

ICU milestones: It was 23 years ago today, May 4th 2000, when @NEJM published one of the most influential studies in Critical Care (CC): the Acute Respiratory Distress Syndrome Network (ARDSNet) trial, sometimes referred to as the ARMA trial:

Roy Brower, Michael Matthay, Alan Morris, David Schoenfeld, Taylor Thompson & Arthur Wheeler were the members of the writing committee. ARMA compared traditional ventilation w tidal volume (Vt) of 12 ml/kg of predicted body weight (PBW) & an airway pressure measured after a
0.5-sec end-inspiratory pause (plateau pressure; Ppl) of ≤50 cm H2O, with ventilation w a lower Vt of 6 ml/kg of PBW & a Ppl of ≤30 cm H2O. The trial was stopped early, after the 4th interim analysis & enrollment of 861 patients;
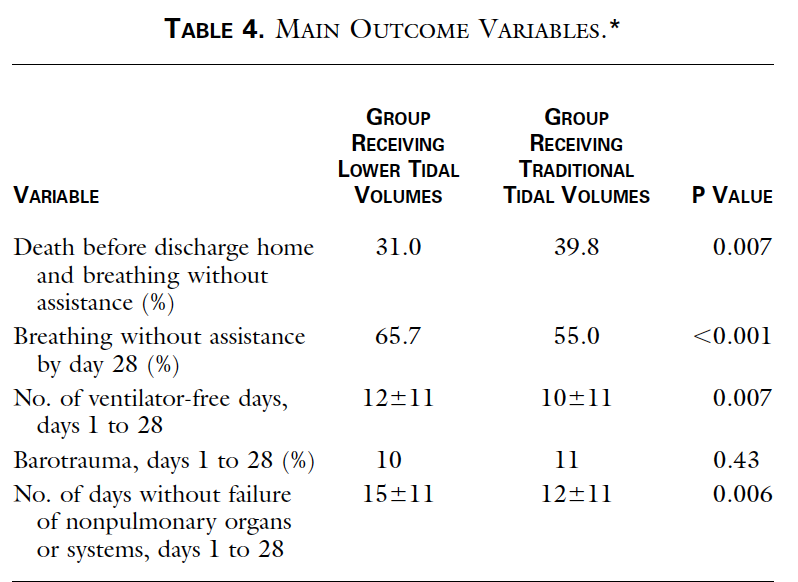
mortality was lower in the lower Vt group than in the traditional Vt group (31.0% vs 39.8%; P=0.007), and the number of ventilator-free days during the first 28 d after randomization was greater in this group (12±11 vs 10±11; P=0.007) 👇
Pts were recruited (03/1996-03/1999) at 10 university centers of the ARDSNetwork. The volume-assist-control mode was used until the pt was weaned from the vent or for 28 d post-randomization. Because normal lung vol is predicted on the basis of sex/height, PBW was calculated for
each pt. In the traditional Vt group, initial Vt was 12 ml/kg PBW. This was later ⬇️ stepwise by 1 ml/kg if needed to keep Ppl ≤50 cm H2O. In the low Vt group, Vt ⬇️ to 6 ml/kg within 4 hrs post-randomization & later ⬇️ stepwise by 1 ml/kg if necessary to keep Ppl ≤30 cm H2O.
Minimal Vt was 4 ml/kg PBW. If Ppl ⬇️ <25 cm H2O, Vt was ⬆️ by 1 ml/kg until Ppl ≥25 cmH2O or Vt was 6 ml/kg. For pts w severe dyspnea, Vt could be ⬆️ to 7-8 ml/kg if Ppl stayed ≤30 cm H2O. If ⬆️ in the vent rate were not adequate, HCO3 drips were allowed to correct pH of <7.15
