

ICU stories: Middle-aged pt w/o significant PMHx presented to the ED on a Friday afternoon w SOB/cough x 2 wks. Vaxed x2 but tested C19(+). BP 120/90, Sat 98% on 2 l/m. ECG: new-onset Afib/HR 140/QTc 500. CXR attached; read as RLL infiltrate. Labs: Na 125, BNP 800 (nl<100),
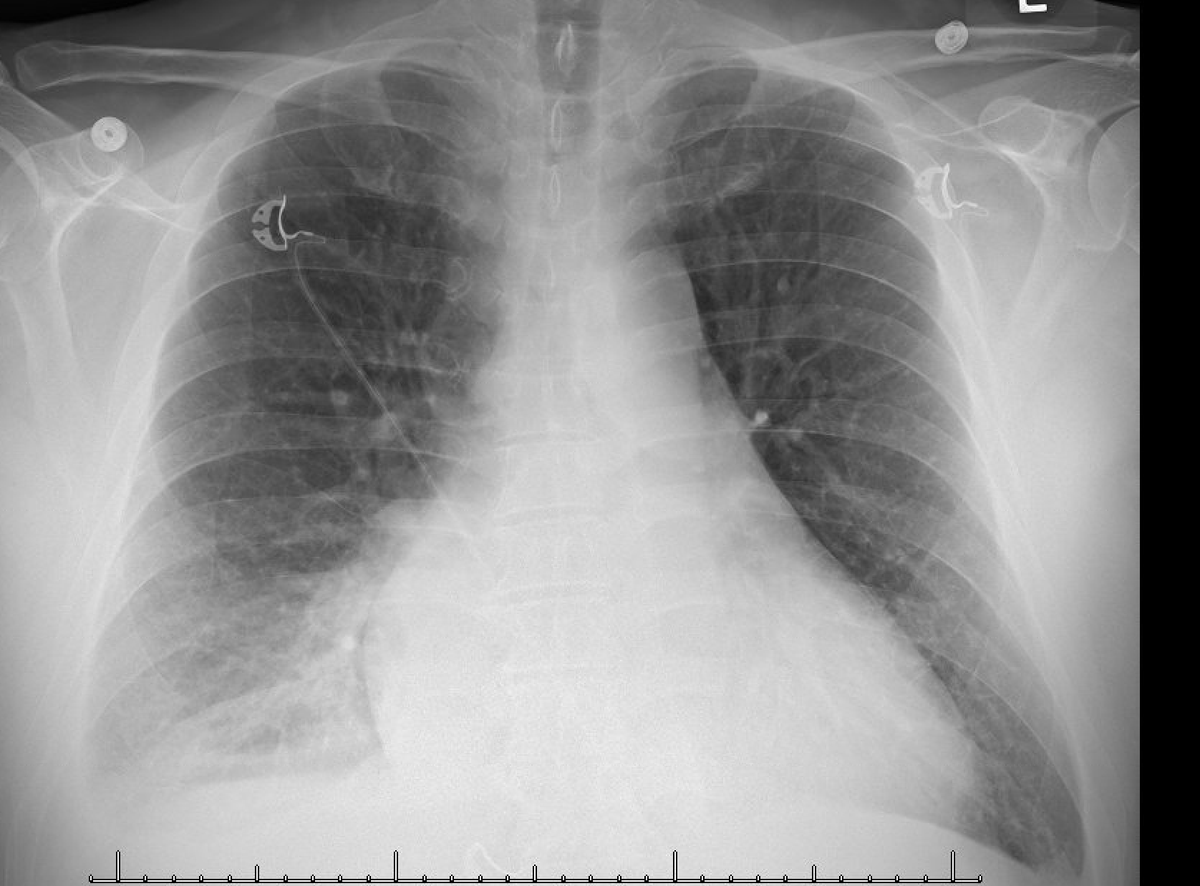
trop 60 (nl<20), BUN/creat 28/1.7 (baseline 10/1.0). Received ivf bolus for sepsis/PNA, antibiotics and diltiazem drip (Cards order). Placed in isolation. Next am Cards stopped ivf & gave Lasix 20 mg iv. UOP was reported poor. Creat ⬆️, Na ⬇️ further, AST/ALT checked & found ⬆️⬆️
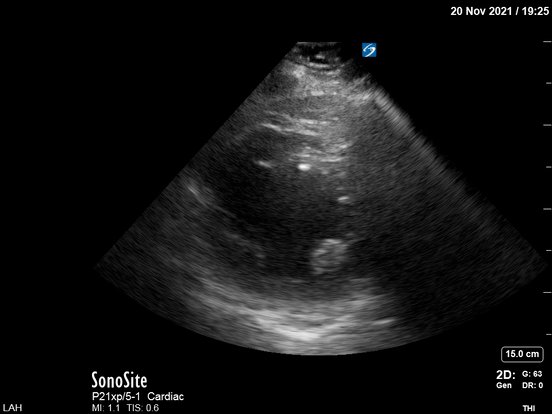
Pt emergently transferred to the ICU. POCUS was done. PLAX:

