

ICU stories (from the trenches): 70 yo pt w hx of A-fib/CAD/ICM w EF 25%/VT ablation s/p BiV ICD/CKD/HTN/HLD/peripheral vasc dz/COPD etc presented to outside 🏥 w SOB/weakness/falls. Labs: wbc 15k/creat 3.5 (baseline 2.0)/INR: 8.5/AST/ALT/Tbil: 180/250/3.0, lactate 3.5



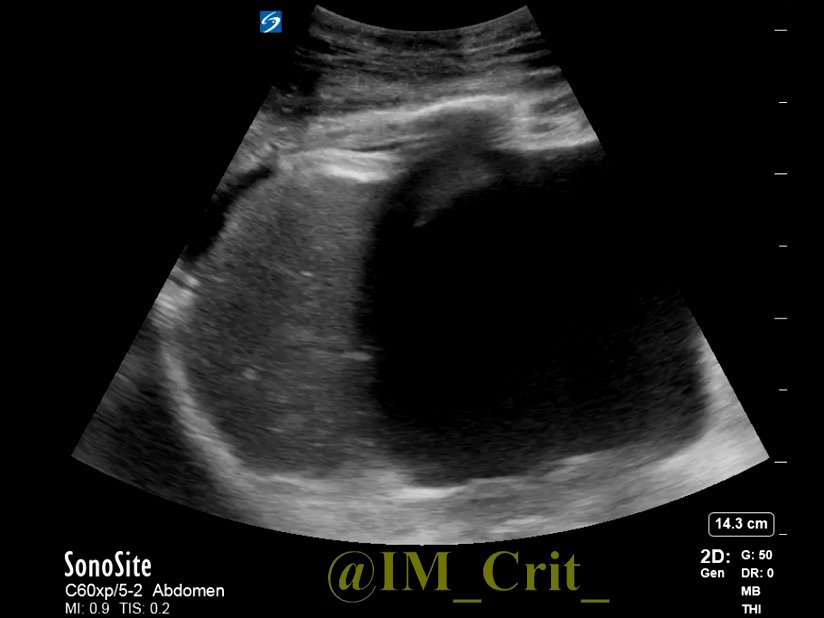
RUQ US was obtained to work-up elevated LFTs:

Diagnosed w bilateral PNA/AKI/liver dysfunction. Treated for sepsis w ivf boluses, broad-spectrum antibiotics, steroids, bicarb. Continue to get worse; due to ⬆️O2 needs, transferred to our 🏥. I saw her the next am: in resp distress while on BiPAP 15/10-100%, abg 7.26/50/70/19.
Confused-restless, hr 70 (paced), bil rales, CRT 6 sec. Skin images follow:




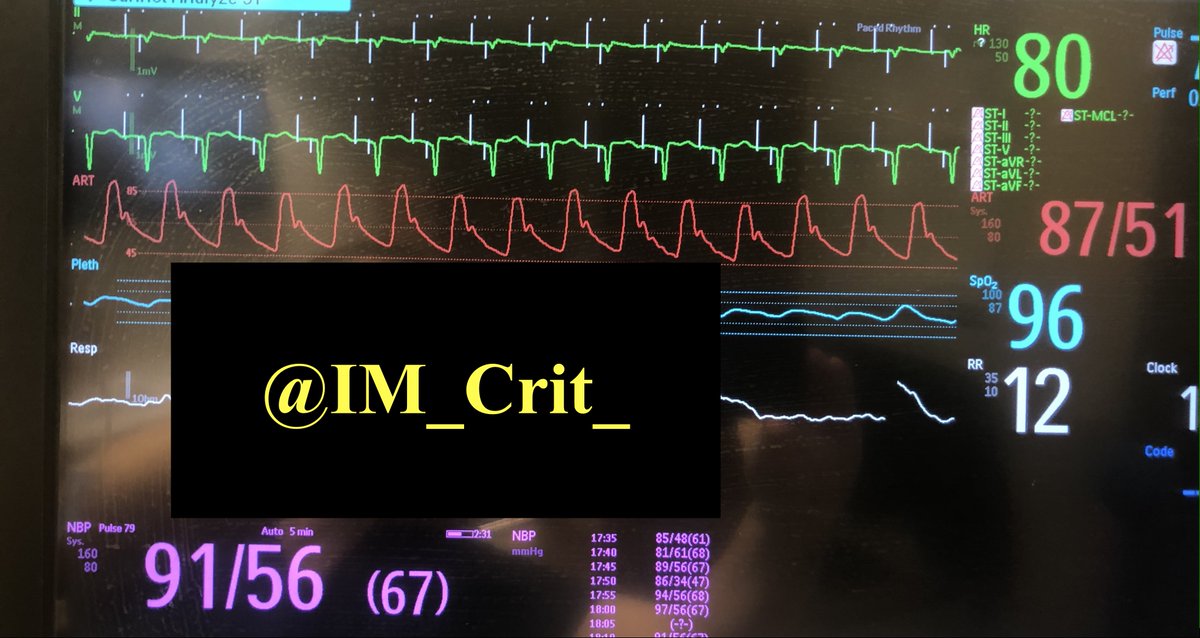
Despite horrible blood gases, rising lactate (5.0) and physical exam as above, BP was "OK"

