

...🧵This is a thread about 8.4% sodium bicarbonate (aka bicarb amp) in critical care.
This the first part in a series of three about sodium bicarbonate 🧂in critical care:
🧐I will get in deep to complexities, benefits, risks and clinical implications of this (overused) drug. x.com
This the first part in a series of three about sodium bicarbonate 🧂in critical care:
🧐I will get in deep to complexities, benefits, risks and clinical implications of this (overused) drug. x.com

Necessary premise: this is a complex, huge and tricky topic, so forgive me if I missed some key points. I did my best in digging deep into my FOAMed references and literature. I hope you enjoy the discussion and share your opinions as well. x.com

8.4% bicarb is available as a 50ml amp in US.
📝8.4% = 84 g/L = 1000 meq/L sodium and 1000 meq/L bicarbonates
📝8.4%= 1 meq/ml = 2000 mOsm/L (highly hypertonic solution roughly equivalent to 6% NaCl!)
Fun fact: In 🇮🇹 8.4% bicarb is available as a 100ml vial x.com
📝8.4% = 84 g/L = 1000 meq/L sodium and 1000 meq/L bicarbonates
📝8.4%= 1 meq/ml = 2000 mOsm/L (highly hypertonic solution roughly equivalent to 6% NaCl!)
Fun fact: In 🇮🇹 8.4% bicarb is available as a 100ml vial x.com
⚠️Risks and side effects.
Mostly, they depend on rapid pH shifts due to rapid amps pushes.
1⃣ Acute paradoxically respiratory acidosis 🫁
Basically, alkalinization occurs as long as (rate or volume) ventilation increases ("open systems") in order to get rid of [...] x.com
Mostly, they depend on rapid pH shifts due to rapid amps pushes.
1⃣ Acute paradoxically respiratory acidosis 🫁
Basically, alkalinization occurs as long as (rate or volume) ventilation increases ("open systems") in order to get rid of [...] x.com
[...] CO2 excess generated by bicarb infusion.
This can be problematic in "closed systems" such as:
👉 🫁 diseases
👉 pts who have maximized the efficiency of their breathing (eg. augmented minute ventilation in DKA)
👉most of all, pts who are not breathing (cardiac arrest💔) x.com
This can be problematic in "closed systems" such as:
👉 🫁 diseases
👉 pts who have maximized the efficiency of their breathing (eg. augmented minute ventilation in DKA)
👉most of all, pts who are not breathing (cardiac arrest💔) x.com
![[...] CO2 excess generated by bicarb infusion.
This can be problematic in "closed systems" such as:...](https://pbs.twimg.com/media/GjXS0O_WUAASqEa.jpg)
2⃣ Paradoxical CSF acidosis🧠
In closed systems an acute CO2 raise can lead to acute (and 🧠symptomatic) CSF acidosis due to the high (and faster than bicarb) CO2 BBB permeability.
@nickmmark calculated that one bicarb amp cointans roughly 1.16L CO2 😱. x.com