Obviously there was poor global LV systolic function but just to "play by the book", let's look at another view to confirm the first one. PSAX:
Very difficult 4-chamber view showing an unhappy LV:

Sometimes it's impossible to get good views. Even with US enhancing agent (Definity), Cards could not (later) get a nice view (but ruled out apical clot):
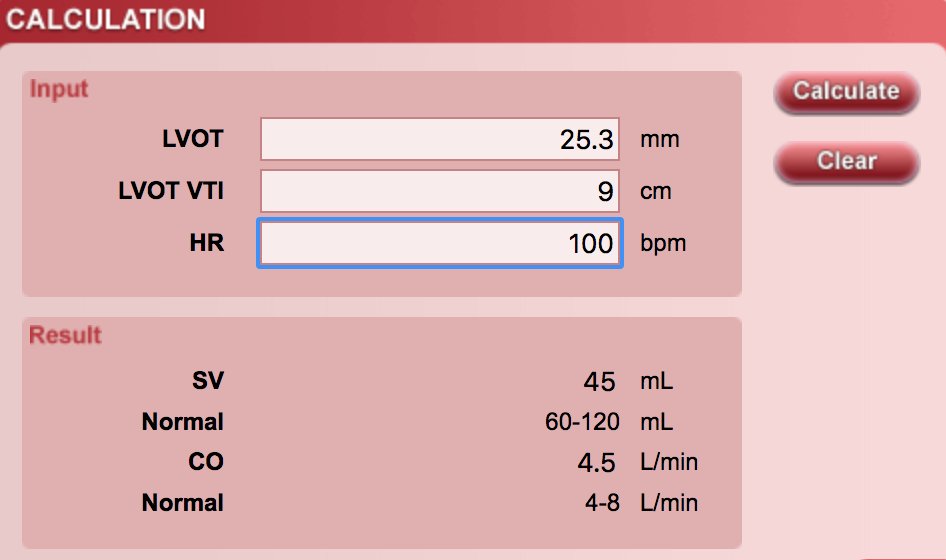
My next step was to measure LVOT VTI. It was around 9 cm (mean value of several beats since pt was in A fib). Nl value: 18-22. The LVOT from a zoomed view:

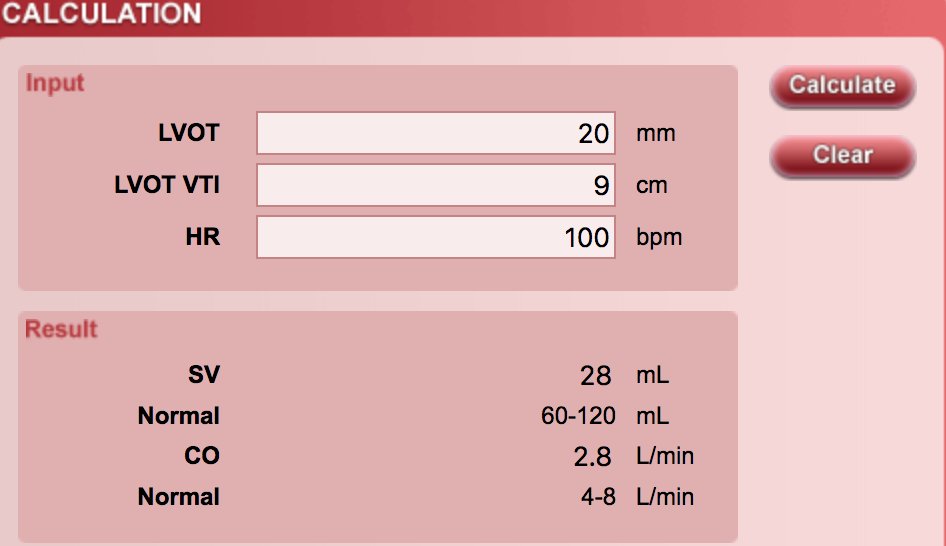
and the LVOT diameter was measured 2.53 cm. Sounds large but it fits w patient's size. Don't assign "2 cm" in every LVOT diameter because sometimes you will make big mistakes
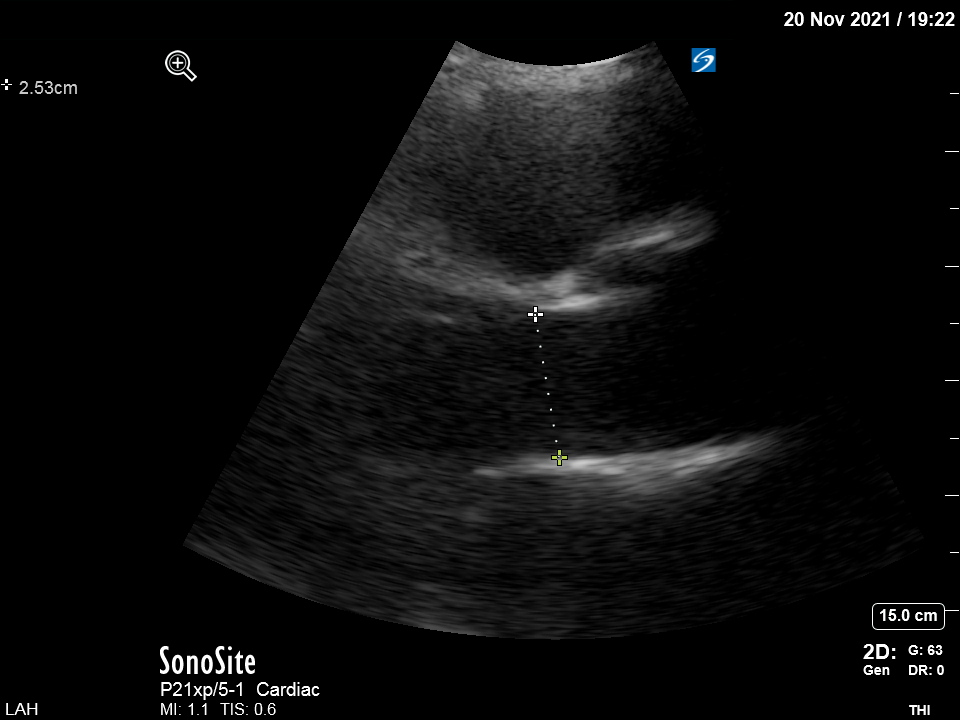
I measured CO 4.5 l/m. If the diameter was blindly set at 2 cm, the CO would be off by 38%...
My next step was to look at the venous side. Pt tachypneic and in A fib (I will skip the poor HV and renal vein Doppler clips). This was the interesting transverse IVC view (at increased depth to look also at the R pleural space):