I ❤️ this study. Not only because CC is plagued by “negative” trials & this was a hugely positive one. Have you noticed that nowadays any study showing absolute mortality risk reduction > 3-4% raises eyebrows? ARMA found ARR ~ 9%. You had to treat 11 pts in order to save 1 life.
Not even because it had ripple effects beyond the way we ventilate pts (stay tuned: I'll return to this point). I ❤️ it because it took a simple, bold approach & studied a basic, non-pharmacologic intervention (low vs high Vt) & not a fancy drug; no xyz35wthmycin versus placebo…
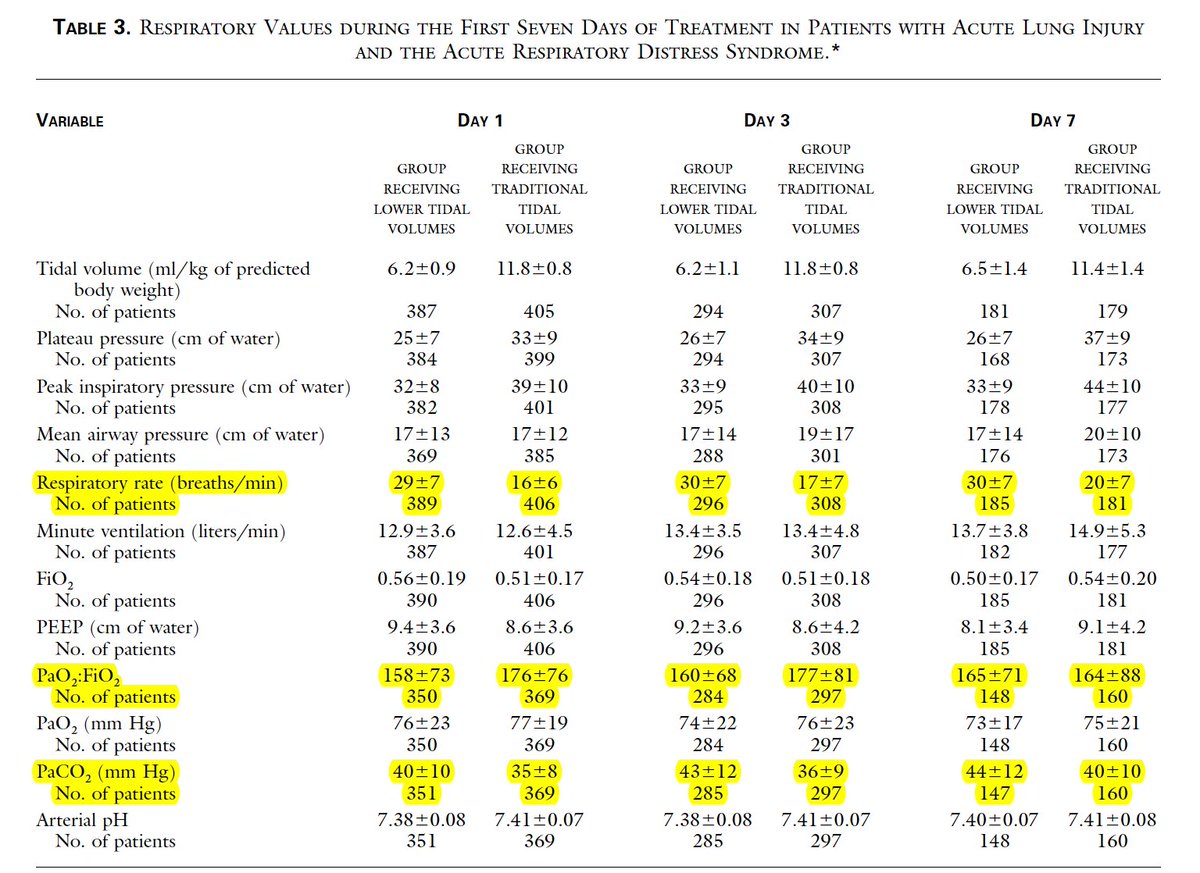
More importantly, it challenged the orthodoxy of aiming "normal" blood gases; in fact, the low Vt group had worse oxygenation, higher pCO2 & higher respiratory rates (30 vs 17!) 👇
As happens often in our specialty, ARMA was not free of controversy. For many yrs later, I was reading commentaries about how “ethically problematic” it was, because it failed to include a control group representative of current practice. Eichacker expressed 2 additional concerns
1. Many pts were randomized to a Vt (6 or 12 ml/kg PBW) that was substantially lower or higher than their pre-randomization (& supposedly “individualized”) Vt,
2. In order to minimize risks to study subjects, a “best current practices” control group should have been included
2. In order to minimize risks to study subjects, a “best current practices” control group should have been included
The ARDSNet investigators claimed among others that there was no real standard of care for ventilation of ARDS pts & that the Vts of 6 & 12 ml/kg were “consistent with contemporary opinion & within the scope of routine care” 👇. The controversy over the ARDSNet trial
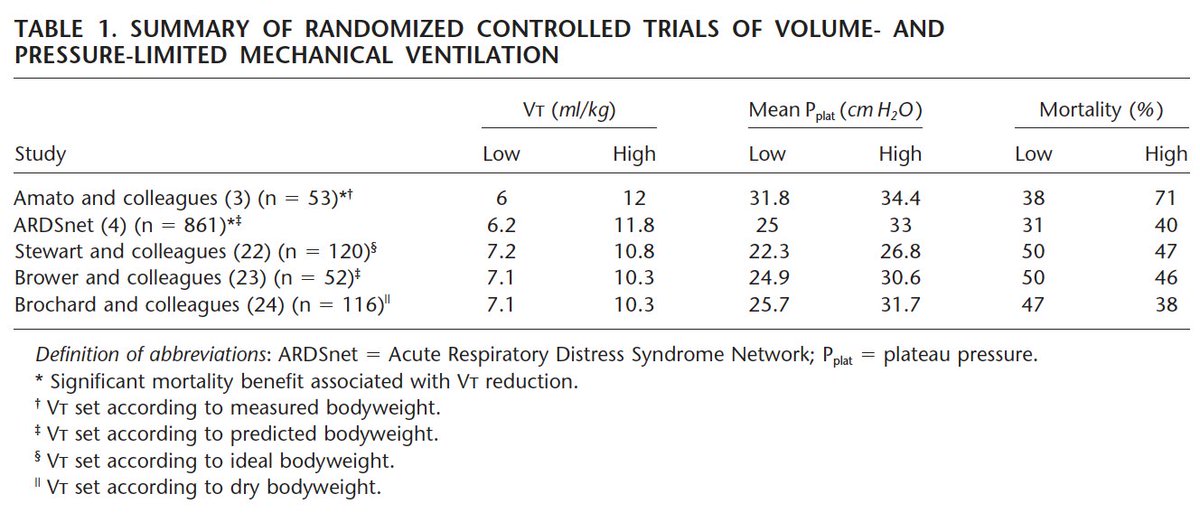
gave the scientific community the opportunity to re-evaluate the trade-offs between explanatory (efficacy) & pragmatic (effectiveness) trials. The former try to determine whether a treatment effect exists & therefore focus on maximizing internal validity. The latter try to