In closed systems an acute CO2 raise can lead to acute (and 🧠symptomatic) CSF acidosis due to the high (and faster than bicarb) CO2 BBB permeability.
@nickmmark calculated that one bicarb amp cointans roughly 1.16L CO2 😱. x.com
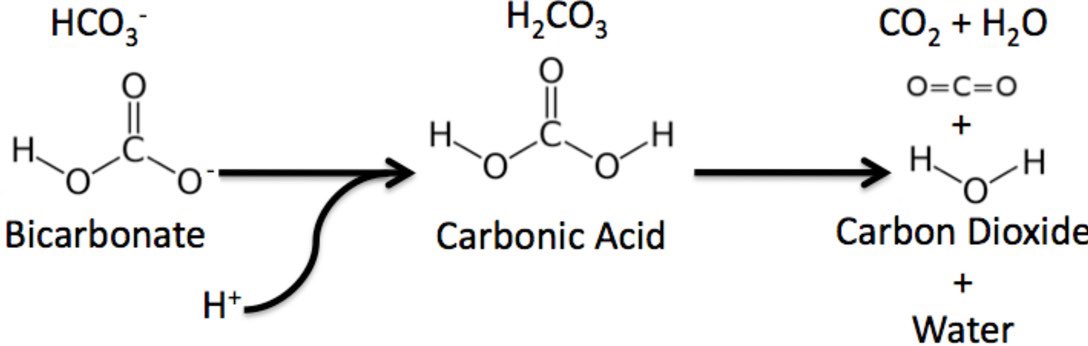
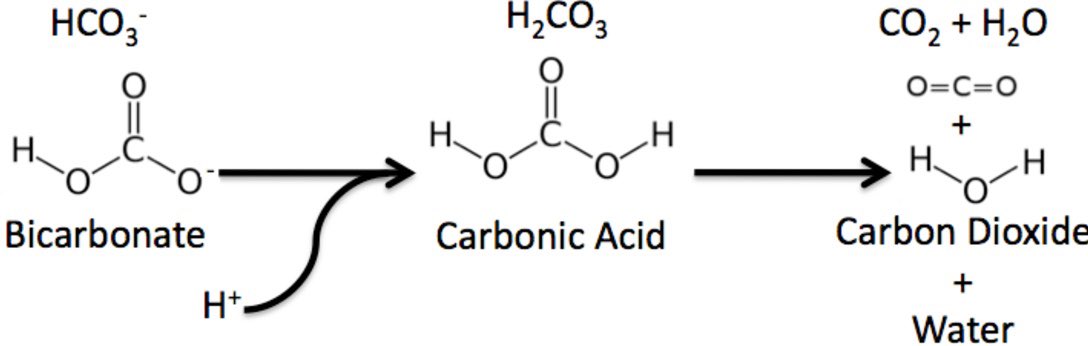
3⃣ Paradoxical intracellular acidosis 🔬
In closed systems CO2 diffuses across cells membranes and combines with intracellular H20 leading to reduction in pH (right to left equation). x.com
In closed systems CO2 diffuses across cells membranes and combines with intracellular H20 leading to reduction in pH (right to left equation). x.com
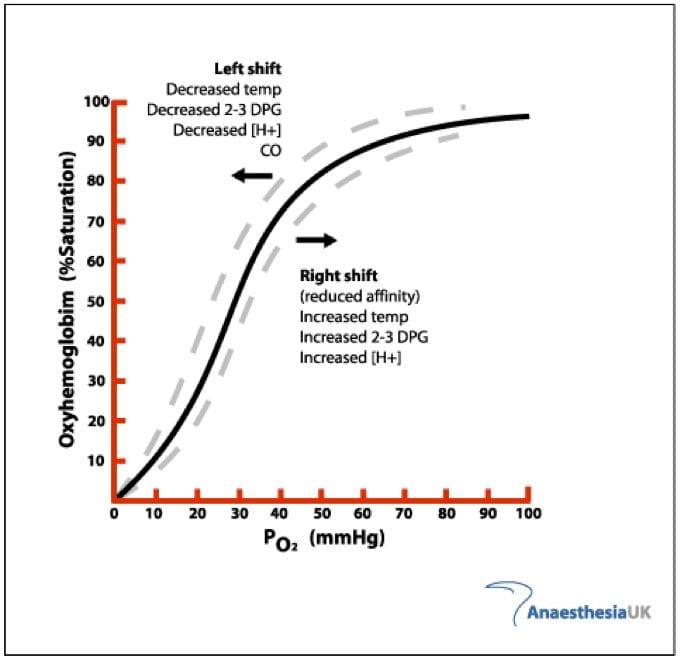
4⃣ Tissue oxygenation impairment 🩸
A rapid increase in pH leads to left shift in the oxygen-hemoglobin dissociation curve, hampering oxygen delivery and potentially generating anaerobic lactate. x.com
A rapid increase in pH leads to left shift in the oxygen-hemoglobin dissociation curve, hampering oxygen delivery and potentially generating anaerobic lactate. x.com
5⃣ Hypocalcemia
A rapid increase in pH can exacerbate a pre-existing mild hypoCa by:
👉augmented Ca-albuming binding by removal of protons stuck to albumin.
👉Ca chelation by bicarb infused.
🛑Hypocalcemia is often an overlooked sodium bicarbonate controindication. 🛑
A rapid increase in pH can exacerbate a pre-existing mild hypoCa by:
👉augmented Ca-albuming binding by removal of protons stuck to albumin.
👉Ca chelation by bicarb infused.
🛑Hypocalcemia is often an overlooked sodium bicarbonate controindication. 🛑
6⃣ Hypernatriemia 🧂
Each 50 ml amp will increase Na by roughly 1 meq📝,
⚠️so it may be used in limited quantities in patients with normonatremia: repeated doses will inevitably cause hypernatremia.
🛑Hypernatremia is always an absolute 8.4% bicarb controindication.🛑 x.com
Each 50 ml amp will increase Na by roughly 1 meq📝,
⚠️so it may be used in limited quantities in patients with normonatremia: repeated doses will inevitably cause hypernatremia.
🛑Hypernatremia is always an absolute 8.4% bicarb controindication.🛑 x.com

7⃣ Volume overload 🌊
The high osmotic load can significantly increase intravascular volume by sudden huge fluids shift.
That’s can be problematic in renal failure and HF patients 🫀.
🛑Hypervolemia is a (relative) sodium bicarbonate controindication.🛑 x.com
The high osmotic load can significantly increase intravascular volume by sudden huge fluids shift.
That’s can be problematic in renal failure and HF patients 🫀.
🛑Hypervolemia is a (relative) sodium bicarbonate controindication.🛑 x.com

