

1/7
H PYLORI AND IRON DEFICIENCY
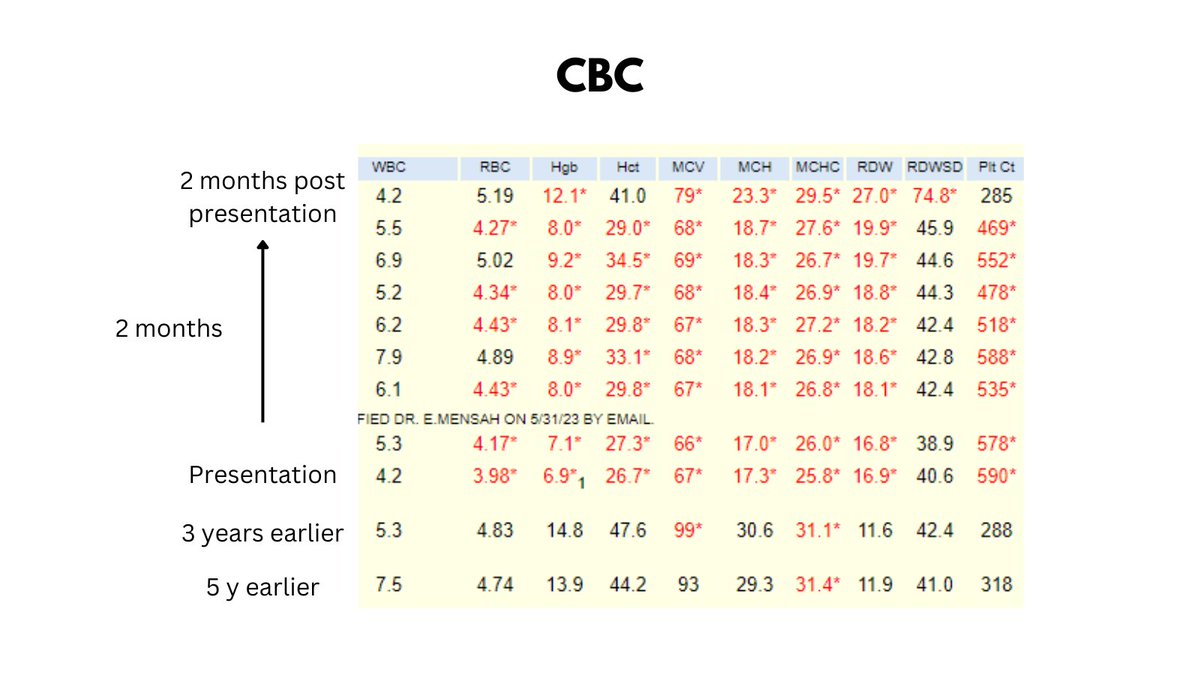
Saw a young previously healthy 36 yo male who presented with 2 month history of lower abdominal cramping and was found to have iron deficiency anemia with secondary thrombocytosis (CBCs shown in graphic, ferritin < 5).
H PYLORI AND IRON DEFICIENCY
Saw a young previously healthy 36 yo male who presented with 2 month history of lower abdominal cramping and was found to have iron deficiency anemia with secondary thrombocytosis (CBCs shown in graphic, ferritin < 5).
2/7
GI work up revealed evidence of gastritis, and stomach biopsy surface bacteria morphology was c/w H. pylori. Stool antigen was positive for H. pylori. Screen for Celiac's was negative.
GI work up revealed evidence of gastritis, and stomach biopsy surface bacteria morphology was c/w H. pylori. Stool antigen was positive for H. pylori. Screen for Celiac's was negative.

3/7
He was treated with quadruple therapy consisting of bismuth subsalicylate, metronidazole, tetracycline, and a PPI given for 14 days along with ferrous sulfate 325 mg daily. His GI symptoms improved, as did his Hb and ferritin levels.
He was treated with quadruple therapy consisting of bismuth subsalicylate, metronidazole, tetracycline, and a PPI given for 14 days along with ferrous sulfate 325 mg daily. His GI symptoms improved, as did his Hb and ferritin levels.
4/7
About as clear cut a case of H pylori-associated ID as I have ever seen!