Pt was DNR/DNI & per previous documentation, she did not want "heroic interventions". Family could not be reached by 📞. What would be your next step?
Pt was too confused/restless to give any information. But more data might be helpful in clarifying what we were dealing with. So, POCUS was performed:
There were bilateral diffuse B-lines, bilateral pleural effusions, a dilated-round IVC, dilated HVs, & a pulsatile PV. HV wihout ecg (sorry!) looked interesting! Intrarenal vein Doppler was tough since pt was breathing too fast; only 1 image was captured (monophasic pattern)




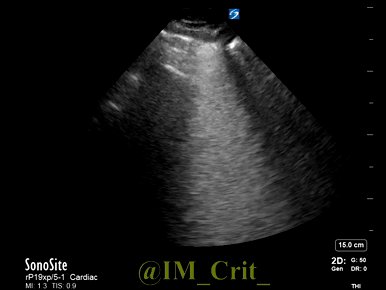
Besides obvious venous congestion & lung congestion, it would be helpful to have an idea about LV/RV function. Remember the calcified LV aneurysm? This degraded any 4ch & LVOT VTI attempts. So, subcostal 4ch, 2ch and RVOT VTI for the win:
Cardiac output was estimated at 2.8 l/min (CI 1.8). But, was it poor global LV systolic function or there was something "bad" going on "in front of" the RV as well? Zoomed view included:
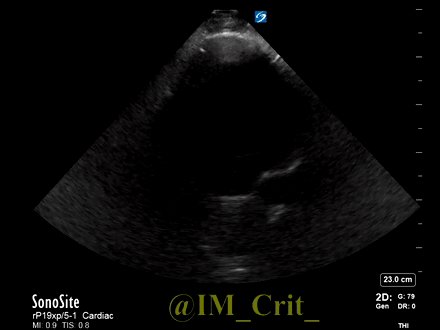
Without any additional US data (no TV or MV resp variation could be obtained), do you think there is pericardial tamponade or just a pericardial effusion?
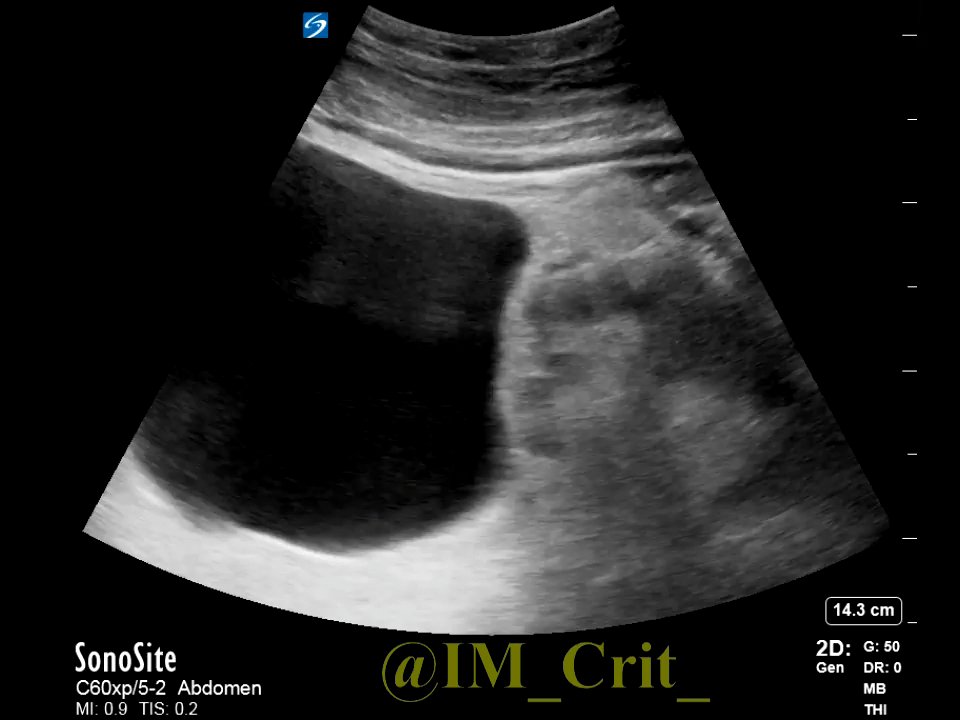
This was ascites, not a pericardial effusion (or tamponade). It's a common pitfall in the subcostal view. Knowing that you are dealing with ascites, you take a look at the L side of the abdomen, at the level of the xiphoid, and you see this hypoechoic area under the spleen:
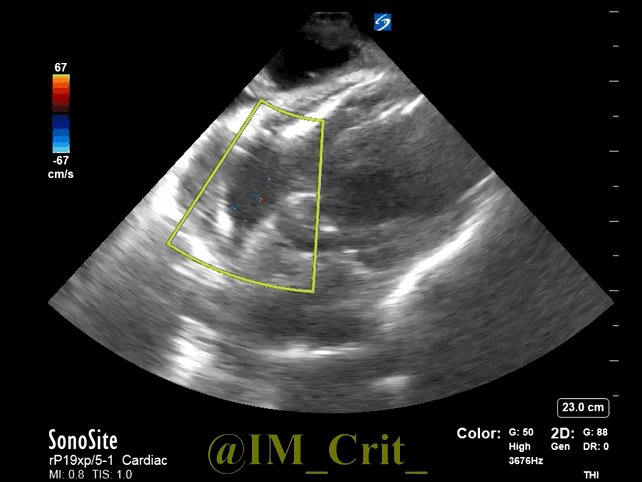
Assuming interventions were permitted, what would you place next?
Better do nothing, since this is a huge L renal cyst:
Having gathered a good amount of data regarding pt's hemodynamics and avoiding some pitfalls, I just placed a brachial arterial line. Pt seemed to be in low-flow state w L and R sided congestion. Estimated CO was 2.8 l/min (CI 1.7). If you could choose one infusion, it would be:
I chose a vasodilator (nitro drip) since I wanted to increase the cardiac output without whipping the heart. Two hours later, mean BP was 10 mmHg lower but CO was up by 15%
and skin looked much better:




If you noticed, pt was paced at 80. During POCUS, pacer was interrogated by a technician. I took advantage of his visit and thinking that pt was most likely in a low flow state, the safe bet would be to increase the pacing rate (instead of decreasing or keeping it the same)... 🤷♂️
Unfortunately, 40 mg of Lasix led to only 200 cc of urine. Doubling the dose and adding a dose of diuril was followed by a diuresis of 1 l

The ADVOR trial (N Engl J Med 2022; 387: 1185-1195
DOI: 10.1056/NEJMoa2203094) has showed that the addition of acetazolamide to a loop diuretic in pts with acute decompensated heart failure results in a greater incidence of successful decongestion. Would you give it here?
DOI: 10.1056/NEJMoa2203094) has showed that the addition of acetazolamide to a loop diuretic in pts with acute decompensated heart failure results in a greater incidence of successful decongestion. Would you give it here?
I did not (not on day 1, at least). Even though ADVOR reported zero cases of severe metab acidosis, this was defined as HCO3 <12. My patient had a bicarb of 19 and mixed resp/metab acidosis, so I thought that further decrease of HCO3 by acetazolamide would make her more acidotic
In the next 2 days, CXR cleared more and BP improved. Lactate normalized. LFTs returned to normal. Creat began to decrease. Patient today is on 5 l/min O2 and wants us to "try for the best". Looks like a different person


Take-home messages:
1. Normotensive cardiogenic shock is quite common. This was a typical case
2. Vasodilators -and not necessarily inotropes- can be all that is necessary to improve hemodynamics
3. Manipulating the microcirculation remains one of the holy grails in Critical Care
1. Normotensive cardiogenic shock is quite common. This was a typical case
2. Vasodilators -and not necessarily inotropes- can be all that is necessary to improve hemodynamics
3. Manipulating the microcirculation remains one of the holy grails in Critical Care
In a landmark study 20 y ago, Spronk et al infused 0.5 mg of nitroglycerin iv in pts w septic shock & found marked increase in microvascular flow. This study did not lead to a major breakthrough but if you look closely, you will find cases where NTG has this microvascular effect

4. Even though the awareness of hemodynamic AKI is increasing, the entity of congestive hepatopathy usually remains unrecognized. Patients receive RUQ US & serial LFTs without us paying attention to their hemodynamic profile. Please notice that the initial RUQ US had signs of
venous congestion but there was no comment in the report to "alert" the primary team. We have to recognize it more often (DOI 10.5152/dir.2020.19673)
PS: Yes, all are real cases. I have to pick a few interesting points each time, otherwise each case would go on for ever...
For those asking, this is a nice, free access review on microcirculation
hindawi.com
hindawi.com
Loading suggestions...