☝️Full IVC and large R effusion. The admission CXR was read as "no evidence of pleural effusion". This was the chest CT for comparison:

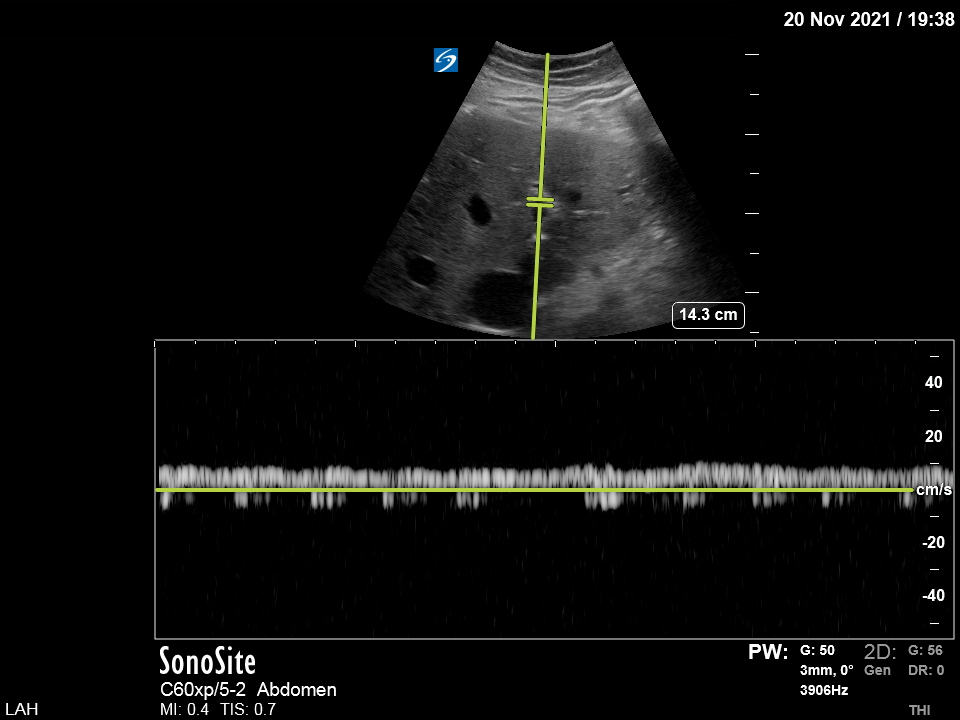
Back to the venous side and VEXUS. The IVC was large (almost 3 cm) but there were no "supportive" HV or renal vein Doppler images