Some learning points:
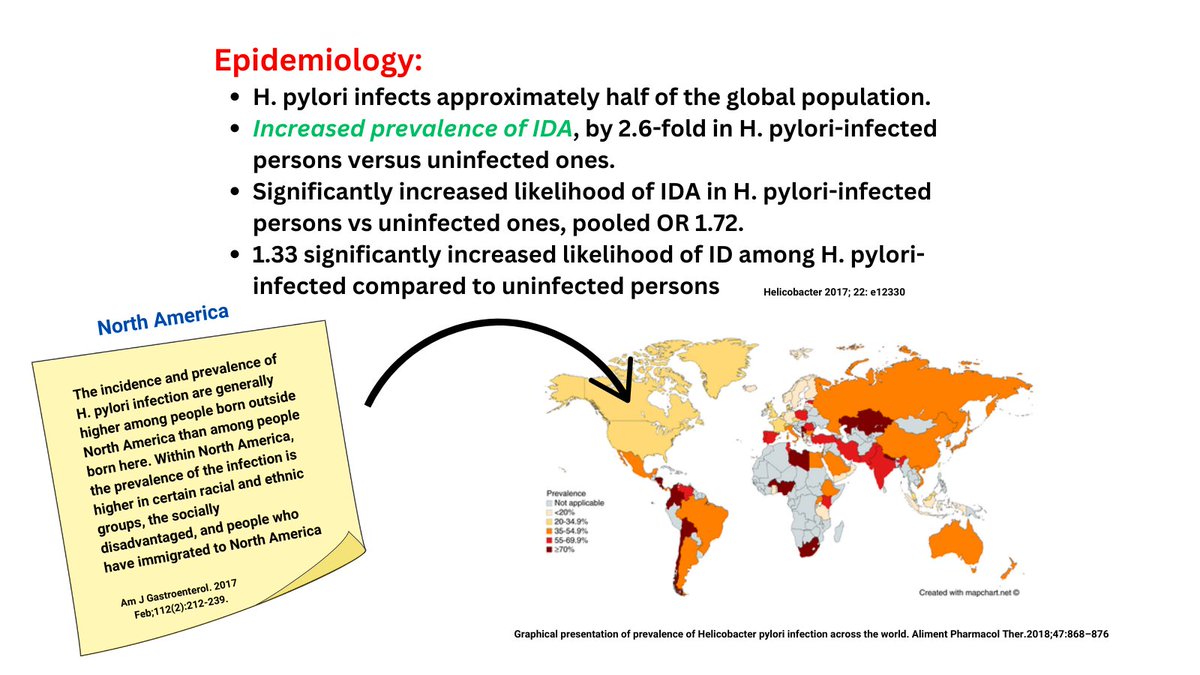
1. H pylori infection VERY common, though less prevalent in North America than in many parts of the world.
2. H pylori infection is associated with increased risk of ID.
About as clear cut a case of H pylori-associated ID as I have ever seen!
Some learning points:
1. H pylori infection VERY common, though less prevalent in North America than in many parts of the world.
2. H pylori infection is associated with increased risk of ID.
5/7
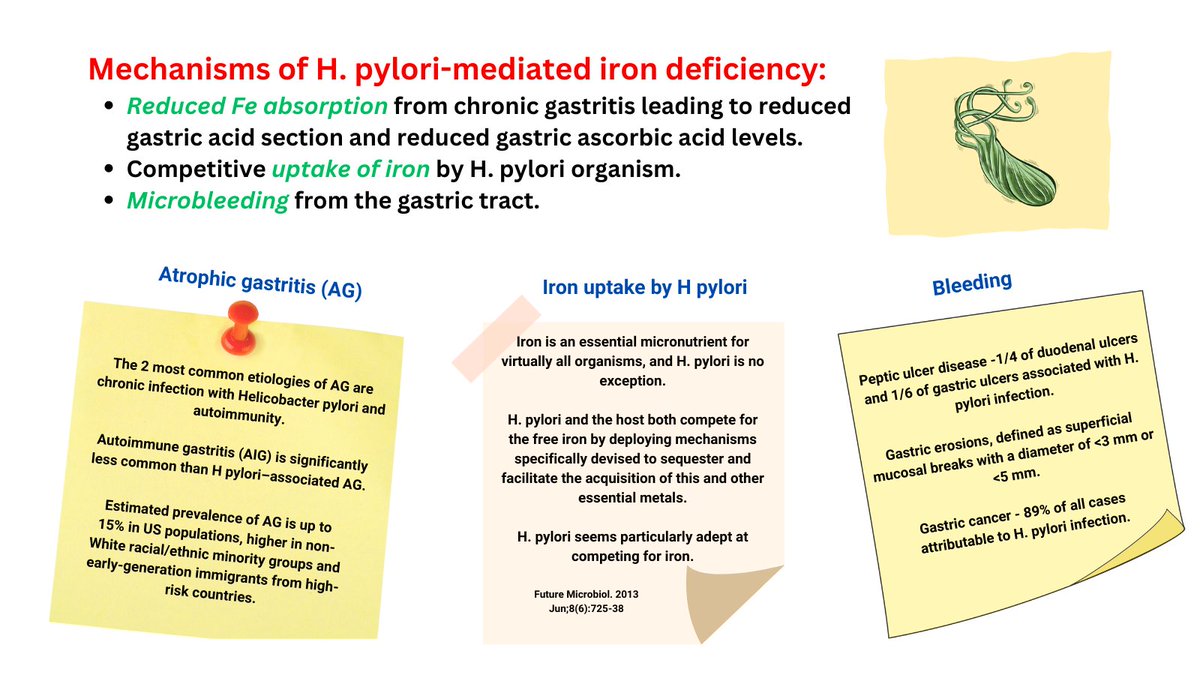
3. Mechanisms of ID in patients with H pylori infection include:
a. Achlorhydria from gastritis (less conversion of ferric to ferrous form of Fe).
