2O ➡️ 1 minute, ➡️ 45 ➡️ 2 minutes. After recruitment, decremental PEEP titration was started
PEEP 23 in VC mode. PEEP levels were decreased in steps of 3 down to a minimum of 11. ⬇️⬇️⬇️
ART trial in JAMA
2017
1010 Pts
PEEP 25 ➡️ 1 minute, ➡️ 35 cm H2O ➡️ 1 minute, ➡️ 45 ➡️ 2 minutes. After recruitment, decremental PEEP titration was started
PEEP 23 in VC mode. PEEP levels were decreased in steps of 3 down to a minimum of 11. ⬇️⬇️⬇️
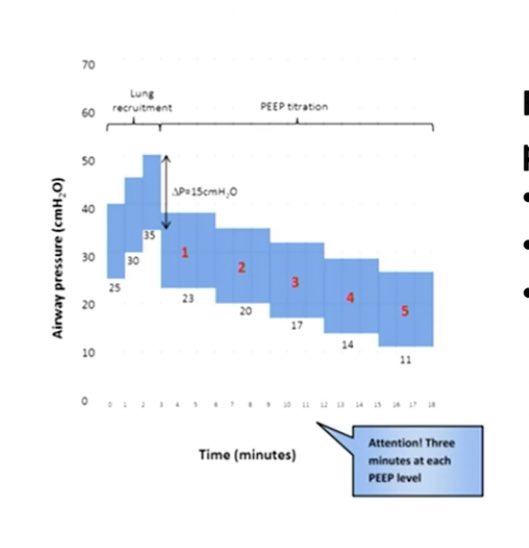
After 4 minutes in each step, The PEEP associated with the best compliance plus 2 cm H2O was considered the optimal PEEP.
This is what I gathered for prolonged LRM
🛑 don’t do it
This is what I gathered for prolonged LRM
🛑 don’t do it
Titrating PEEP according to the Ppeak and Pplat if increase the PEEP by 2 cmh2o and the Ppeak and Pplat goes up by 1 or stays the same ➡️ this indicate recruitment but if the Pplat goes up at the same ratio or higher ➡️ indicates overdistention
What’s about titrating the PEEP according to driving pressure = Pplat - PEEP keep it < 15?
As Cstatic = TV/(Pplat-PEEP) we can say DP = TV/Cstatic
2015 N Engl J Med 2015;372:747-55.
DOI: 10.1056/NEJMsa1410639
Stated that ⬇️ DP were strongly associated with increased survival
As Cstatic = TV/(Pplat-PEEP) we can say DP = TV/Cstatic
2015 N Engl J Med 2015;372:747-55.
DOI: 10.1056/NEJMsa1410639
Stated that ⬇️ DP were strongly associated with increased survival
Retrospective studies showed that each unit increase of driving pressure (1 cmH2O) was associated with a 5% increment in mortality 🥴😵💫
How we reduce the DP
Adjust the PEEP and TV
How we reduce the DP
Adjust the PEEP and TV
Small studies showed titrating the PEEP to reduce DP has trend towards improving survival (small trials)

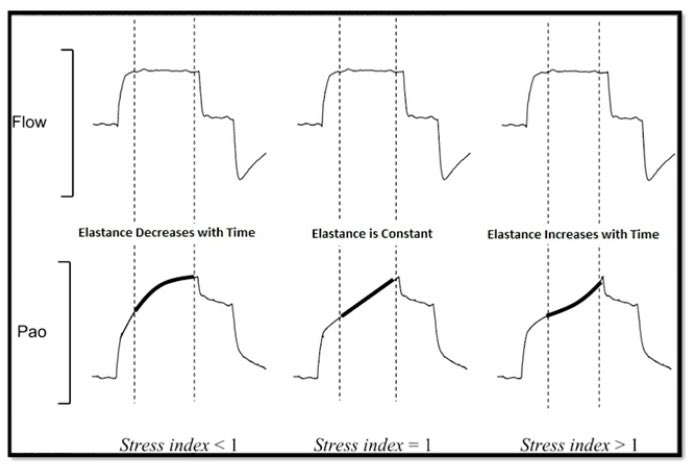
What’s about Stress Index
When you use the stress index you have to use VC-CMVs square flow. Which it can help you with to titrating TV and PEEP if < 1 you can increase your parameters and re-evaluate. If > 1 there is higher risk of Barotrauma and volumetrauma, if 1 (optimal)
When you use the stress index you have to use VC-CMVs square flow. Which it can help you with to titrating TV and PEEP if < 1 you can increase your parameters and re-evaluate. If > 1 there is higher risk of Barotrauma and volumetrauma, if 1 (optimal)
N Engl J Med 2008;359:2095-104.