determine whether the intervention works in routine clinical practice & therefore focus on maximizing external validity (ie, generalizability). ARMA was an explanatory trial & slow to be broadly adopted even among the ARDS Network centers...
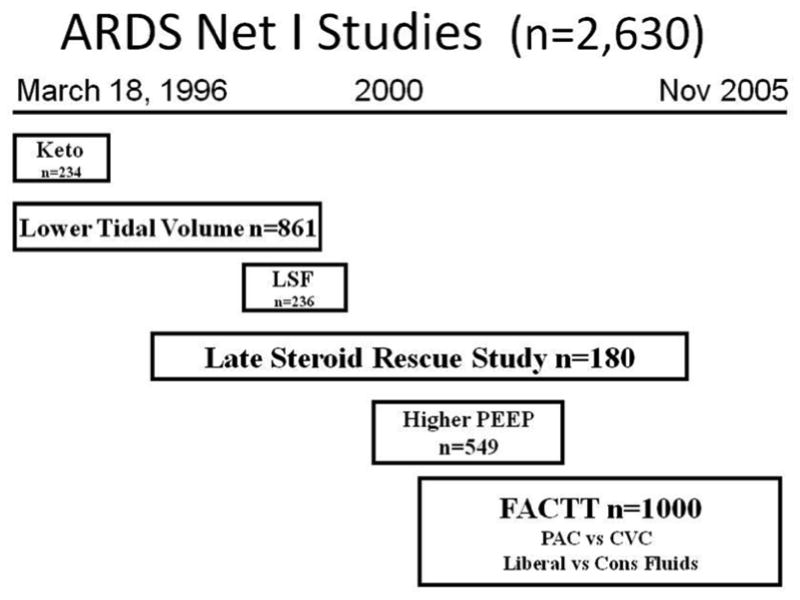
ARDS Network gave us several RCTs, before & after ARMA. For example, SAILS, ALTA & EDEN-OMEGA are not included here 👇. PETAL network built on the strengths & accomplishments of the ARDSNet. More on PETAL 23 yrs from now (if I happen to read a study the day it was published...)
Thanks for reading!
References:
1. pubmed.ncbi.nlm.nih.gov
2. pubmed.ncbi.nlm.nih.gov
3. pubmed.ncbi.nlm.nih.gov
4. pubmed.ncbi.nlm.nih.gov
References:
1. pubmed.ncbi.nlm.nih.gov
2. pubmed.ncbi.nlm.nih.gov
3. pubmed.ncbi.nlm.nih.gov
4. pubmed.ncbi.nlm.nih.gov

pubmed.ncbi.nlm.nih.gov/12406836/
Meta-analysis of acute lung injury and acute respiratory distress syndrome trials testing low tidal volumes - PubMed
Meta-analysis of acute lung injury and acute respiratory distress syndrome trials testing low tidal...

pubmed.ncbi.nlm.nih.gov/15616401/
The acute respiratory distress syndrome network controversy: lessons and legacy - PubMed
The controversy related to and the impact of the Acute Respiratory Disease Syndrome Network clinical...

pubmed.ncbi.nlm.nih.gov/10793162/
Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome - PubMed
In patients with acute lung injury and the acute respiratory distress syndrome, mechanical ventilati...

pubmed.ncbi.nlm.nih.gov/21742211/
ARDS Network (NHLBI) studies: successes and challenges in ARDS clinical research - PubMed
To hasten the development of effective therapy for acute respiratory distress syndrome (ARDS), in 19...
Loading suggestions...