b. Fe uptake by H pylori organisms.
c. Bleeding, especially from stomach erosions.
3. Mechanisms of ID in patients with H pylori infection include:
a. Achlorhydria from gastritis (less conversion of ferric to ferrous form of Fe).
b. Fe uptake by H pylori organisms.
c. Bleeding, especially from stomach erosions.
6/7
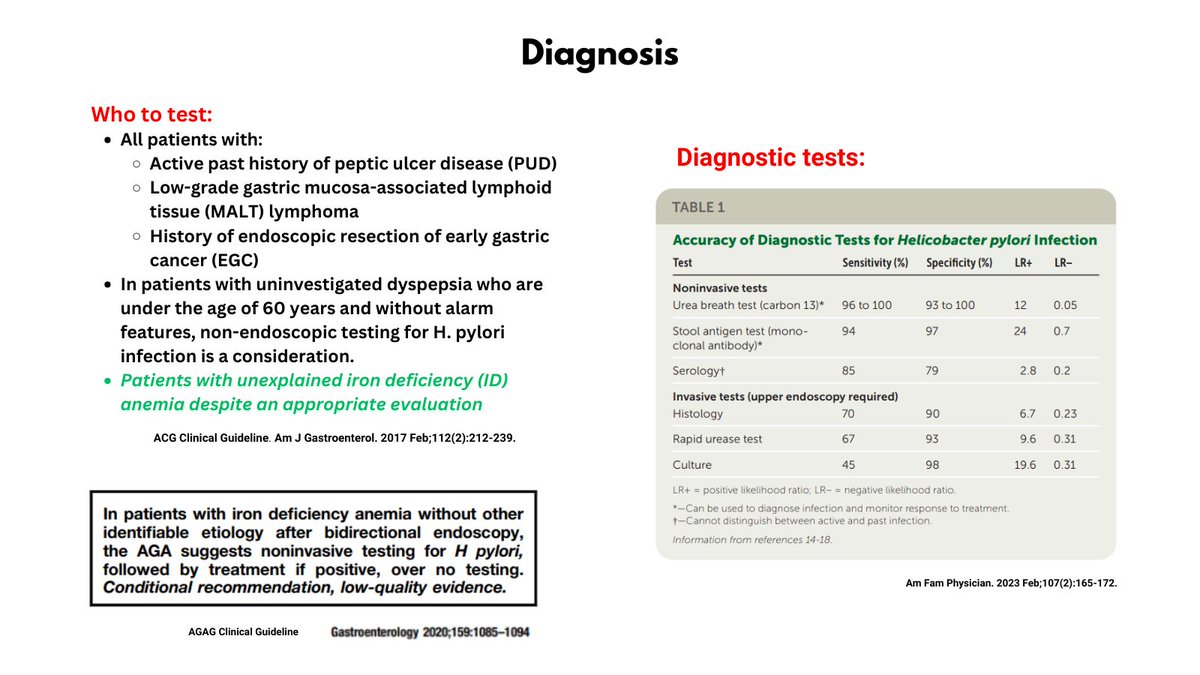
4. Who to test - CGC and AGAG clinical guidelines suggest (non-invasive) testing for H pylori in patients with IDA who have a negative workup, including bidirectional endoscopy.
5. How to test - Urea breath test of stool antigen test.
4. Who to test - CGC and AGAG clinical guidelines suggest (non-invasive) testing for H pylori in patients with IDA who have a negative workup, including bidirectional endoscopy.
5. How to test - Urea breath test of stool antigen test.
7/7
How to treat - outside my wheelhouse, but typically bismuth quadruple therapy. 😀
How to treat - outside my wheelhouse, but typically bismuth quadruple therapy. 😀
Loading suggestions...