8⃣ Metabolic alkalosis
Repeated pushes can lead to alkalosis due to expected bicarb physiological effect (aka pH rise), assuming an open system (otherwise you will probably get little net effect).
🛑Alkalosis is always a sodium bicarbonate controindication.🛑
Repeated pushes can lead to alkalosis due to expected bicarb physiological effect (aka pH rise), assuming an open system (otherwise you will probably get little net effect).
🛑Alkalosis is always a sodium bicarbonate controindication.🛑
🟢Indications🟢
8.4% bicarb is an highly overused medication primarly due to the desire to correct BGA parameters rather than achieving homeostasis by treating the cause of metabolic acidosis. 😶🌫️
✅Highly recommended indications are the following: x.com
8.4% bicarb is an highly overused medication primarly due to the desire to correct BGA parameters rather than achieving homeostasis by treating the cause of metabolic acidosis. 😶🌫️
✅Highly recommended indications are the following: x.com

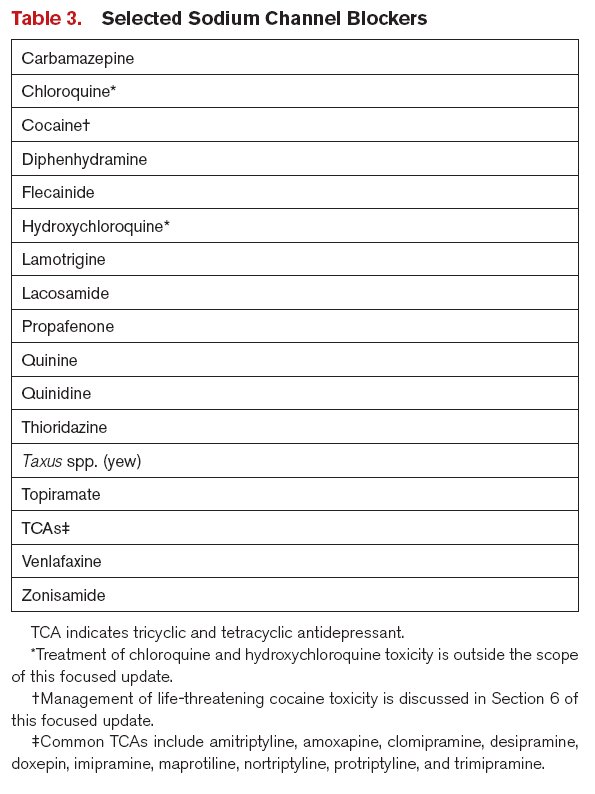
1⃣ Intoxications (eg. salicylates, TCA, cocaine) ☠️
👉Above all 8.4% bicarb is the cornestore (loading) therapy in sodium channel blockers profound overdose and barely the only – strictly proven – related indication for bolusing amps (cardiac arrest). x.com
👉Above all 8.4% bicarb is the cornestore (loading) therapy in sodium channel blockers profound overdose and barely the only – strictly proven – related indication for bolusing amps (cardiac arrest). x.com
2⃣ Emergent treatment of cerebral edema 🧠
👉Hypertonicity and the ready availability make this drug useful in ICP management
👉Roughly 100 ml 8.4% bicarb is a reasonable start
👉Benefit over NaCl 3%: hypertonic saline therapy can lead to NAGMA due to high chloride delivery. x.com
👉Hypertonicity and the ready availability make this drug useful in ICP management
👉Roughly 100 ml 8.4% bicarb is a reasonable start
👉Benefit over NaCl 3%: hypertonic saline therapy can lead to NAGMA due to high chloride delivery. x.com
3⃣ Emergent treatment of acute seizing hyponatriemic patient
👉Similarly, hypertonicity and the ready availability are the golden pros here.
👉8.4% bicarb is twice powerful than NaCl 3%: one amp (50ml) contains 50 meq sodium as nearly those into NaCl 3% 100ml. [...] x.com
👉Similarly, hypertonicity and the ready availability are the golden pros here.
👉8.4% bicarb is twice powerful than NaCl 3%: one amp (50ml) contains 50 meq sodium as nearly those into NaCl 3% 100ml. [...] x.com
[...]
👉2 ml/kg 8.4% bicarb (to make it simple roughly 100-150ml in a normal weight pt) increase sodium by near 2-3 meq 📝
👉Logistical benefit over NaCl 3%: crafting hypertonic saline potions in emergency can be tricky.
emcrit.org x.com
👉2 ml/kg 8.4% bicarb (to make it simple roughly 100-150ml in a normal weight pt) increase sodium by near 2-3 meq 📝
👉Logistical benefit over NaCl 3%: crafting hypertonic saline potions in emergency can be tricky.
emcrit.org x.com