I looked at the portal vein and - to my surprise - there was no pulsatile flow:
Cards (and Renal) learned the POCUS results and asked for inotropic support (dobutamine). I decided to try first a higher Lasix dose (100 mg iv) and re-assess. Pt made 8 liters of urine that night... and was 28 liters negative the next 4 days... Na, creat, AST/ALT improved:
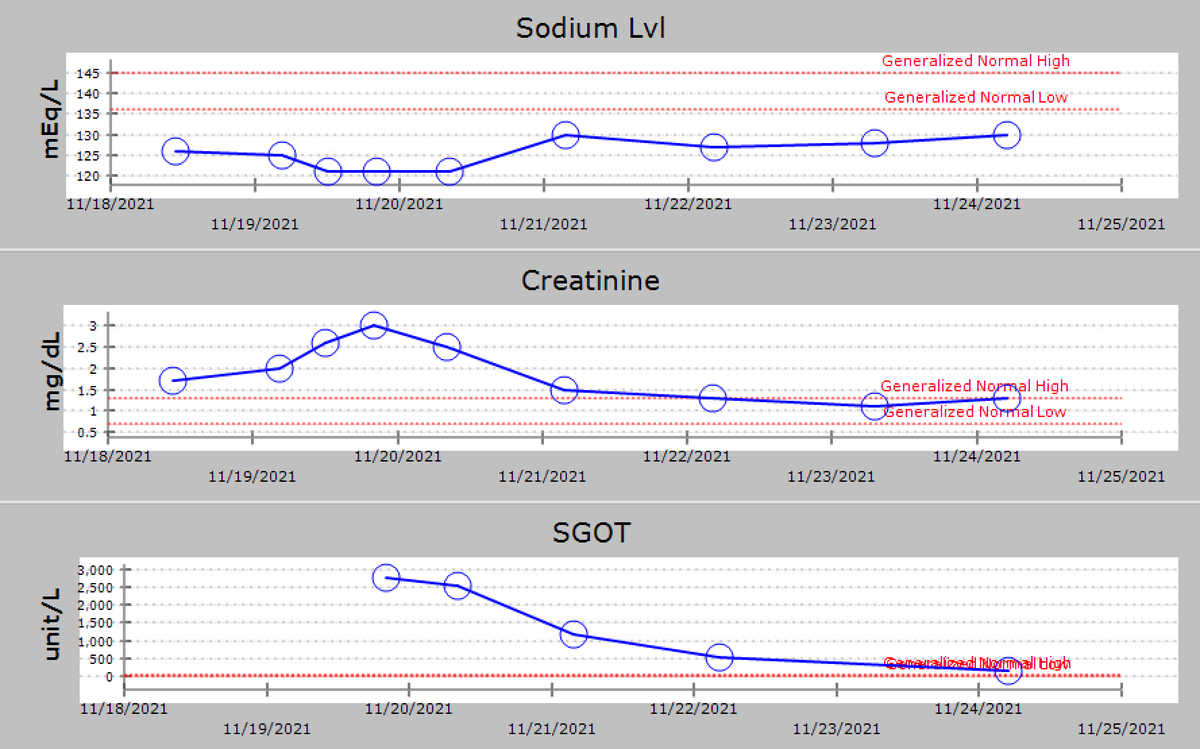
Pt was transferred out of the ICU and a couple of ds later, a cardiac cath showed CO/CI 4.4/1.9. The etiology of CHF is still unclear. GI follow the pt for a newly diagnosed "cirrhosis" probably explaining why portal vein was not pulsatile!
Take-home message:
In cases of poor LV systolic function w organ hypoperfusion, there is usually an urge to use inotropes/vasodilators to increase “forward flow”. In some of these cases a trial of high doses of iv diuretic can make the trick without need for advanced hemodynamic
In cases of poor LV systolic function w organ hypoperfusion, there is usually an urge to use inotropes/vasodilators to increase “forward flow”. In some of these cases a trial of high doses of iv diuretic can make the trick without need for advanced hemodynamic
monitoring (besides POCUS +/- A line). Sometimes in pts w renal dysfunction, neurohormonal maladaptive mechanisms come into play & lead to increased Na reabsorption, decreased H2O clearance, and diuretic resistance (all three probably shown in this case). If/when diuretics start
to work, you may see impressive diuresis (nurses say that pt "opened up"…). I guess a combination of some decongestion in the venous side and improvement of forward flow by blunting of sympathetic activation may increase renal perfusion and diuresis
As always, this was just one way to manage this patient and there may be better ways than mine!
Thanks for reading!
Thanks for reading!
I decided to write this case tonight after reading a thread from @NephroP @ArgaizR @ThinkingCC @critconcepts @Rajiv_sinavan. Thank you!
I used the csecho.ca for the CO calcs. Thank you!
I used the csecho.ca for the CO calcs. Thank you!
Loading suggestions...