Esophageal Ballon to measure the transpulmonary pressure and titrate PEEP according to the Transpulmonary pressure the target pressure is 0 to 10 cm of water at end expiration that showed improvement in oxygenation
Esophageal Ballon to measure the transpulmonary pressure and titrate PEEP according to the Transpulmonary pressure the target pressure is 0 to 10 cm of water at end expiration that showed improvement in oxygenation
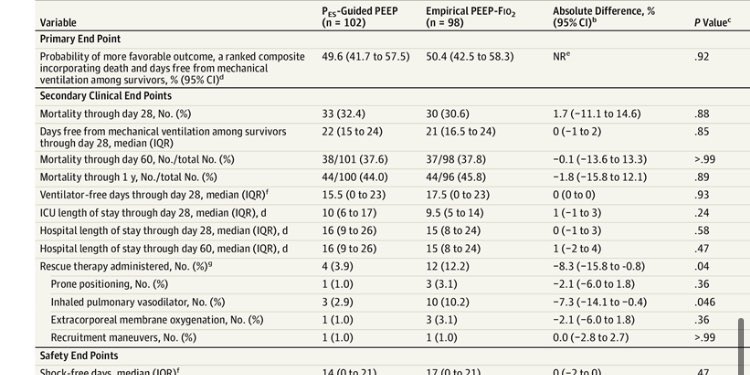
2019 in JAMA
doi:10.1001/jama.2019.0555
PEEP titration guided by PES measurement, compared with empirical high PEEP-Fio2 titration, resulted in no significant difference in a composite outcome that incorporated death and days free from mechanical ventilation
doi:10.1001/jama.2019.0555
PEEP titration guided by PES measurement, compared with empirical high PEEP-Fio2 titration, resulted in no significant difference in a composite outcome that incorporated death and days free from mechanical ventilation
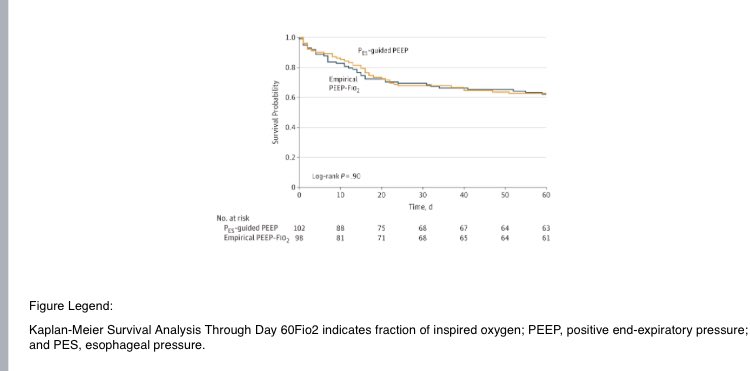
Titrating PEEP with esophageal balloon should less need for rescue maneuver compared to empirical titration.
In Summary PEEP titration should be individualized according to the disease severity, Pt lung mechanics.
Personally I use all the above methods except for the esophageal balloon I use it in morbid obese pt with refractory hypoxemia.
Thank you
Personally I use all the above methods except for the esophageal balloon I use it in morbid obese pt with refractory hypoxemia.
Thank you
What method do you use to adjust PEEP in cases of severe ARDS?What are your thoughts?
Loading suggestions...