1⃣ Solute drag effect
Increasing plasma tonicity causes cells to shrink leading to increased intracellular potassium: equilibration with serum concentration then causes potassium to leave cells following water.
☹️This is the primary cause of 8.4% bicarb failure in lowering K.
Increasing plasma tonicity causes cells to shrink leading to increased intracellular potassium: equilibration with serum concentration then causes potassium to leave cells following water.
☹️This is the primary cause of 8.4% bicarb failure in lowering K.
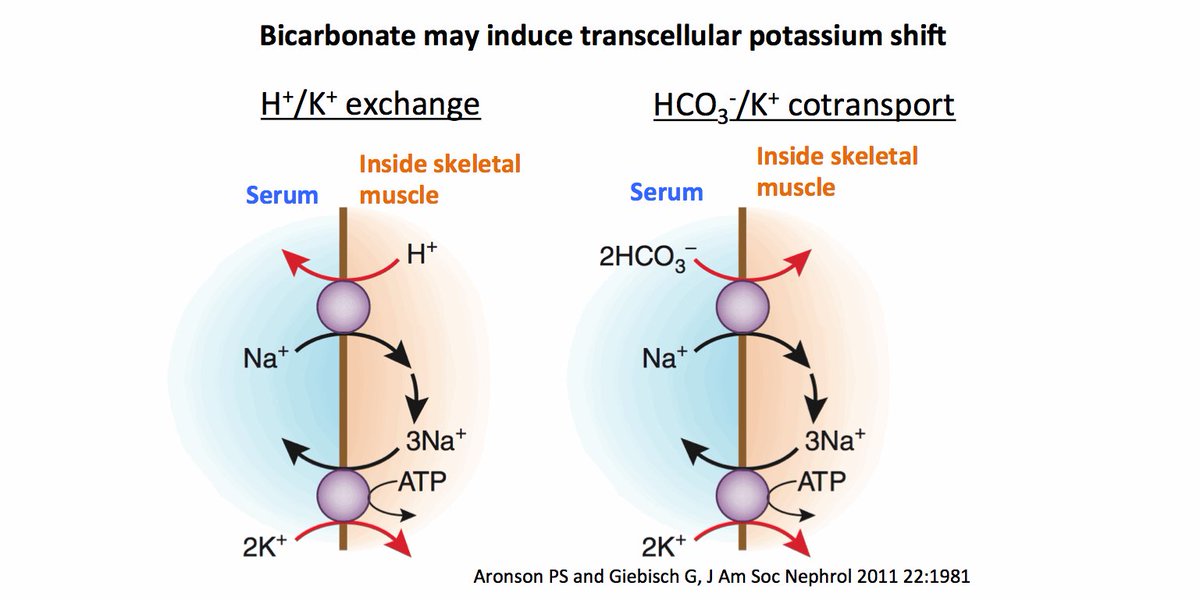
2⃣ pH driven intracellular potassium shift 🔄.
😢Unfortunately this effect is counteracted by the previous one and in addition it appears ineffective in absence of significant metabolic acidosis (more on the next chapter🧵). x.com
😢Unfortunately this effect is counteracted by the previous one and in addition it appears ineffective in absence of significant metabolic acidosis (more on the next chapter🧵). x.com
3⃣ Diluition
Little “K-free fluid” volume is administered, so this effect is negligible.
4⃣ K renal excretion
Largely promoted by alkalosis and also by increased bicarb excretion in urine.
⚠️ It seems to be a delayed effect which may not work in oliguric/anuric pts.
Little “K-free fluid” volume is administered, so this effect is negligible.
4⃣ K renal excretion
Largely promoted by alkalosis and also by increased bicarb excretion in urine.
⚠️ It seems to be a delayed effect which may not work in oliguric/anuric pts.
🔴“NOT TO DO LIST” with 8.4% bicarb amps 🛑
1⃣ Don’t bolus bicarb amps: the potential harms are likely related to the speed of delivery. Ideally amps should be pushed slowly over 15 minutes. x.com
1⃣ Don’t bolus bicarb amps: the potential harms are likely related to the speed of delivery. Ideally amps should be pushed slowly over 15 minutes. x.com

2⃣ Don’t blindly bolus bicarb amps in cardiac arrest (unless toxins suspicion) ❤️🩹
👉no increased survival, actually potential harm: remember the paradoxically acidosis due to "closed system".
🫸 Not routinely recommended by ACLS and AHA guidelines. x.com
👉no increased survival, actually potential harm: remember the paradoxically acidosis due to "closed system".
🫸 Not routinely recommended by ACLS and AHA guidelines. x.com

Thanks to all my twitter guru❤️ @emcrit @ross_prager @PulmCrit @katiewiskar @IM_Crit_ @critconcepts @CriticalCareNow @iceman_ex @Wilkinsonjonny @CritCareTime
Loading suggestions...